Page 17 of 24
OG34.6 | Endometriosis-Adenomyosis Spectrum — SDL Guide (Part 2)
Investigation and Diagnosis
The investigation of suspected endometriosis or adenomyosis requires a tiered approach that begins with clinical assessment and non-invasive imaging and escalates to surgical diagnosis when required.
Laparoscopy — gold standard for endometriosis. Direct laparoscopic visualisation and biopsy of suspicious peritoneal lesions, followed by histological confirmation of endometrial glands and stroma, remains the definitive diagnostic standard. Laparoscopy allows simultaneous assessment of disease extent, staging, and therapeutic intervention (ablation or excision at the same sitting). It should be performed in women with clinical suspicion of endometriosis where non-invasive investigations are inconclusive or where surgical treatment is planned.
Transvaginal ultrasound (TVS-USG) is the first-line imaging modality for both conditions. For endometriosis, TVS is highly accurate for detecting endometriomas — a classic endometrioma appears as a unilocular cyst with homogeneous low-level internal echoes ('ground-glass' pattern) and no papillary projections; sensitivity >90%, specificity >90% for endometrioma. TVS is, however, less sensitive for detecting peritoneal implants, uterosacral lesions, or deep infiltrating endometriosis. For adenomyosis, TVS findings include: a globally enlarged, globular uterus; myometrial cysts (small anechoic spaces within the myometrium); echogenic myometrial foci (haemosiderin deposits); asymmetrical myometrial thickening; and fan-shaped shadowing ('striped myometrium'). TVS sensitivity for adenomyosis is approximately 70–80%, improving with 3D ultrasound.
MRI pelvis is the preferred modality for complex cases: deep infiltrating endometriosis (DIE), bowel endometriosis, pre-operative surgical mapping, and when TVS is inconclusive for adenomyosis. For adenomyosis, MRI is the most accurate non-invasive investigation: it demonstrates a thickened junctional zone (>12 mm — the most specific sign), high-signal T1 foci within the myometrium, and ill-defined low-signal myometrial bands. MRI junctional zone thickness >12 mm has a sensitivity of ~85% and specificity of ~90% for adenomyosis.
CA-125 (cancer antigen 125) is elevated in endometriosis (typically modestly, often 35–200 IU/mL), but it is neither sensitive nor specific enough for diagnosis. It is most useful as a monitoring tool — rising CA-125 after medical or surgical treatment may indicate recurrence. CA-125 is also elevated in ovarian cancer, fibroids, PID, and even physiological states, so an elevated value always requires contextual interpretation.
Definitive diagnosis of adenomyosis is histological — made on hysterectomy specimens showing endometrial glands and stroma within the myometrium at >2.5 mm from the basal endometrium. In current practice, pre-operative MRI effectively guides the clinical diagnosis and management decision without requiring histology first, unless malignancy is a concern.
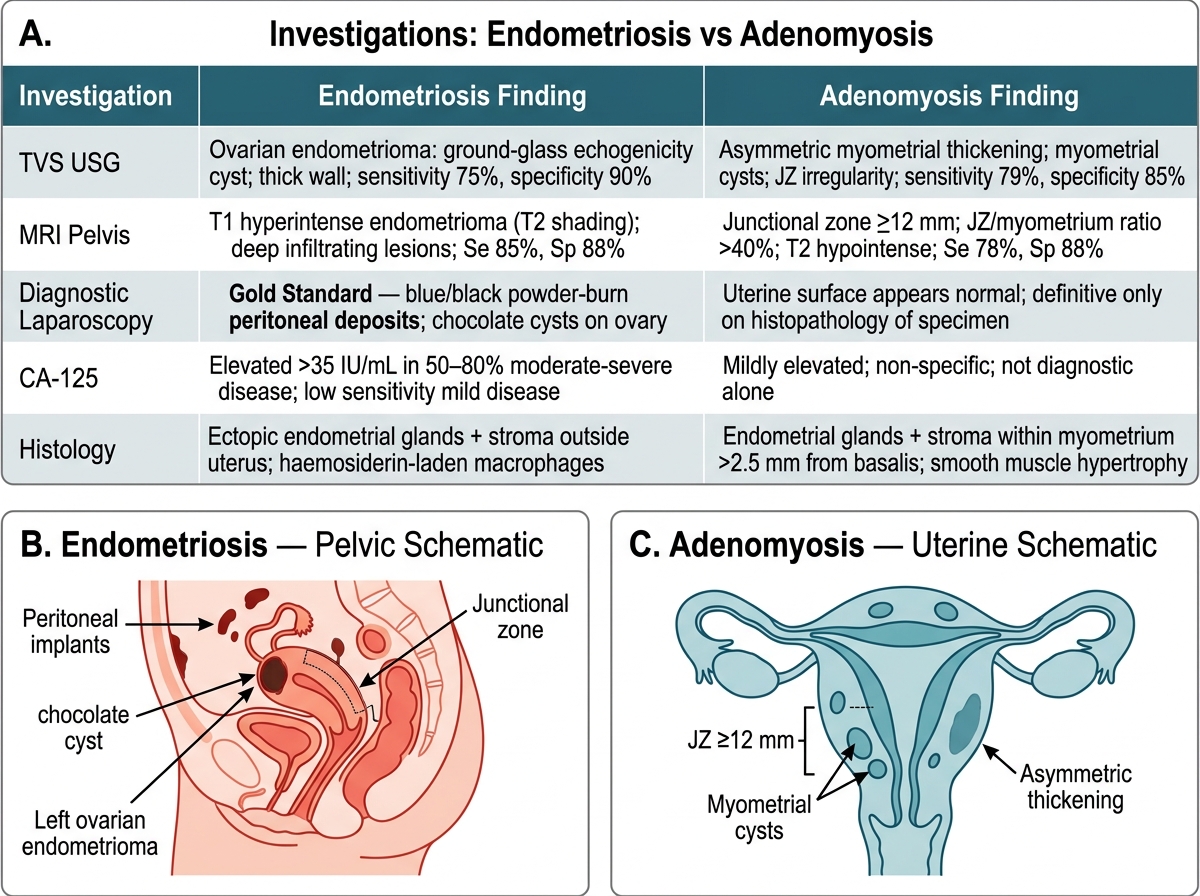
Comparison of Investigations: Endometriosis vs Adenomyosis
SELF-CHECK
A 38-year-old woman with menorrhagia has a globally enlarged, boggy, tender uterus (equivalent to 12-week size) with no adnexal mass. Transvaginal ultrasound shows asymmetric myometrial thickening and myometrial cysts. MRI demonstrates a junctional zone of 16 mm. Which diagnosis is most consistent and what is the most appropriate first-line medical treatment?
A. Uterine fibroids — combined oral contraceptive pill
B. Adenomyosis — levonorgestrel-releasing intrauterine system (LNG-IUS)
C. Endometriosis Stage III — GnRH analogue
D. Adenomyosis — emergency hysterectomy
Reveal Answer
Answer: B. Adenomyosis — levonorgestrel-releasing intrauterine system (LNG-IUS)
The clinical picture (globally enlarged boggy tender uterus, no adnexal mass), ultrasound findings (myometrial cysts, asymmetric thickening), and MRI junctional zone >12 mm all strongly point to adenomyosis. The first-line medical treatment is the LNG-IUS (levonorgestrel-releasing intrauterine system/Mirena), which delivers local progestin to suppress endometrial and ectopic gland activity, reducing menorrhagia and dysmenorrhoea significantly. It is preferred over hysterectomy (a definitive but major surgical step) as the initial approach. GnRH analogues are second-line or pre-operative adjuncts.
Management of Endometriosis
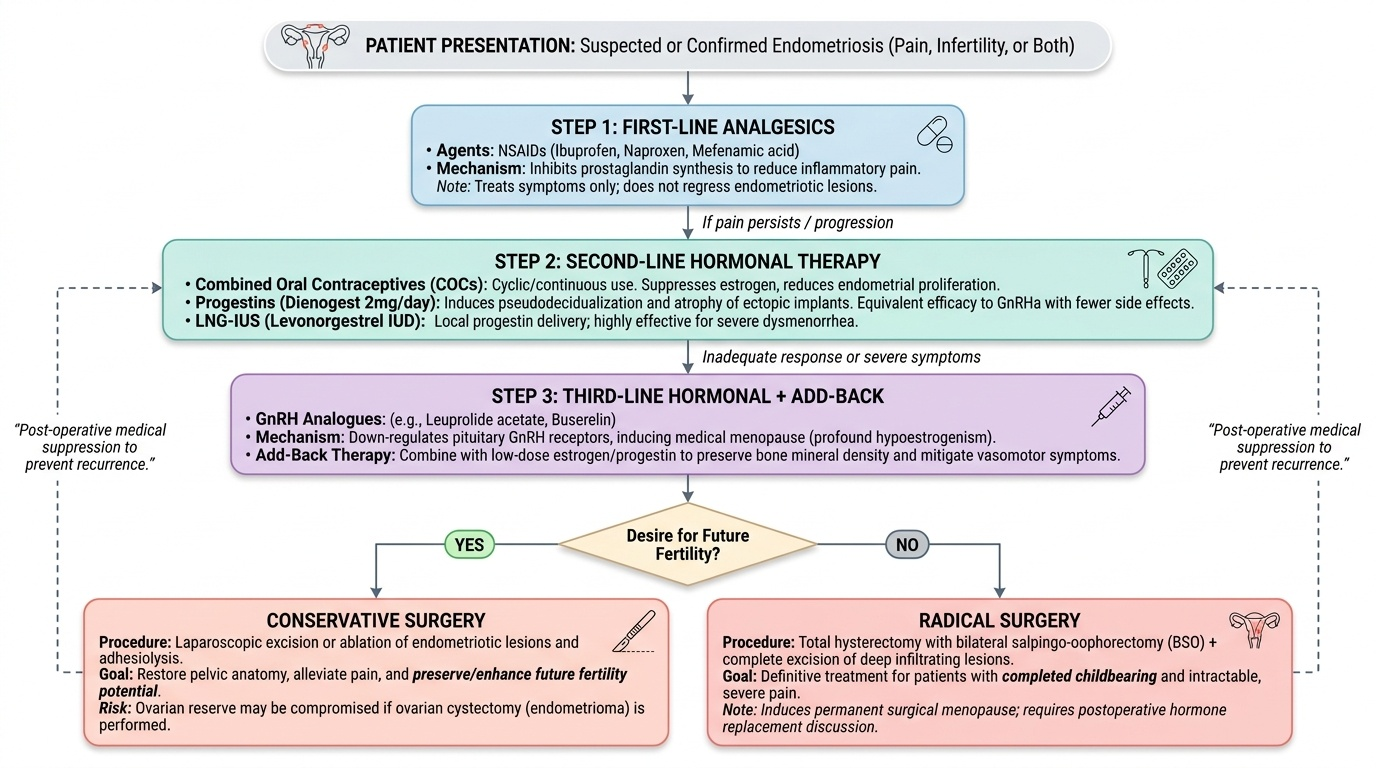
Management of endometriosis is tailored to the woman's primary complaint (pain, infertility, or both), her desire for future fertility, disease stage, and symptom severity. There is no curative medical therapy for endometriosis — all hormonal treatments suppress disease activity while in use and allow progression after cessation. Surgical treatment can debulk disease but is associated with recurrence, particularly if ovarian reserve is compromised.
Medical management. The objectives of medical therapy are pain relief and suppression of disease progression through hormonal manipulation, exploiting the oestrogen dependence of endometriotic implants.
First-line analgesics and anti-inflammatory agents: NSAIDs (ibuprofen, mefenamic acid, naproxen) are the initial analgesic choice. They inhibit prostaglandin synthesis and reduce the inflammatory pain and dysmenorrhoea associated with endometriosis. They do not treat the underlying lesions.
Hormonal suppression — first line: Combined oral contraceptive pill (COC), used cyclically (standard 21-day cycles to reduce monthly flares) or continuously (to eliminate menstruation altogether), reduces endometrial proliferation via progesterone-dominant effect and oestrogen suppression. COC is the most widely used first-line hormonal therapy, particularly in adolescents and young women who do not wish to conceive. It is contraindicated in women with migraine with aura, active thromboembolic disease, and other WHO MEC category 3/4 conditions. Progestins alone (norethisterone, medroxyprogesterone acetate, dienogest) induce a pseudodecidual reaction in ectopic implants and cause their atrophy. Dienogest (progestin, 2 mg/day) is a well-studied option with efficacy comparable to GnRH analogues but fewer hypoestrogenic side effects; it is increasingly preferred. The LNG-IUS provides local progestin delivery and is particularly useful when dysmenorrhoea and pelvic pain are the dominant complaints.
Second-line hormonal therapy: GnRH analogues (leuprolide acetate, buserelin, nafarelin) create a state of medical menopause by down-regulating pituitary GnRH receptors, reducing ovarian oestrogen production to near-menopausal levels. This effectively suppresses all endometriotic implants. GnRH analogues are highly effective for pain relief but cause hypoestrogenic symptoms (hot flushes, vaginal dryness, decreased libido) and bone mineral density loss. They should not be used for >6 months without add-back therapy (low-dose oestrogen-progestogen or tibolone), which attenuates hypoestrogenic side effects without reducing efficacy. Danazol (an androgen derivative) is highly effective but poorly tolerated (androgenic side effects: acne, hirsutism, voice change, weight gain) and is largely replaced by newer agents.
Surgical management. Surgery is indicated when: (a) medical therapy fails or is contraindicated; (b) an endometrioma requires excision; (c) infertility evaluation or treatment is planned; (d) DIE causing bowel/bladder symptoms needs resection.
Conservative surgery (preserving fertility): Laparoscopic ablation or excision of endometriotic implants, fulguration of peritoneal lesions, ovarian cystectomy (stripping the cyst wall of an endometrioma — preferred over drainage alone, which has high recurrence). For ovarian endometriomas >4 cm, cystectomy is the standard approach. Ablation (Stage I/II) and cystectomy are associated with improved fecundity in infertile patients with mild-moderate disease.
Radical surgery: Total abdominal or laparoscopic hysterectomy with bilateral salpingo-oophorectomy (THBSO) is the definitive treatment for women with severe, refractory endometriosis who have completed childbearing. The ovaries must be removed to eliminate the oestrogen source driving residual implants; oestrogen replacement can be given postoperatively but may stimulate residual disease. Bowel and bladder resection may be required for deeply infiltrating disease.
Fertility-desiring patients. In women with infertility and Stage I/II endometriosis, laparoscopic ablation/excision improves spontaneous pregnancy rates (modest but significant). For Stage III/IV disease, in vitro fertilisation (IVF) is generally recommended rather than attempting repeated conservative surgery, which can compromise ovarian reserve.
Provided image
Management of Adenomyosis
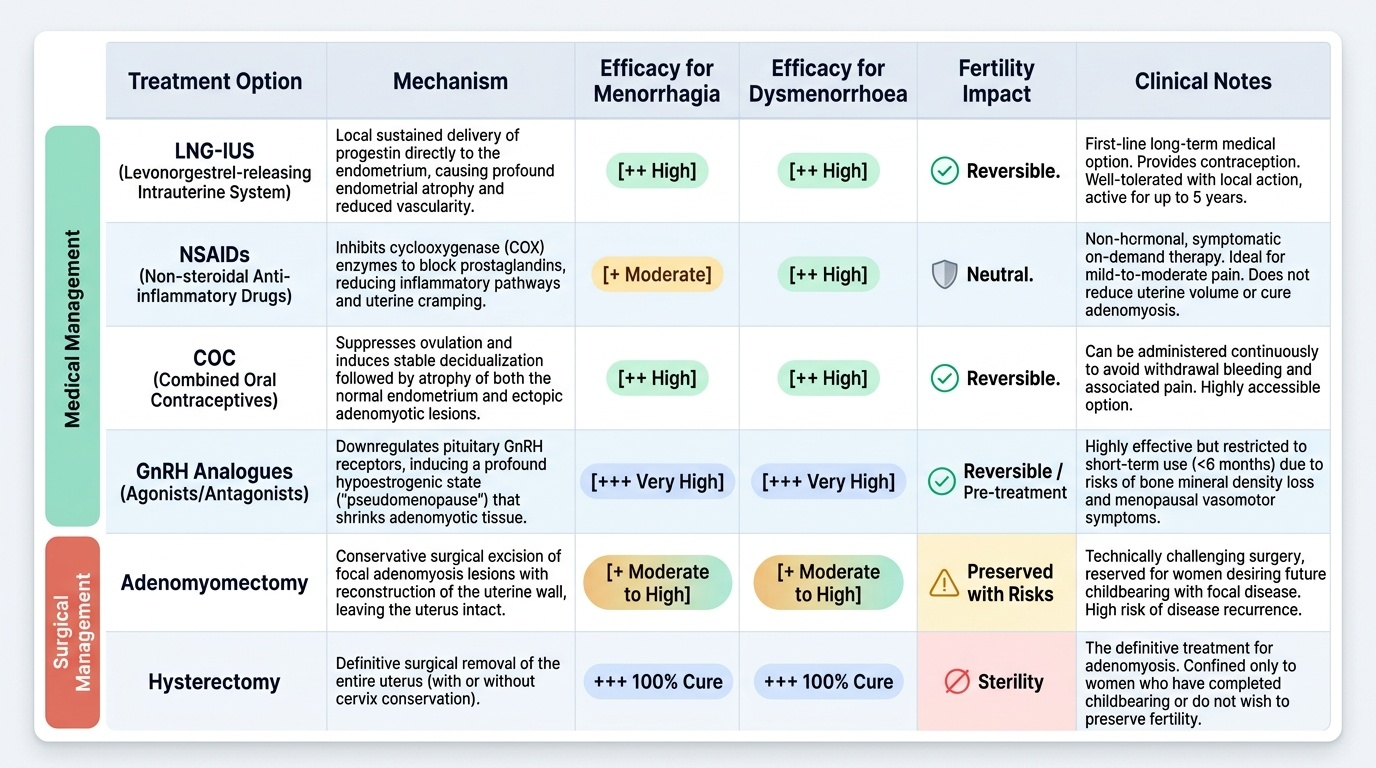
The management of adenomyosis is symptom-driven and guided by the woman's desire for future fertility, since the condition is entirely confined to the uterus and the definitive treatment — hysterectomy — removes it altogether.
Medical management. As with endometriosis, medical therapy for adenomyosis is suppressive, not curative; symptoms return when treatment is discontinued unless menopause intervenes.
The levonorgestrel-releasing intrauterine system (LNG-IUS / Mirena) is the first-line treatment for women with adenomyosis-related menorrhagia and dysmenorrhoea who wish to preserve the uterus. It releases 20 µg/day of levonorgestrel directly into the uterine cavity, causing profound endometrial atrophy and markedly reducing menstrual blood loss (up to 90% reduction in measured blood loss at 3–6 months). Local delivery avoids systemic progestogenic side effects. It is effective for up to 5 years. RCT evidence (Sheng et al., 2009, and subsequent trials) confirms significant reductions in pain scores and menorrhagia in histologically confirmed adenomyosis.
GnRH analogues are used pre-operatively to reduce uterine size and vascularity before hysterectomy (improving operative conditions), or as a medium-term bridge when the patient is not yet ready for surgery. They are not a permanent solution and are limited to 6-month courses without add-back therapy.
NSAIDs provide symptomatic relief for dysmenorrhoea. Combined oral contraceptives (cyclical or continuous) reduce menorrhagia and dysmenorrhoea in milder cases. Tranexamic acid (anti-fibrinolytic) reduces menorrhagia by 35–50% and can be combined with NSAIDs.
Surgical management. Hysterectomy is the only definitive treatment for adenomyosis and is curative. It is appropriate for women who have completed childbearing and have failed medical therapy or prefer a permanent solution. The approach may be abdominal, laparoscopic, or robotic depending on uterine size and surgeon expertise. Oophorectomy is not required since adenomyosis is not oestrogen-dependent in the same way as endometriosis — the ovaries are conserved in most premenopausal women undergoing hysterectomy for adenomyosis.
Uterus-sparing surgical options for fertility-desiring women include adenomyomectomy (excision of a focal adenomyoma) and uterine artery embolisation (UAE). The evidence for these techniques is limited compared to hysterectomy — recurrence and residual disease are common, and UAE is associated with a risk of premature ovarian failure; neither is the standard of care, and patients should be counselled about the risks and benefits.
Provided image
SELF-CHECK
A 32-year-old woman with confirmed endometriosis (Stage II) and 2 years of infertility has failed three cycles of ovulation induction. Her partner's semen analysis is normal. Laparoscopy shows minimal adhesions and patent tubes. Which of the following is the most appropriate next step regarding fertility management?
A. GnRH analogue for 6 months, then attempt natural conception
B. Laparoscopic ablation of endometriotic lesions
C. Total hysterectomy with bilateral oophorectomy
D. Combined oral contraceptive for 3 months, then IVF
Reveal Answer
Answer: B. Laparoscopic ablation of endometriotic lesions
In infertile women with Stage I/II endometriosis, laparoscopic ablation/excision of endometriotic implants improves spontaneous pregnancy rates (NNT ~8, Marcoux et al.). It addresses both the disease and provides histological confirmation. GnRH analogues suppress ovarian function and do not improve fertility; using them pre-conception delays pregnancy. Hysterectomy is not appropriate in a fertility-desiring patient. COC suppresses ovulation and delays fertility. Laparoscopic ablation is the correct first surgical step; IVF is reserved for higher-stage disease or failed conservative surgery.