Page 13 of 24
OG30.1 | PCOS — SDL Guide
Learning Objectives
- Describe the Rotterdam 2003 diagnostic criteria for PCOS and explain why it is a diagnosis of exclusion
- Explain the pathophysiology of PCOS, including the roles of insulin resistance, hyperinsulinaemia, and androgen excess
- Select and interpret appropriate investigations for a patient presenting with suspected PCOS
- Outline a tiered management plan for PCOS, including lifestyle measures, medical therapy, and ovulation induction
- Identify the long-term complications of PCOS and plan appropriate surveillance
INSTRUCTIONS
Polycystic ovary syndrome (PCOS) is the most common endocrine disorder in women of reproductive age, affecting 8-13% of women globally. It is a leading cause of anovulatory infertility, menstrual irregularity, and androgen excess. Because PCOS has heterogeneous presentations and overlaps with other endocrine disorders, accurate diagnosis requires systematic application of the Rotterdam criteria and exclusion of mimics. This module equips you to recognise PCOS in a clinical encounter, apply the diagnostic framework confidently, and counsel patients about their management options and long-term health risks.
References
- DC Dutta's Textbook of Gynaecology, 8th ed., Ch. 27 (textbook)
- Shaw's Textbook of Gynaecology, 17th ed., Ch. 25 (textbook)
- ESHRE International Evidence-Based Guideline for PCOS, 2023 (guideline)
- Legro RS et al. Clomiphene, Metformin, or Both for Infertility in PCOS. NEJM 2007; 356:551-566 (journal)
- Legro RS et al. Letrozole vs. Clomiphene for Infertility in PCOS. NEJM 2014; 371:119-129 (journal)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Riya, a 22-year-old final-year medical student, comes to the gynaecology outpatient department worried because she has not had a menstrual period in three months. She mentions her cycles have always been irregular — sometimes coming every six weeks, sometimes every three months. On examination you notice mild acne along her jawline and some coarse hair on her upper lip. Her BMI is 27 kg/m². She asks nervously, 'Could I have PCOS, doctor? My cousin has it and she took years to get pregnant.' Before you answer, you need to apply a structured diagnostic framework, order the right tests, and explain what this diagnosis means for her present and future health.
WHY THIS MATTERS
PCOS affects 8-13% of women of reproductive age — making it one of the most common endocrine conditions you will encounter in both general practice and specialist gynaecology clinics. It is the single largest cause of anovulatory infertility and a major driver of metabolic disease in young women. Understanding PCOS matters because it sits at the intersection of reproductive medicine, endocrinology, and metabolic health: a woman diagnosed with PCOS at 22 may face fertility challenges at 28, develop diabetes at 38, and carry elevated cardiovascular risk throughout her life. As a physician you will need to make the diagnosis, manage the immediate complaint (irregular cycles, unwanted hair, acne, infertility), and coordinate long-term surveillance — all skills this module develops.
RECALL
Before entering the pathophysiology, recall the hypothalamic-pituitary-ovarian (HPO) axis from your Physiology studies. The hypothalamus secretes GnRH in pulses; the anterior pituitary responds with LH and FSH. FSH stimulates follicular development and granulosa-cell oestrogen synthesis; LH triggers the midcycle surge and ovulation, and in the luteal phase supports progesterone production. Insulin signalling — from your Biochemistry training — promotes glucose uptake and also acts on ovarian theca cells to stimulate androgen synthesis. Normal androgen levels in women derive from the ovary (testosterone, androstenedione) and the adrenal gland (DHEAS). A disruption in any of these axes can manifest as the PCOS phenotype.
Clinical Presentation of PCOS
PCOS presents along three overlapping clinical domains: menstrual dysfunction, androgen excess, and metabolic disturbance. A thorough history and clinical examination mapping all three domains is essential because no single feature is diagnostic on its own.
The most common presenting symptom is oligomenorrhoea — menstrual cycles occurring fewer than eight times per year or with a cycle length greater than 35 days. A minority of women present with amenorrhoea (complete absence of periods for ≥3 months). Paradoxically, some women with PCOS menstruate regularly but still have anovulatory cycles, which may only become apparent when fertility is desired.
Clinical androgen excess manifests as hirsutism (coarse, pigmented hair in a male distribution — upper lip, chin, chest, linea alba, inner thighs), acne (particularly along the jawline and lower face), and — in severe cases — virilisation (clitoromegaly, voice deepening, temporal hair thinning). It is important to distinguish cosmetically distressing hirsutism from true virilisation: virilisation suggests a more sinister androgen source such as an androgen-secreting tumour.
Metabolic features include weight gain or frank obesity (present in 50-80% of affected women in some series), acanthosis nigricans (velvety hyperpigmented skin folds at the nape, axillae, and groin — a cutaneous marker of insulin resistance), and skin tags. Not all women with PCOS are obese; the lean PCOS phenotype is well recognised, particularly in South Asian women where insulin resistance may be present even at a normal BMI.
On examination, document: BMI, waist circumference, blood pressure, acanthosis nigricans, hirsutism (using the modified Ferriman-Gallwey score — see the Hyperandrogenism SDL), acne distribution, and signs of thyroid disease or Cushing syndrome.
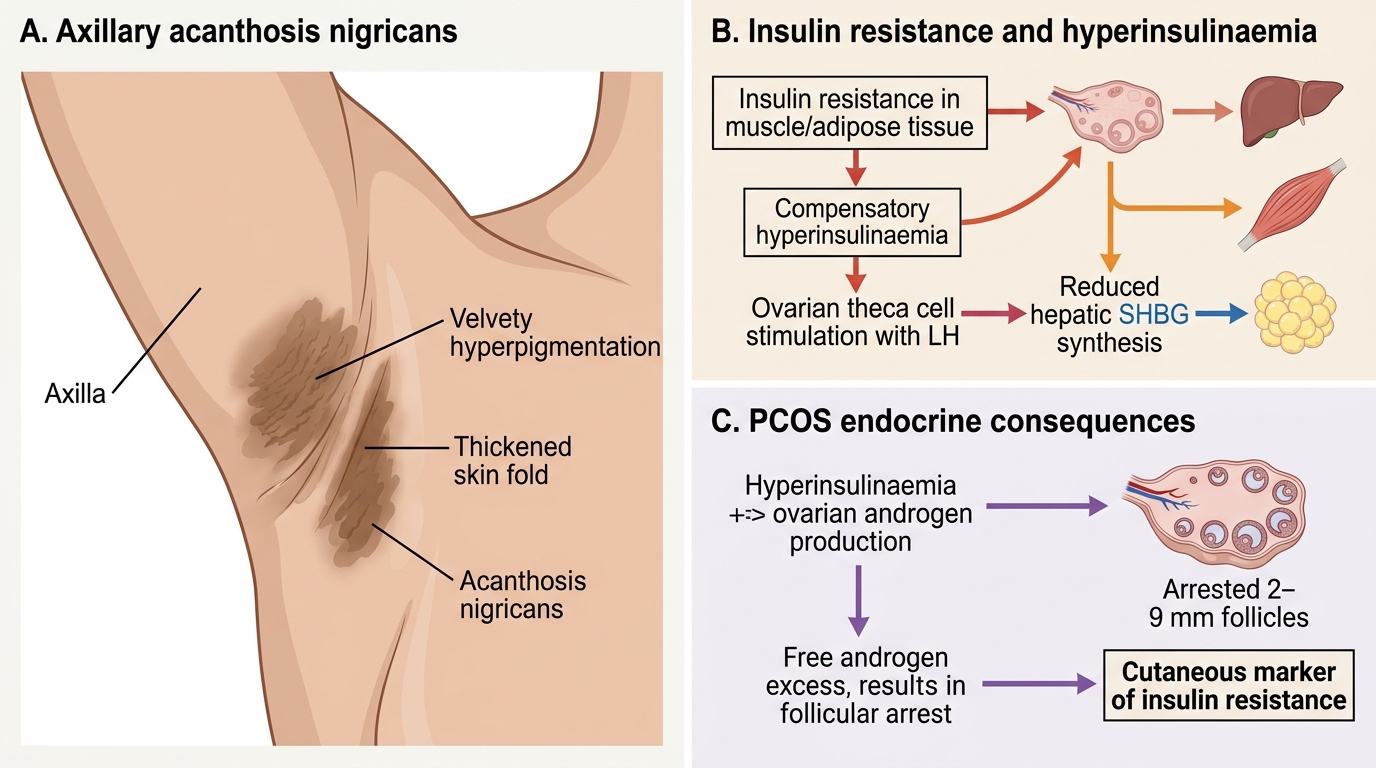
Acanthosis Nigricans as a Marker of Insulin Resistance in PCOS
Pathophysiology: Insulin Resistance and Androgen Excess
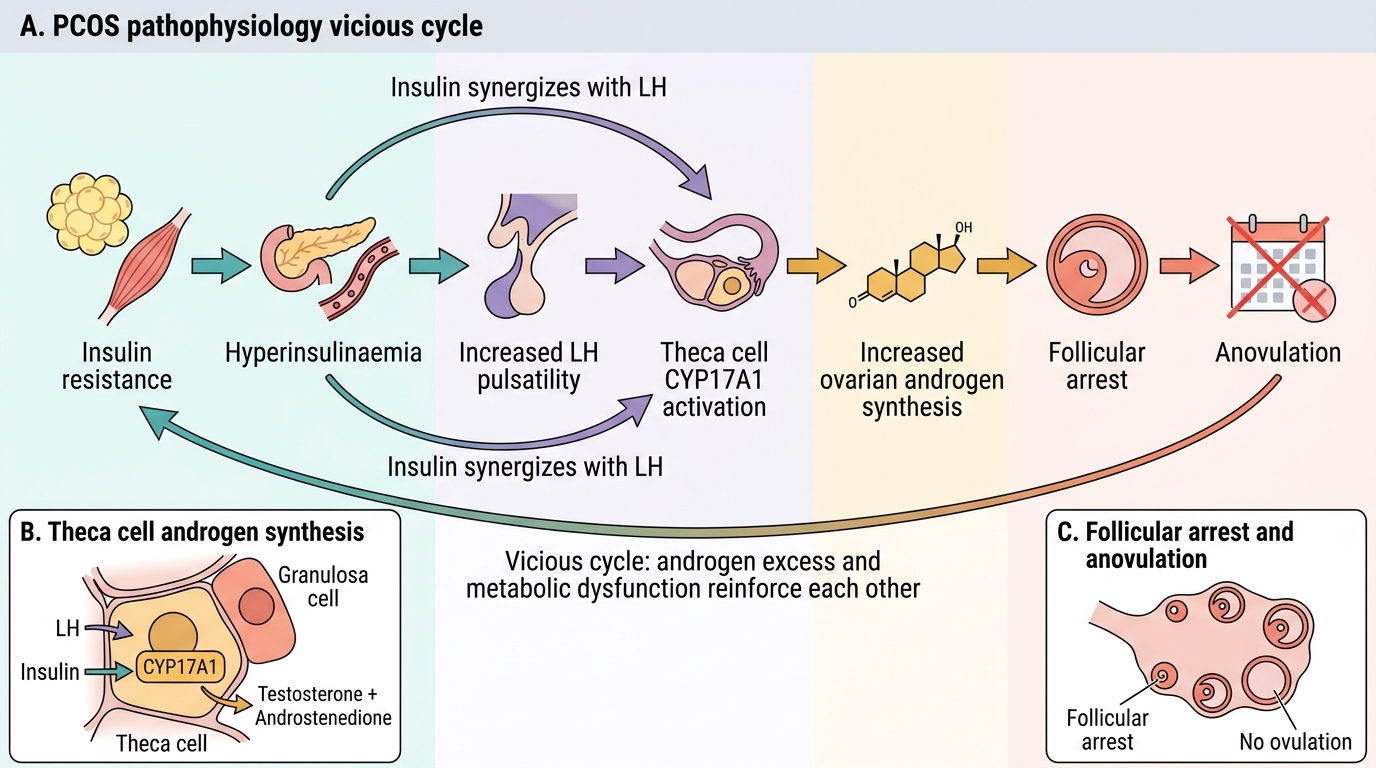
The central pathophysiological mechanism in PCOS is a vicious cycle linking insulin resistance, hyperinsulinaemia, and excess androgen production. Understanding this cycle explains both the clinical phenotype and the rationale for management choices.
In approximately 70% of women with PCOS, cells exhibit impaired insulin receptor signalling — particularly in skeletal muscle and adipose tissue. The pancreas compensates by secreting more insulin, producing hyperinsulinaemia. Ovarian theca cells, however, remain sensitive to insulin; elevated insulin acts synergistically with LH to up-regulate the cytochrome P450c17 enzyme (CYP17A1), dramatically increasing ovarian androgen synthesis (testosterone and androstenedione). Simultaneously, insulin suppresses hepatic synthesis of sex hormone-binding globulin (SHBG), which further amplifies free androgen levels in the circulation.
Excess androgens in the ovarian follicle impair normal follicular development and maturation. Small antral follicles (2-9 mm) are recruited but do not progress to dominance; they arrest and accumulate — producing the characteristic polycystic ovarian morphology on ultrasound. The follicular arrest is accompanied by disrupted LH pulsatility: LH pulse frequency and amplitude are elevated, shifting the LH:FSH ratio upward (often >2:1, though this is supportive rather than diagnostic). Elevated LH further stimulates theca-cell androgen production, closing the cycle.
Androgens are peripherally converted to oestrone (E1) in adipose tissue via aromatisation. This chronic, unopposed, non-cyclic oestrogen exposure — without the counterbalancing progesterone of normal luteal phases — is responsible for the long-term endometrial hyperplasia risk in PCOS.
Adrenal androgen excess (elevated DHEAS) coexists in about 25% of PCOS cases, reflecting adrenal CYP17A1 dysregulation.
PCOS Pathophysiology: Insulin-Androgen Vicious Cycle
SELF-CHECK
Which enzyme, up-regulated by hyperinsulinaemia in theca cells, drives excess ovarian androgen synthesis in PCOS?
A. Aromatase (CYP19A1)
B. CYP17A1 (17α-hydroxylase/17,20-lyase)
C. 3β-hydroxysteroid dehydrogenase
D. Steroidogenic acute regulatory (StAR) protein
Reveal Answer
Answer: B. CYP17A1 (17α-hydroxylase/17,20-lyase)
CYP17A1 is the rate-limiting enzyme for androgen synthesis in both the ovary and adrenal gland. Insulin and LH act synergistically to up-regulate CYP17A1 in theca cells, driving excess testosterone and androstenedione production. Aromatase (CYP19A1) converts androgens to oestrogens in granulosa cells and adipose tissue — useful context, but it is not the driver of androgen excess in PCOS.
Rotterdam 2003 Criteria and Diagnosis of Exclusion
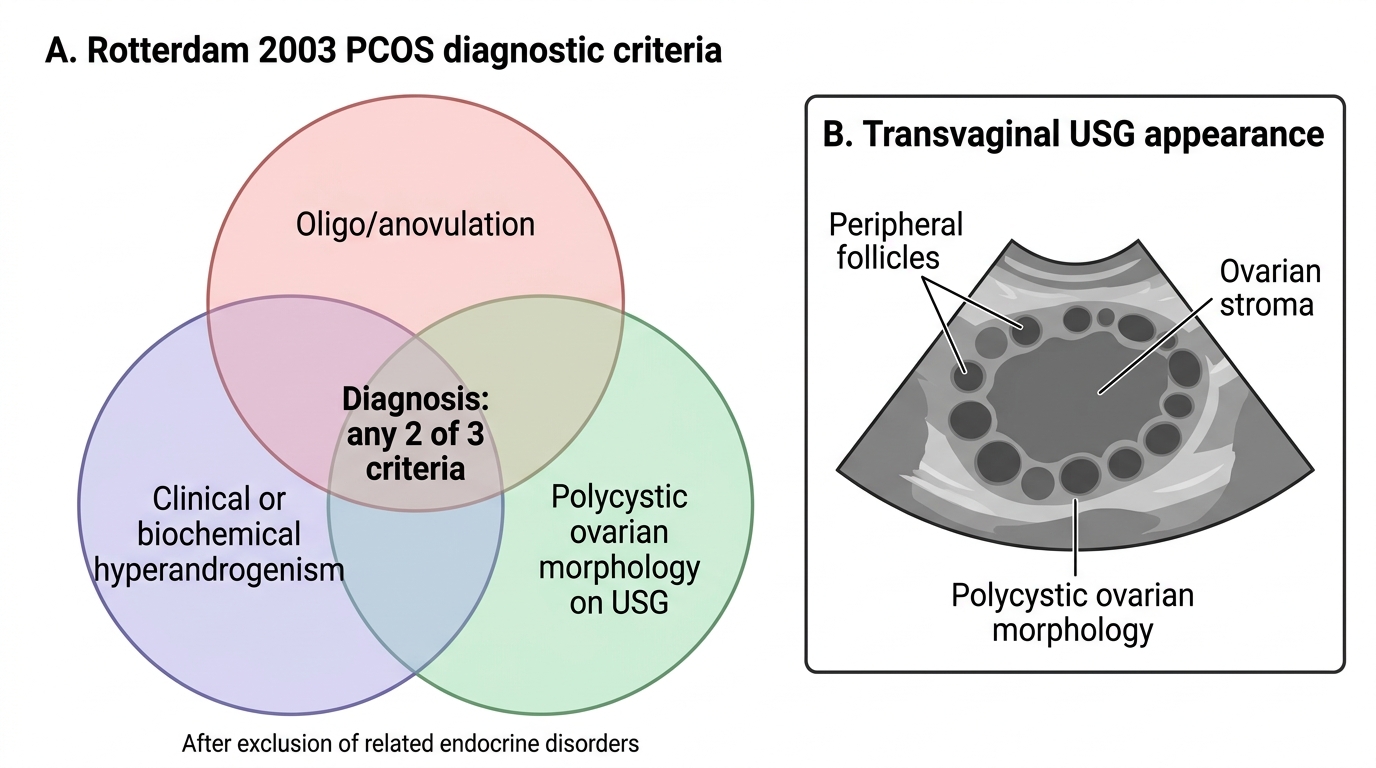
PCOS is defined by the Rotterdam 2003 consensus criteria, an international diagnostic framework agreed at a joint ESHRE/ASRM consensus workshop and subsequently validated in large populations worldwide. The Rotterdam criteria have been in use for over two decades and remain the accepted standard for clinical diagnosis, though their application requires both a positive diagnosis (two of three features present) and a negative one (exclusion of conditions that mimic the same triad). This dual requirement — positive and negative — makes PCOS categorically different from most diagnoses you have studied, which depend on a single positive finding. Getting this logic right in practice is what separates thorough from superficial gynaecological assessment. The criteria require the presence of at least 2 of the following 3 features — and crucially, the exclusion of other disorders that can produce the same triad:
- Oligo-ovulation or anovulation — cycle frequency <8/year or cycle length >35 days, or evidence of anovulation on progesterone assay
- Clinical and/or biochemical signs of hyperandrogenism — hirsutism (modified Ferriman-Gallwey score ≥8), acne, or elevated serum total/free testosterone or androstenedione
- Polycystic ovarian morphology (PCOM) on ultrasound — ≥20 follicles per ovary (2-9 mm each) OR ovarian volume ≥10 mL on transvaginal ultrasound (using the updated 2018 threshold; the older criterion of ≥12 follicles was superseded when high-resolution transducers became standard)
Importantly, PCOM on ultrasound alone, without the other features, does not constitute PCOS — ovarian morphology is common in healthy young women. Conversely, a woman with oligomenorrhoea and hyperandrogenism satisfies Rotterdam even with a normal-appearing ovary on USG.
PCOS is a diagnosis of exclusion. Before confirming the diagnosis, the following conditions must be ruled out because they can independently produce some or all of Rotterdam's three features:
- Thyroid dysfunction (hypothyroidism → menstrual irregularity)
- Hyperprolactinaemia (elevated prolactin → oligomenorrhoea, galactorrhoea)
- Late-onset (non-classic) congenital adrenal hyperplasia (21-hydroxylase deficiency → elevated 17-hydroxyprogesterone, hyperandrogenism)
- Cushing syndrome (cortisol excess → weight gain, menstrual disturbance, androgen excess)
- Androgen-secreting tumour (ovarian or adrenal — rapid-onset virilisation with very high testosterone)
A working mnemonic: PCOS MATCH — P-COS comes after excluding Menstrual/thyroid, Adrenal (CAH, Cushing), Tumour, and Hyperprolactinaemia.
Rotterdam 2003 Criteria for PCOS