Page 1 of 24
OG29.1 | Fibroid Uterus — SDL Guide
Learning Objectives
- Describe the aetiology, classification (FIGO 0–8), and pathophysiology of fibroid uterus
- Enumerate the clinical features and differential diagnosis of fibroid uterus
- List the degenerations of fibroid and their clinical significance
- Outline the principles of investigation and management (medical and surgical)
INSTRUCTIONS
Fibroid uterus (leiomyoma) is the single most common pelvic tumour in women of reproductive age, encountered in up to one-third of women by age 50. Understanding its classification, degenerations, and evidence-based management is essential for final-year clinical practice. This module uses the FIGO leiomyoma subclassification system, which underpins modern treatment selection.
References
- DC Dutta's Textbook of Gynaecology, 7th edition, Ch 16 (textbook)
- Shaw's Textbook of Gynaecology, 17th edition, Ch 10 (textbook)
- FIGO Leiomyoma Subclassification System (Munro 2011) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Mrs Sunita, a 38-year-old school teacher, presents with heavy, prolonged menstrual periods for the past 18 months. She soaks 8–10 pads daily for 7 days and has noticed progressive lower abdominal heaviness. She is anaemic (Hb 8.2 g/dL) and increasingly fatigued. On bimanual palpation you feel a firm, irregular, non-tender pelvic mass that moves with the cervix. A pelvic ultrasound shows multiple hypoechoic masses within the myometrium, the largest measuring 6 cm. What is your diagnosis, and how do you classify and manage this condition?
WHY THIS MATTERS
Fibroid uterus (uterine leiomyoma) is the most common benign pelvic tumour in women, estimated to be clinically significant in 25–30% of women of reproductive age and found at autopsy in up to 70–80% of women by age 50. It is the leading cause of hysterectomy in India and worldwide. A final-year student must be able to classify fibroids using the FIGO system, recognise the clinical presentations, correctly diagnose degenerations, and select appropriate management — both to avoid unnecessary surgery in women who desire fertility and to prevent harm from delayed treatment of complications such as severe anaemia or pressure symptoms.
RECALL
Before proceeding, recall the following from your earlier studies: the layers of the uterus (endometrium, myometrium, perimetrium); the role of oestrogen and progesterone in the menstrual cycle; the concept of smooth-muscle cell origin; basic pelvic anatomy including the broad ligament, round ligament, and adnexa; and the clinical approach to uterine enlargement. Recall also that leiomyomata arise from smooth muscle cells of the myometrium — the word itself means smooth-muscle tumour.
Clinical Scenario and Presentation
Fibroid uterus most commonly presents in women aged 30–50 years in the reproductive phase, and the clinical presentation depends primarily on the site, size, and number of fibroids. The classic triad is menorrhagia (heavy cyclical bleeding, the most common symptom — especially with submucosal fibroids), lower abdominal pain or pelvic pressure, and a palpable pelvic mass. Menorrhagia occurs because submucous fibroids distort the endometrial cavity and impair uterine contractility, enlarging the surface area from which bleeding occurs. Patients often develop secondary iron-deficiency anaemia from chronic blood loss, presenting with fatigue, pallor, and dyspnoea on exertion.
On abdominal examination, a fibroid uterus feels firm, irregular, and non-tender, and moves with the cervix on bimanual palpation — a feature that distinguishes it from an ovarian mass. Additional symptoms include pressure symptoms (urinary frequency from an anteriorly placed fibroid compressing the bladder, and constipation or backache from a posterior fibroid), dysmenorrhoea (particularly with submucous or intramural types), infertility, and recurrent miscarriage (especially submucous fibroids distorting the cavity). Asymptomatic fibroids discovered incidentally on ultrasound are increasingly common.
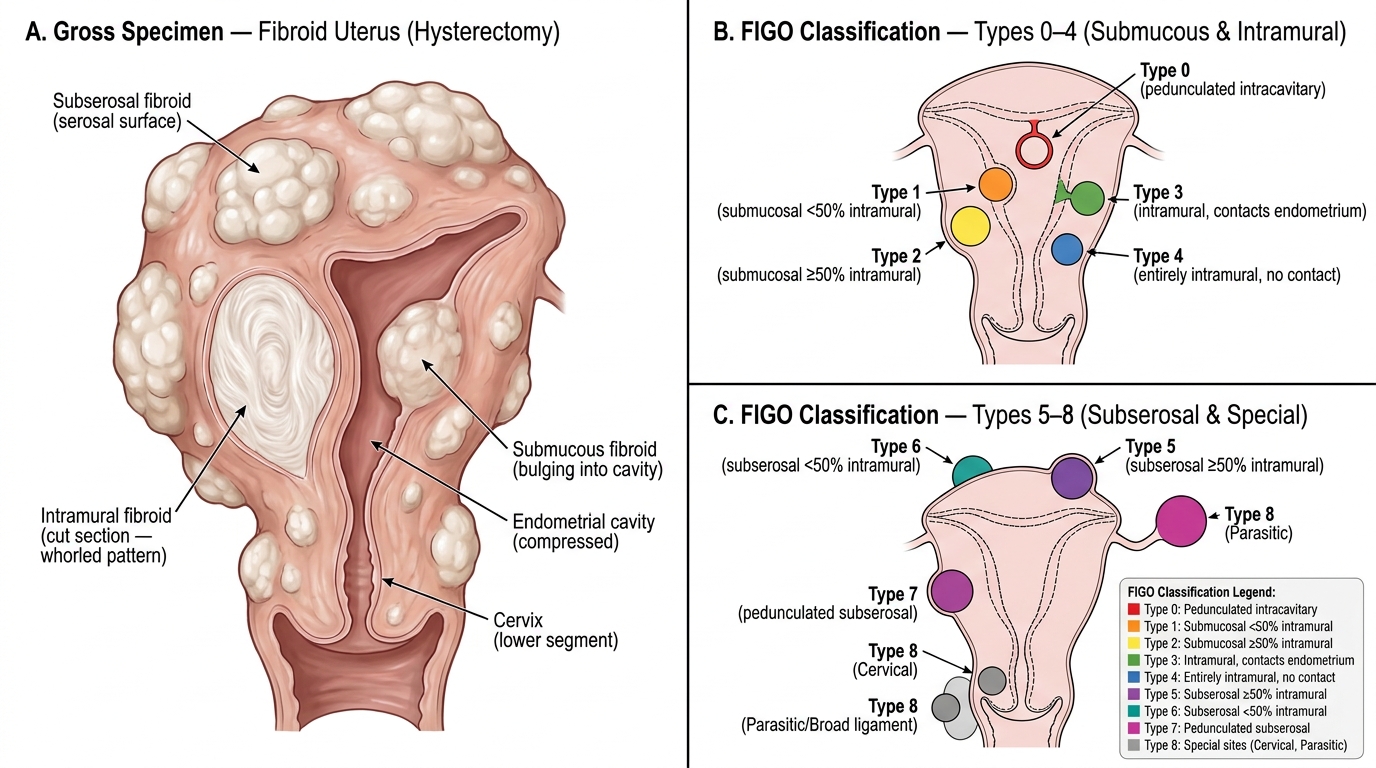
Fibroid Uterus: Gross Pathology and FIGO Leiomyoma Subclassification (Types 0–8)
Types and FIGO Leiomyoma Subclassification
The FIGO leiomyoma subclassification system (Munro, 2011) classifies fibroids by their relationship to the uterine wall and cavity, using a numerical system from 0 to 8. This classification directly guides treatment selection and prognosis, particularly for submucous fibroids where the degree of intramural extension predicts the difficulty and success of hysteroscopic resection.
FIGO type 0 is a pedunculated intracavitary fibroid with no intramural component — accessible by hysteroscope and easiest to resect. Type 1 is a submucosal fibroid with less than 50% of its diameter within the myometrium; Type 2 is submucosal with ≥50% intramural extent. Type 3 is an entirely intramural fibroid that contacts but does not breach the endometrium. Type 4 is entirely intramural with no endometrial or serosal contact. Type 5 is subserosal with ≥50% of the fibroid within the myometrium; Type 6 is subserosal with <50% intramural extent. Type 7 is a pedunculated subserosal fibroid attached by a stalk. Type 8 encompasses special locations — cervical, parasitic (detached and vascularised by adjacent structures), or broad-ligament fibroids. Types 0–3 are classified as submucous (endometrial-cavity–distorting), types 4–6 as intramural/subserosal, and a hybrid notation (e.g. 2–5) is used when a fibroid bridges two compartments.
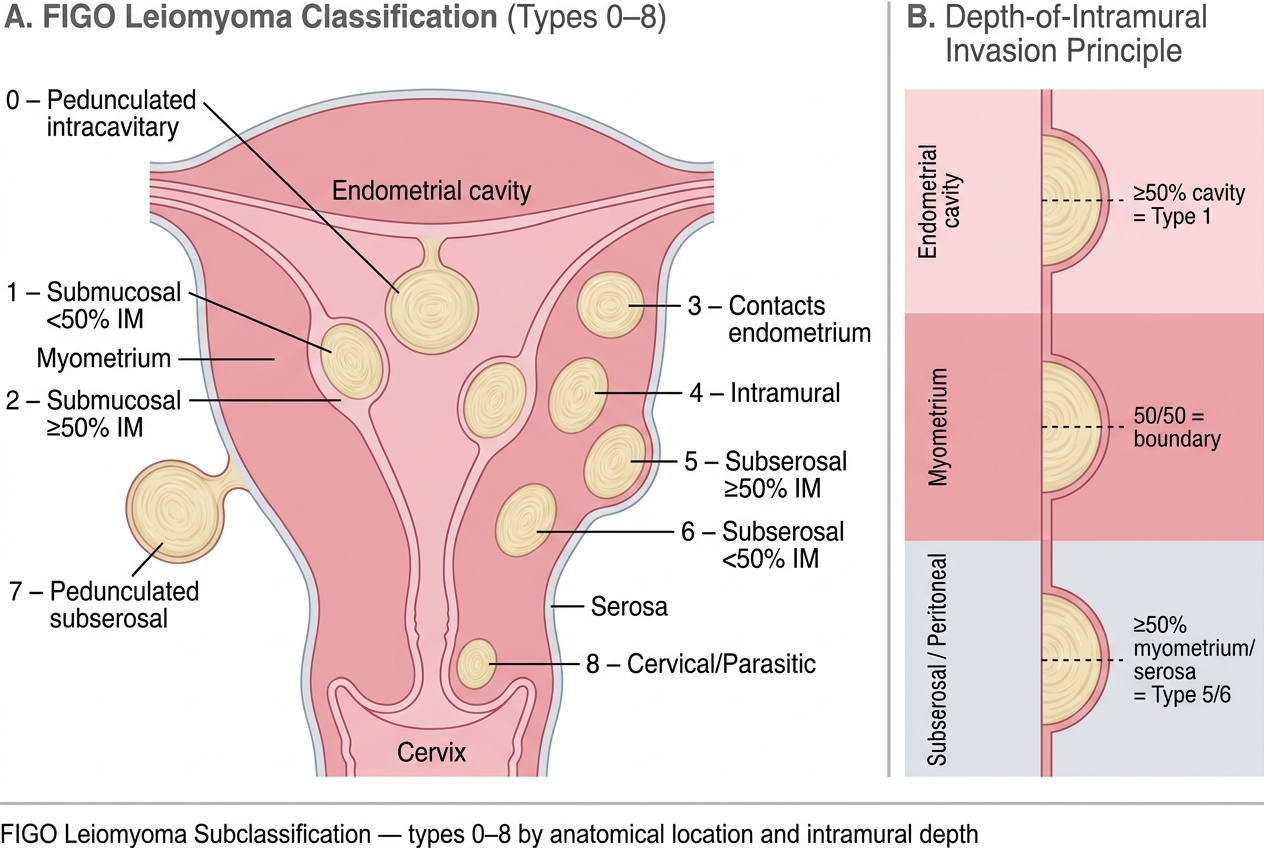
FIGO Leiomyoma Subclassification: Types 0–8 by Location and Intramural Depth
Clinically, submucous fibroids (types 0–2) are the most symptomatic for menorrhagia and infertility despite being the smallest in size. Intramural fibroids are the most common overall. Pedunculated subserosal (type 7) fibroids can tort on their pedicle, causing acute abdominal pain mimicking an ovarian torsion.
Aetiology and Pathophysiology
Fibroid uterus arises from a single smooth-muscle cell of the myometrium that undergoes clonal proliferation. The fundamental driver is oestrogen dependence: fibroids express higher concentrations of oestrogen receptors and aromatase compared to surrounding normal myometrium, and they grow during the reproductive years (when oestrogen is high), enlarge in pregnancy, and characteristically regress after menopause. This oestrogen dependence is the scientific basis of medical treatments that create a hypoestrogenic state.
The exact aetiology involves both hormonal and genetic factors. Local growth factors — especially insulin-like growth factor-1 (IGF-1) and epidermal growth factor (EGF) — mediate the mitogenic effect of oestrogen on leiomyoma cells. Somatic mutations in genes such as MED12 (found in ~70% of fibroids), HMGA2, and fumarate hydratase (FH, associated with hereditary leiomyomatosis) have been identified. Risk factors include: early menarche, nulliparity, obesity (increased peripheral aromatisation), African-American ethnicity, and family history. Protective factors include: multiparity, prolonged breastfeeding, combined oral contraceptive use (by suppressing ovulation and reducing menstrual bleeding, though the evidence is mixed), and menopause.
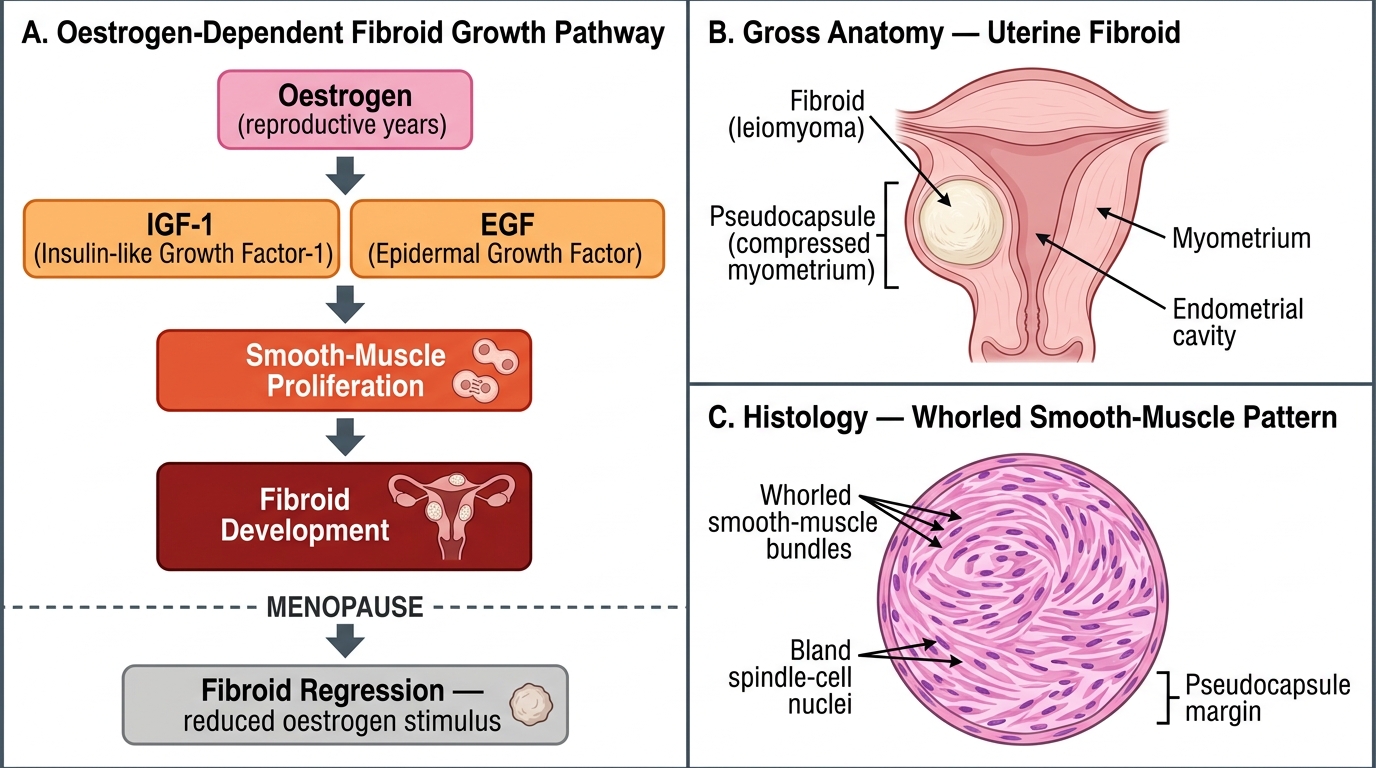
Pathogenesis and Morphology of Uterine Fibroids (Leiomyomata)
Histologically, fibroids consist of whorled bundles of smooth-muscle cells in a pseudocapsule, which is a compressed layer of surrounding myometrium. This pseudocapsule is the surgical plane exploited during myomectomy. Fibroids are typically firm, rubbery, and well-circumscribed on gross examination.