Page 18 of 24
OG34.6 | Endometriosis-Adenomyosis Spectrum — SDL Guide (Part 3)
Implications for Fertility and Long-term Health
Both endometriosis and adenomyosis have important implications beyond immediate symptoms, affecting reproductive outcomes, quality of life, and long-term health over years to decades.
Endometriosis and infertility. Endometriosis is found in 30–40% of women investigated for infertility, and the relationship is multi-mechanistic. The mechanisms through which endometriosis impairs fertility include: (1) Anatomical distortion — peritubal adhesions, hydrosalpinx, and obliteration of the Pouch of Douglas impair ovum pick-up and tubal transport; (2) Ovarian damage — endometriomas reduce the functional ovarian cortex; recurrent cystectomies compound this by removing healthy ovarian tissue, reducing ovarian reserve (low AMH, poor response to stimulation); (3) Peritoneal inflammatory environment — elevated prostaglandins, activated macrophages, and cytokines in peritoneal fluid are toxic to sperm, impair fertilisation, and create a hostile implantation environment; (4) Progesterone resistance — impairs endometrial receptivity, reducing implantation rates even after successful fertilisation.
For Stage I/II endometriosis with infertility and no other factors, laparoscopic surgical treatment (ablation + adhesiolysis) modestly improves fecundity; the monthly fecundity rate (MFR) increases from ~2–5% untreated to ~5–10% post-ablation. For Stage III/IV disease with distorted anatomy, or where conservative surgery has failed or is contraindicated by poor ovarian reserve, IVF is the recommended fertility treatment — it bypasses the peritoneal environment and overcomes tubal distortion.
Adenomyosis and fertility. Adenomyosis is increasingly recognised as a cause of implantation failure and early pregnancy loss. The mechanisms include altered uterine contractility (abnormal peristalsis) and compromised endometrial receptivity in the zone adjacent to adenomyotic foci. Adenomyosis is found in a higher-than-expected proportion of women undergoing IVF with repeated implantation failure. Management of adenomyosis in fertility-desiring women is challenging; pre-IVF GnRH analogue down-regulation may improve outcomes, but the evidence is evolving.
Long-term health implications. Women with endometriosis have an elevated risk (relative risk approximately 2–3 times background) of endometrioid and clear-cell ovarian cancer, though the absolute lifetime risk remains small (~1–2% in severe endometriosis). This association is specific to the histological subtypes arising from endometriotic tissue, not all ovarian cancer types. Long-term GnRH analogue use without add-back therapy causes bone mineral density loss, with risk of osteoporosis. The chronic pain and fertility burden of endometriosis also carry significant psychological morbidity (depression, anxiety, relationship strain) that requires holistic management.
CLINICAL PEARL
The single most common reason for delayed diagnosis of endometriosis is the normalisation of dysmenorrhoea — both by patients (who believe painful periods are 'normal') and by clinicians (who reassure without investigation). The clinical red flags that demand active exclusion of endometriosis are: progressive secondary dysmenorrhoea, deep dyspareunia, dyschezia, and any young woman with infertility. A fixed retroverted uterus or tender uterosacral ligaments on pelvic examination are physical signs that should trigger urgent laparoscopic evaluation. Endometriosis is not a diagnosis of exclusion — it is a diagnosis that requires surgical confirmation, and the earlier it is made, the better the fertility outcomes. For adenomyosis, the key pearl is that the uterus in adenomyosis is soft, boggy, and tender, unlike the hard, irregular, non-tender uterus of fibroids — this distinction, missed in the examination, frequently leads to the wrong pre-operative diagnosis.
Clinical Decision Framework and Self-Assessment
Bringing together the clinical, investigative, and management threads covered in this module, the following framework summarises the clinical approach to a patient with suspected endometriosis or adenomyosis. These two conditions are among the most frequently examined gynaecological topics in final MBBS and are encountered with high frequency in clinical practice — the ability to move systematically from symptom recognition through investigation to a management plan is the core skill being tested. The key decision nodes are: recognising the dominant symptom complex, selecting the appropriate investigation pathway, and tailoring management to fertility aspirations and disease severity. Co-existence of endometriosis and adenomyosis is possible — around 10–20% of women undergoing surgery for endometriosis have coexisting adenomyosis — and the management approach must address both. The comparison table at the end of this section is a high-yield examination reference and should be committed to memory.
Step-by-step clinical approach:
- Symptom recognition: Is the dominant complaint dysmenorrhoea + dyspareunia + infertility? → Suspect endometriosis. Is it menorrhagia + bulky tender uterus in a multiparous woman in the late reproductive years? → Suspect adenomyosis. Are both present simultaneously? → Consider co-existing conditions.
- Examination: Assess uterine size, consistency, mobility, tenderness. Check posterior fornix for nodularity (endometriosis) or uniform uterine enlargement (adenomyosis).
- First-line investigation: TVS-USG — endometrioma (ground-glass cyst), adenomyosis (myometrial cysts, echogenic foci, globular uterus). MRI for complex or deep disease.
- Definitive diagnosis: Endometriosis = laparoscopy + histology. Adenomyosis = MRI (clinical diagnosis pre-operatively); histology on hysterectomy specimen.
- Management decision: Is fertility desired? → Medical suppression first (endometriosis: COC/progestins/GnRH; adenomyosis: LNG-IUS) → conservative surgery if medical fails. Childbearing complete and refractory? → Radical surgery (THBSO for endometriosis; hysterectomy for adenomyosis).
- Follow-up: Monitor symptoms + CA-125 (endometriosis) or symptom response + pelvic USG (adenomyosis post-LNG-IUS).
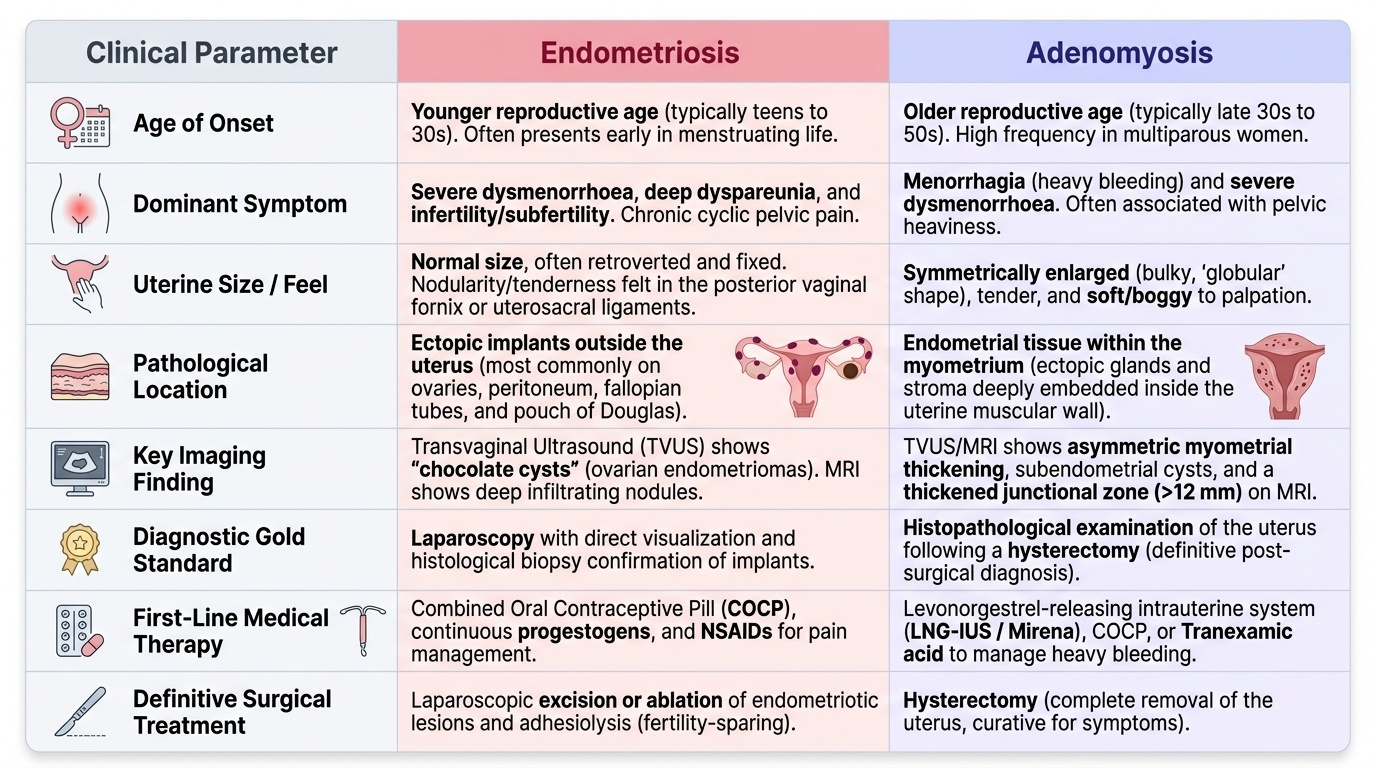
The following table provides a rapid comparison of the two conditions across key clinical parameters for examination purposes:
| Parameter | Endometriosis | Adenomyosis |
|---|---|---|
| Age group | Reproductive (20–40 yr) | Late reproductive (35–50 yr) |
| Dominant symptom | Dysmenorrhoea + dyspareunia | Menorrhagia + dysmenorrhoea |
| Infertility | Common (30–40% of infertile women) | Less prominent, emerging evidence |
| Uterus | May be fixed retroverted, normal or irregular size | Uniformly enlarged, soft, boggy, tender |
| Pathological location | Ectopic (peritoneum, ovary, POD) | Intramyometrial |
| Gold standard diagnosis | Laparoscopy + histology | MRI (junctional zone >12 mm) / histology on specimen |
| First-line medical therapy | COC or progestins (NSAIDs for pain) | LNG-IUS |
| Definitive surgical treatment | THBSO (with hysterectomy) | Hysterectomy |
Provided image
SELF-CHECK
Which of the following statements about GnRH analogues in the management of endometriosis is CORRECT?
A. They can be used indefinitely without significant adverse effects
B. They improve spontaneous pregnancy rates and should be given before attempting conception
C. They require add-back therapy if used for more than 6 months to prevent bone mineral density loss
D. They are the first-line treatment for adolescents with suspected endometriosis
Reveal Answer
Answer: C. They require add-back therapy if used for more than 6 months to prevent bone mineral density loss
GnRH analogues create a hypoestrogenic state (medical menopause), which causes bone mineral density loss. Current guidelines recommend that GnRH analogues should not be used for more than 6 months without add-back therapy (low-dose oestrogen-progestogen), which attenuates hypoestrogenic side effects without reducing therapeutic efficacy. They are not used indefinitely (option A). GnRH analogues actually suppress ovulation and do not improve pregnancy rates — they are not used pre-conceptually (option B). First-line therapy for adolescents with suspected endometriosis is COC (option D).