Page 15 of 24
OG30.1 | PCOS — SDL Guide (Part 3)
Long-Term Complications and Monitoring
PCOS is not merely a reproductive condition — it is a chronic metabolic disorder that carries significant long-term risks if left unaddressed. Final-year students and junior doctors must understand these risks so they can initiate appropriate surveillance rather than treating PCOS as a self-limited gynaecological complaint.
1. Metabolic syndrome and type 2 diabetes mellitus
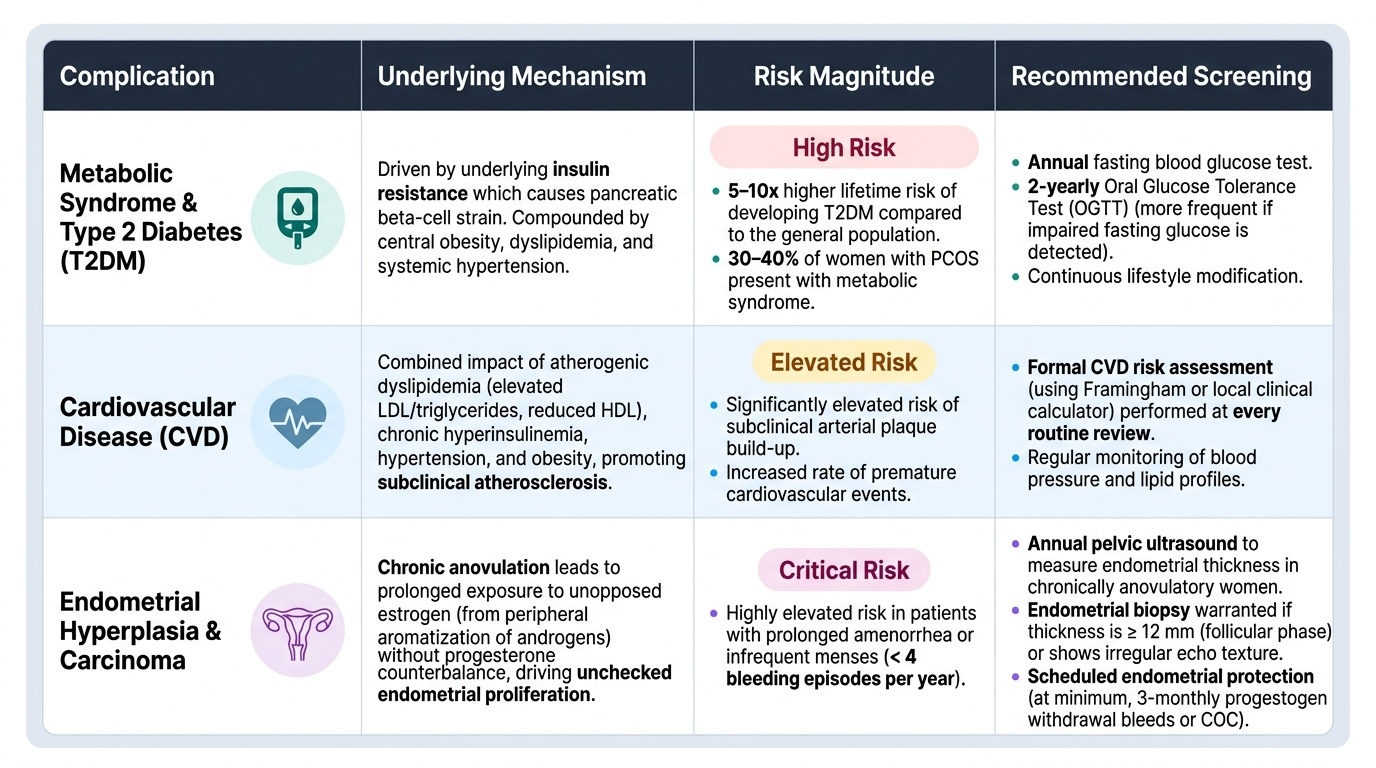
Women with PCOS have a 5-10 fold higher lifetime risk of developing type 2 diabetes compared with the general population, driven by the underlying insulin resistance. Metabolic syndrome (central obesity + dyslipidaemia + elevated blood glucose + hypertension) is present in 30-40% of women with PCOS. Annual fasting glucose and a 2-yearly OGTT (or more frequent in those with impaired fasting glucose) are recommended. Lifestyle modification significantly reduces progression risk.
2. Cardiovascular disease
Chronic hyperinsulinaemia, dyslipidaemia (elevated LDL and triglycerides, reduced HDL), hypertension, and obesity combine to elevate cardiovascular risk. Women with PCOS have higher rates of subclinical atherosclerosis. CVD risk should be formally assessed (Framingham or local calculator) at each review.
3. Endometrial hyperplasia and carcinoma
Chronic anovulation means prolonged exposure to unopposed oestrogen (from peripheral aromatisation of androgens) without the counterbalancing monthly progestogen of a normal luteal phase. This stimulates endometrial proliferation. Women with PCOS who have infrequent (<4/year) or absent menstrual shedding require scheduled endometrial protection — at minimum, 3-monthly progestogen withdrawal bleeds (medroxyprogesterone acetate 10 mg for 12-14 days per quarter) or the COC. Pelvic ultrasound measurement of endometrial thickness should be performed annually in women with chronic anovulation; endometrial thickness >12 mm in the follicular phase or irregular echo texture warrants biopsy.
4. Psychological morbidity
Anxiety, depression, and body-image disturbance are significantly more prevalent in women with PCOS — driven by hirsutism, acne, weight gain, and infertility. Screening for psychological well-being is part of holistic PCOS care.
5. Sleep-disordered breathing
Obstructive sleep apnoea is 5-10 times more prevalent in women with PCOS than age- and weight-matched controls, partly due to the independent androgen effect on upper-airway muscle tone. Ask about snoring and daytime somnolence.
Provided image
CLINICAL PEARL
The three most common errors in PCOS management that you should avoid:
1. Diagnosing PCOS without exclusion: always check TSH, prolactin, and 17-OHP before finalising the diagnosis — late-onset CAH is found in up to 8% of women presenting with the PCOS phenotype.
2. Neglecting endometrial protection: a woman who menstruates fewer than four times per year due to anovulation has chronic unopposed oestrogen exposure. Endometrial hyperplasia is silent until it causes irregular bleeding. Initiate scheduled progestogen or COC routinely.
3. Confusing letrozole and clomiphene as equivalent: letrozole is now first-line for ovulation induction (ESHRE 2023, supported by NEJM 2014 RCT showing higher live birth rates). Prescribing clomiphene first is now a deviation from standard of care in most settings.
SELF-CHECK
A 32-year-old woman with known PCOS has had only 2 menstrual periods in the past year and is not planning pregnancy. Her endometrial thickness on pelvic USG is 14 mm. What is the most appropriate immediate management?
A. Reassure and repeat ultrasound in 6 months
B. Start COC immediately to provide hormonal regulation
C. Perform endometrial biopsy to exclude hyperplasia or malignancy
D. Start letrozole to induce ovulation and shed the endometrium
Reveal Answer
Answer: C. Perform endometrial biopsy to exclude hyperplasia or malignancy
Endometrial thickness >12 mm in the follicular phase in a woman with chronic anovulation (only 2 periods/year) warrants endometrial biopsy before any hormonal intervention, to exclude endometrial hyperplasia or well-differentiated endometrial carcinoma. Reassurance alone is inappropriate given the thickness. COC can be started after histological confirmation of benign endometrium. Letrozole is for ovulation induction in women seeking pregnancy, not for managing endometrial thickening.
Self-Assessment: PCOS
Use the following questions to consolidate your learning. Attempt each question before revealing the answer.
Q1. A 20-year-old woman has oligomenorrhoea (6 periods/year) and acne. Ultrasound shows 15 follicles per ovary (each 4-7 mm). Testosterone and other hormones are normal. Does she meet Rotterdam criteria for PCOS?
Answer: She has 2 of 3 features — oligo-ovulation and clinical hyperandrogenism (acne). PCOM is not met (15 follicles < 20 threshold). Two of three criteria are still fulfilled, so Rotterdam criteria ARE met, provided other causes of oligomenorrhoea and acne are excluded. Note: PCOM requires ≥20 follicles per ovary (2018 threshold); 15 follicles does not meet PCOM, but the other 2 criteria suffice.
Q2. Why is a COC pill that contains a first-generation progestogen (e.g. norethisterone) less desirable in PCOS?
Answer: First-generation progestogens are androgenic — they can exacerbate hirsutism and acne, which are core complaints in PCOS. Preferred formulations use non-androgenic or anti-androgenic progestogens (drospirenone, desogestrel, norgestimate).
Q3. A woman with PCOS achieves spontaneous conception after 3 months of lifestyle modification alone. What ongoing monitoring does she still require?
Answer: She requires ongoing monitoring for gestational diabetes (PCOS confers higher GDM risk — OGTT at 24-28 weeks), as well as long-term metabolic surveillance post-pregnancy: annual fasting glucose, lipid profile, BP, and BMI.
Q4. What is the mechanism by which a 10% reduction in body weight improves menstrual regularity in obese PCOS?
Answer: Weight loss reduces adipose tissue mass and caloric intake, lowering fasting insulin levels. Reduced hyperinsulinaemia → less stimulation of ovarian CYP17A1 → lower androgen synthesis → rising SHBG → lower free androgen levels → partial restoration of normal HPO axis pulsatility → spontaneous follicular maturation and ovulation.