Page 14 of 24
OG30.1 | PCOS — SDL Guide (Part 2)
Investigations: What to Order and Why
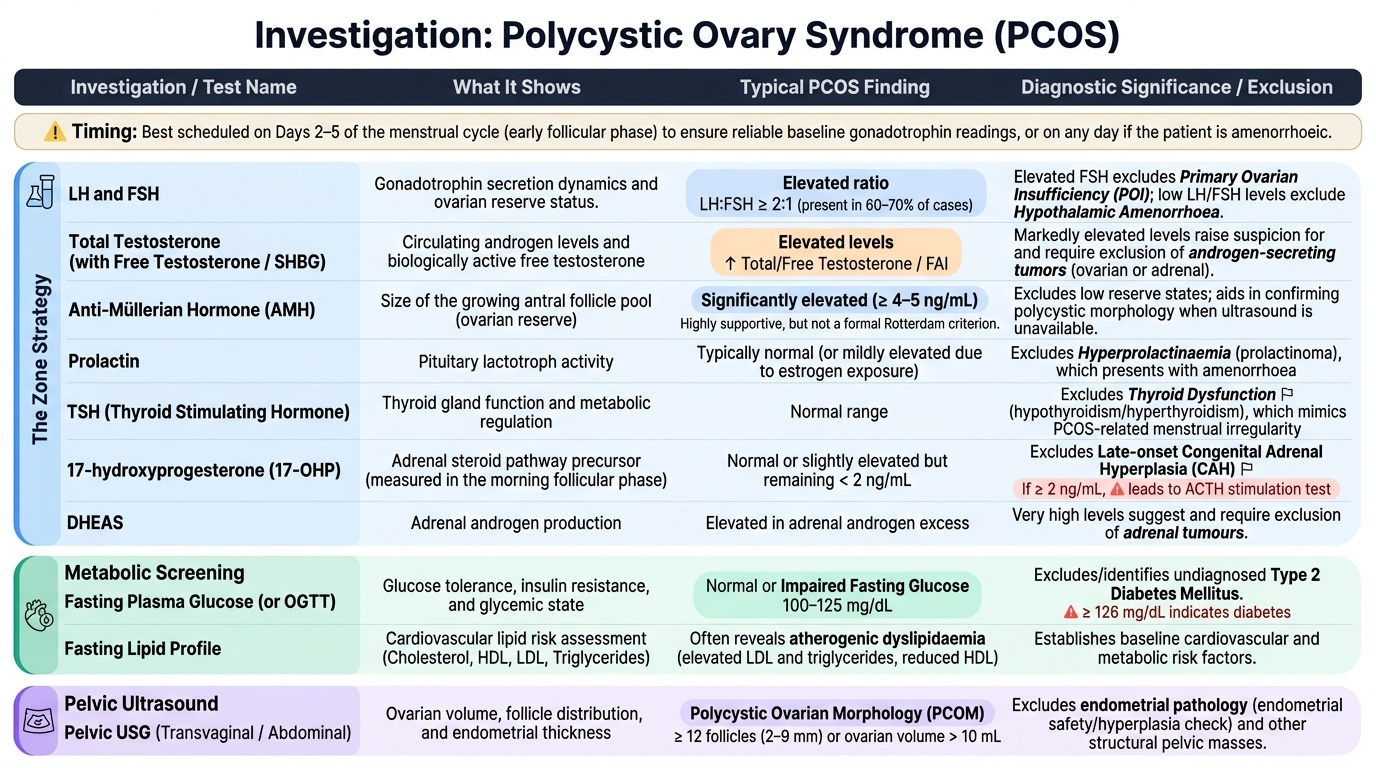
The investigation strategy in PCOS serves two equally important purposes: confirming the Rotterdam features objectively and systematically excluding the conditions that mimic PCOS. Ordering investigations without a clinical rationale wastes resources and can generate misleading results — for example, an LH:FSH ratio >2:1 is supportive of PCOS but is neither sensitive nor specific enough to drive management, whereas a markedly elevated 17-OHP may change the diagnosis entirely to late-onset CAH. The investigation set is therefore divided into three functional groups: a hormonal panel that addresses each Rotterdam criterion and each diagnostic mimic; a metabolic screen that documents cardiovascular and diabetes risk at baseline; and pelvic ultrasound that provides both morphological evidence and an endometrial safety check. Understanding WHY each test is ordered — not merely which tests to order — is what allows you to interpret results intelligently and counsel the patient about what each result means for her diagnosis and her future health. Investigations should ideally be timed on days 2-5 of the menstrual cycle for hormone testing (when FSH/LH readings are most reliable in the early follicular phase), or on any day if the woman is amenorrhoeic.
Hormonal panel (timed on day 2-5 of menstrual cycle, or any day if amenorrhoeic):
- LH and FSH — an LH:FSH ratio >2:1 is found in 60-70% of PCOS; primarily used to exclude primary ovarian insufficiency (elevated FSH) or hypothalamic amenorrhoea (low LH and FSH)
- Total testosterone (and free testosterone or SHBG to derive free androgen index) — elevated in biochemical hyperandrogenism
- Prolactin — to exclude hyperprolactinaemia
- TSH — to exclude thyroid disease
- 17-hydroxyprogesterone (17-OHP) — a morning basal level >2 ng/mL (follicular phase) warrants an ACTH stimulation test to confirm or exclude late-onset CAH
- DHEAS — elevated in adrenal androgen excess; very high levels suggest adrenal tumour
- AMH (anti-Müllerian hormone) — characteristically elevated in PCOS (often >4-5 ng/mL), correlates with follicle pool; supports diagnosis but is NOT a formal Rotterdam criterion
Metabolic screening:
- Fasting plasma glucose — to screen for impaired fasting glucose (100-125 mg/dL) or diabetes (≥126 mg/dL); OGTT if risk factors present
- Fasting lipid profile — to screen for dyslipidaemia (metabolic syndrome)
- Blood pressure and waist circumference — metabolic syndrome assessment
Pelvic ultrasound (TVS preferred for accuracy):
- Follicle count per ovary (≥20 follicles 2-9 mm = PCOM criterion)
- Ovarian volume (≥10 mL = PCOM criterion)
- Endometrial thickness (chronic anovulation → endometrial hyperplasia risk)
Provided image
Differential Diagnosis
The differential diagnosis of PCOS is broad because its three defining features — menstrual irregularity, androgen excess, and polycystic-appearing ovaries — can each arise from distinct pathologies. A systematic approach to the differential prevents the common error of diagnosing PCOS by default without exclusion.
The most important mimics to exclude are:
Hyperprolactinaemia produces amenorrhoea or oligomenorrhoea through suppression of GnRH pulsatility. It may coexist with polycystic-appearing ovaries on USG. Key distinguishing feature: elevated serum prolactin, galactorrhoea on breast examination; MRI pituitary if prolactin is substantially elevated.
Hypothyroidism causes menstrual irregularity (both oligomenorrhoea and menorrhagia), weight gain, and can mimic PCOS metabolically. TSH is the screening test; when elevated, T4 confirms overt or subclinical disease.
Late-onset (non-classic) congenital adrenal hyperplasia (CAH) due to 21-hydroxylase deficiency is the most important single-gene mimic of PCOS. Prevalence in women with hyperandrogenism is 4-8%. Patients present with oligomenorrhoea and hirsutism indistinguishable from PCOS; ovaries may appear polycystic. Distinguish by a morning 17-OHP >2 ng/mL (follicular phase), confirmed with ACTH stimulation test (peak 17-OHP >10 ng/mL).
Cushing syndrome (cortisol excess) produces central obesity, moon facies, striae, hypertension, and menstrual irregularity with androgen excess. Screen with 24-hour urinary free cortisol or overnight low-dose dexamethasone suppression test.
Androgen-secreting tumour (ovarian arrhenoblastoma/Sertoli-Leydig cell tumour; adrenal carcinoma) must be considered when virilisation is rapid-onset, progressing over months rather than years, and when serum total testosterone is markedly elevated (>200 ng/dL). Pelvic/adrenal imaging is mandatory in this setting.
| Condition | Key distinguishing feature | Confirmatory test |
|---|---|---|
| PCOS | 2-of-3 Rotterdam criteria; exclusion of others | Pelvic USG + hormone panel |
| Hyperprolactinaemia | Galactorrhoea; amenorrhoea | Serum prolactin; MRI pituitary |
| Hypothyroidism | Fatigue, cold intolerance, menorrhagia | Serum TSH |
| Late-onset CAH | Morning 17-OHP >2 ng/mL | ACTH stimulation test |
| Cushing syndrome | Central obesity, striae, hypertension | 24-h UFC or LDDST |
| Androgen-secreting tumour | Rapid virilisation, testosterone >200 ng/dL | Pelvic/adrenal imaging |
SELF-CHECK
A 26-year-old woman presents with oligomenorrhoea and hirsutism. Her LH and FSH are normal, testosterone is mildly elevated, ultrasound shows 22 follicles per ovary. Her morning 17-OHP is 3.5 ng/mL (follicular phase). What is the most appropriate next step?
A. Diagnose PCOS and start lifestyle counselling
B. Order a serum prolactin level
C. Perform an ACTH stimulation test
D. Start the combined oral contraceptive pill
Reveal Answer
Answer: C. Perform an ACTH stimulation test
A morning basal 17-OHP >2 ng/mL in the follicular phase raises the suspicion of late-onset (non-classic) CAH due to 21-hydroxylase deficiency. An ACTH stimulation test (Synacthen test) is required to confirm: a peak 17-OHP >10 ng/mL confirms the diagnosis. PCOS cannot be diagnosed until this mimic is excluded — this is the 'diagnosis of exclusion' rule. Starting COC or lifestyle counselling before confirming the diagnosis would be premature.
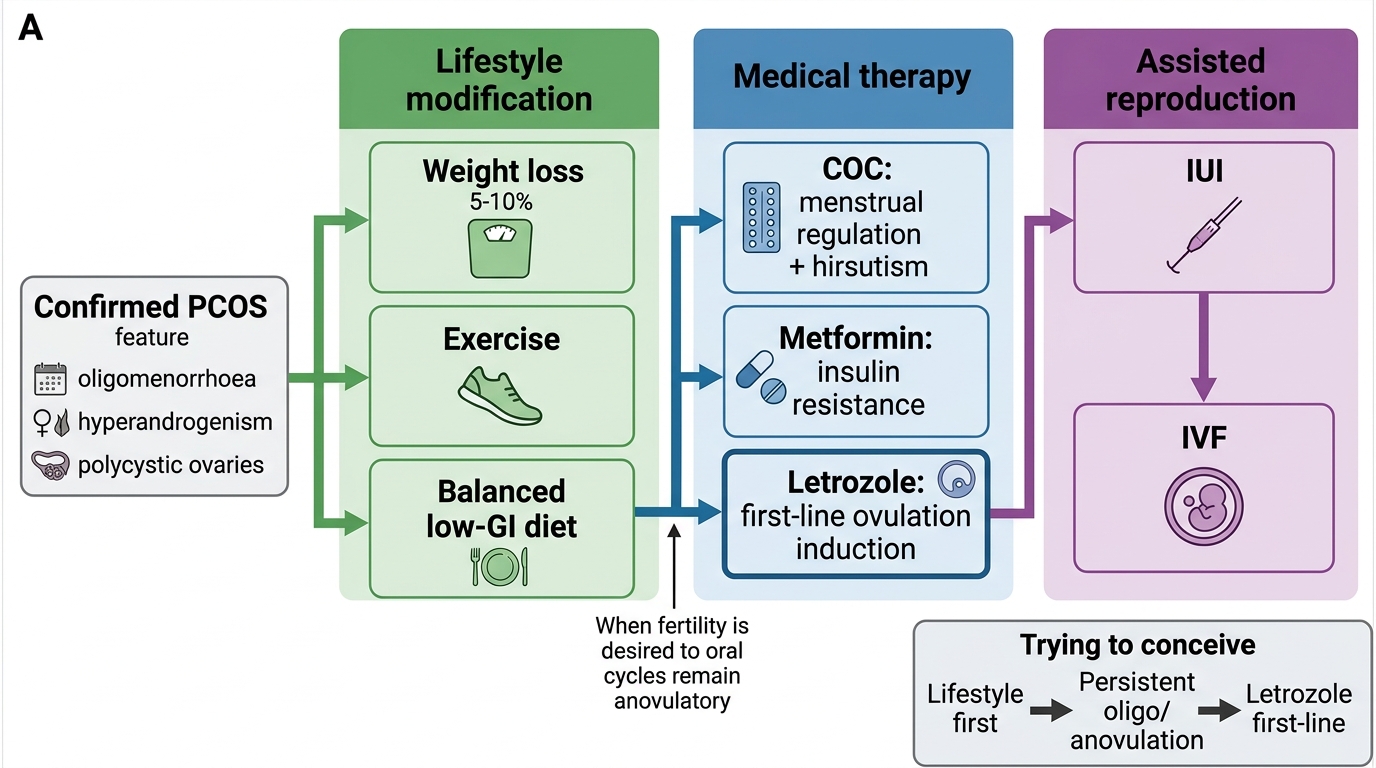
Management: Lifestyle, Medical and Assisted Reproduction
Management of PCOS is individualised according to the woman's primary concern — menstrual regulation, androgen excess, or fertility — while simultaneously addressing the underlying metabolic risk. Treatment is tiered: lifestyle modification is always first-line because it addresses the root pathophysiology; medications are added based on specific goals.
1. Lifestyle modification (first-line for all women with PCOS)
Even a modest 5-10% reduction in body weight in overweight or obese women with PCOS significantly restores menstrual regularity, reduces androgen levels, and improves ovulation rates. The mechanism is straightforward: weight loss reduces hyperinsulinaemia, which in turn lowers ovarian androgen synthesis and raises SHBG. Exercise (at least 150 minutes of moderate-intensity activity per week) independently improves insulin sensitivity. Dietary modification should reduce total calorie intake; there is no single best dietary macronutrient composition, but low glycaemic index diets reduce post-prandial insulin spikes.
For women not desiring immediate fertility, lifestyle measures alone can restore spontaneous ovulation in 30-60% of women who achieve adequate weight loss.
2. Medical management — by presenting complaint
For menstrual regulation and androgen excess:
- Combined oral contraceptive pill (COC) is the first-line medical treatment. Oestrogen raises SHBG (reducing free androgens); progestogen provides endometrial protection and regulates withdrawal bleeds. Choose a formulation with a non-androgenic progestogen (desogestrel, norgestimate, drospirenone). Apply WHO MEC category assessment — COC is generally WHO MEC 1-2 for PCOS, but check for hypertension, migraine-with-aura, and thrombosis risk. COC does not treat underlying insulin resistance.
- Anti-androgens (spironolactone 100-200 mg/day, flutamide) may be added to COC for refractory hirsutism. Note: anti-androgens require concurrent contraception due to teratogenicity.
For insulin resistance and metabolic features:
- Metformin (500-2000 mg/day, with food) reduces hepatic glucose output, improves peripheral insulin sensitivity, and modestly lowers androgen levels and LH. It can restore ovulation in some women (particularly lean PCOS) but is less effective than letrozole as sole ovulation induction. Metformin is especially useful in women with impaired fasting glucose, overt T2DM, or intolerance to COC. Caution: GI side effects are common; start low and titrate up.
For ovulation induction (women desiring pregnancy):
- Letrozole (aromatase inhibitor, 2.5-7.5 mg/day on cycle days 3-7) is the first-line ovulation induction agent in PCOS per ESHRE 2023 guidelines. It transiently suppresses oestrogen, releasing the negative feedback on FSH and triggering mono-follicular development. Cumulative live birth rates are superior to clomiphene citrate (Legro 2014, NEJM). Letrozole is an off-label use for ovulation induction but is now the international standard of care.
- Clomiphene citrate (50-150 mg/day, days 3-7) — selective oestrogen receptor modulator; was first-line for decades but now second-choice due to inferior live birth rates compared to letrozole and concerns about anti-oestrogenic endometrial effects.
- Metformin + letrozole combination is used in clomiphene-resistant or metformin-naïve women.
- Gonadotrophins (FSH injections with ultrasound monitoring) or laparoscopic ovarian drilling are reserved for women who fail oral agents.
Management Algorithm for PCOS
SELF-CHECK
A 29-year-old woman with confirmed PCOS wishes to become pregnant. She is mildly obese (BMI 29) and has been trying to conceive for 12 months. Her cycles remain oligomenorrhoeic despite 3 months of lifestyle modification. What is the first-line pharmacological intervention for ovulation induction?
A. Clomiphene citrate 50 mg on days 3-7
B. Letrozole 2.5 mg on days 3-7
C. Metformin 1500 mg daily alone
D. FSH injections with ultrasound monitoring
Reveal Answer
Answer: B. Letrozole 2.5 mg on days 3-7
Letrozole is the first-line pharmacological agent for ovulation induction in PCOS per the ESHRE 2023 evidence-based guideline, based on Legro et al. (NEJM 2014) showing higher cumulative live birth rates than clomiphene. Clomiphene is now second-choice. Metformin alone is a weaker ovulation inducer and is generally combined with or replaced by letrozole. Gonadotrophin injections are third-line, reserved for failure of oral agents.