Page 2 of 24
OG29.1 | Fibroid Uterus — SDL Guide (Part 2)
Degenerations of Fibroid
As fibroids grow, they may outgrow their blood supply, leading to various forms of degeneration. Recognising degenerations is clinically important because they alter the symptoms, ultrasound appearance, and occasionally indicate a serious complication.
Hyaline degeneration is the most common — occurring in 65% of fibroids. The smooth-muscle cells are replaced by avascular hyaline material, rendering the fibroid soft, white, and glassy. It is usually asymptomatic. Cystic degeneration follows liquefaction of the hyaline material, producing fluid-filled cavities — the fibroid becomes soft and fluctuant, and may be misdiagnosed as an ovarian cyst on ultrasound.
Red (carneous) degeneration is clinically the most important, as it is the most symptomatic. It occurs most commonly during pregnancy (especially in the second trimester), when rapid growth leads to venous occlusion, haemorrhage into the substance, and aseptic necrosis. The fibroid appears brick-red on cut section. The patient presents with localised uterine tenderness, fever, leucocytosis, and pain — managed conservatively with bed rest, analgesics (paracetamol), and hydration; surgery is avoided during pregnancy.
Calcific degeneration is common in postmenopausal women; calcium salts are deposited, making the fibroid extremely hard and producing a radio-opaque shadow on plain X-ray (a diagnostic clue). Sarcomatous change (malignant degeneration) is rare, occurring in <0.5% of fibroids, and should be suspected when a fibroid grows rapidly — especially in a postmenopausal woman or when there is unexpected rapid increase in uterine size.
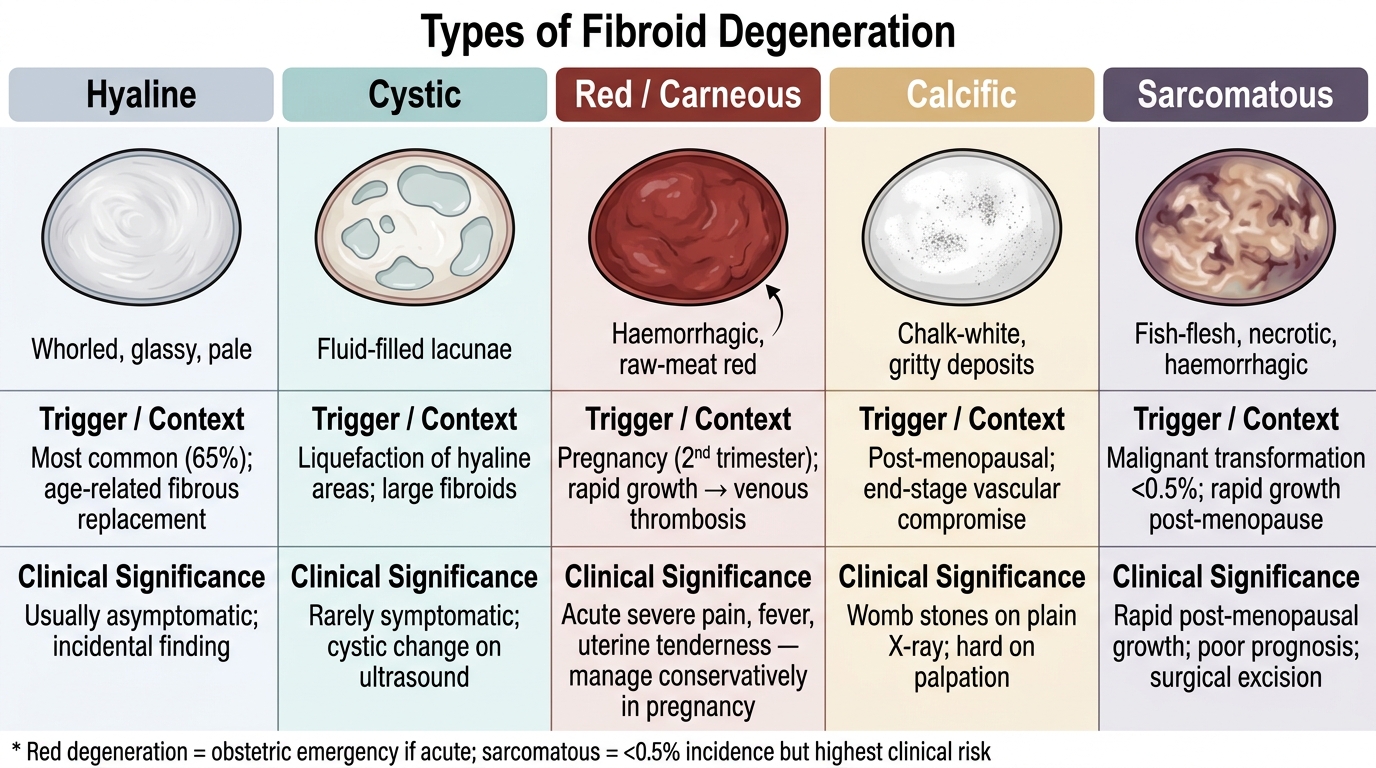
Types of Fibroid Degeneration: Macroscopic Appearance, Triggers, and Clinical Significance
Additional less-common degenerations include myxomatous (mucinous) and fatty (lipomatous) change. The fatty degeneration is visible on MRI as high-signal-intensity areas and may indicate leiomyolipoma.
Complications of Fibroid Uterus
Fibroids can cause a wide spectrum of complications, broadly categorised as local, reproductive, and potentially life-threatening. Understanding these complications provides the rationale for treatment.
Menorrhagia and anaemia are the most common complication, resulting from endometrial distortion (submucous types) and impaired myometrial contractility. Chronic blood loss leads to iron-deficiency anaemia, which may be severe enough to require blood transfusion before definitive surgery. Pressure effects depend on location: anterior fibroids compress the bladder (urinary frequency, urgency, incomplete emptying), and large posterior fibroids compress the rectum (constipation) or ureters (hydronephrosis, rarely). Torsion of a pedunculated subserosal fibroid (type 7) is a gynaecological emergency causing acute severe lower abdominal pain. Infection and suppuration can occur in submucous fibroids that protrude into the vagina. Infertility results from mechanical distortion of the tubal ostia, endometrial cavity, or cervix — types 0–3 have the greatest impact. Recurrent pregnancy loss is associated with submucous fibroids distorting the implantation site. Obstetric complications include malpresentation, preterm labour, placenta praevia (if fibroids are in the lower segment), obstructed labour, and postpartum haemorrhage due to atonic uterus. Malignant change (leiomyosarcoma), while rare (<0.5%), is the most feared long-term complication.
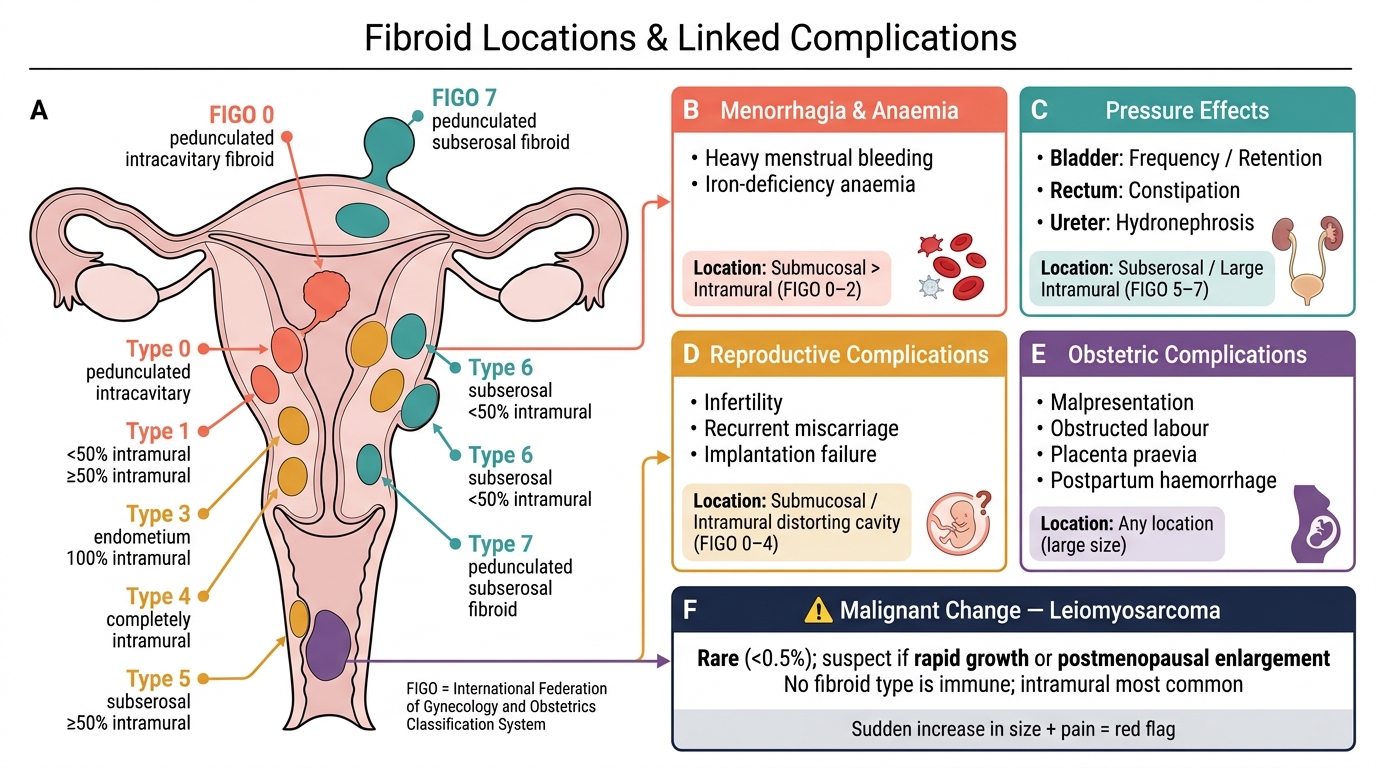
Fibroid Uterus: Complications by Category Linked to Fibroid Location (FIGO Classification)
SELF-CHECK
A 35-year-old nulliparous woman has a 4 cm fibroid entirely within the uterine cavity, attached by a stalk, with no intramural component. What is the FIGO leiomyoma subclassification?
A. FIGO Type 0 (pedunculated intracavitary)
B. FIGO Type 1 (submucosal, <50% intramural)
C. FIGO Type 2 (submucosal, ≥50% intramural)
D. FIGO Type 3 (contacts endometrium, 100% intramural)
Reveal Answer
Answer: A. FIGO Type 0 (pedunculated intracavitary)
FIGO Type 0 is specifically a pedunculated intracavitary fibroid with no intramural extension. It is the most amenable to hysteroscopic resection and has the highest symptom-to-size ratio for menorrhagia. Type 1 and 2 have progressively greater intramural extension, and Type 3 is entirely intramural but contacts the endometrium without distorting the cavity.
Diagnosis and Investigations
The diagnosis of fibroid uterus is primarily clinical, confirmed by ultrasound, and further delineated by additional imaging or endoscopic studies when needed. A structured approach prevents both under-investigation (missing a submucosal fibroid or degeneration) and over-investigation.
Clinical examination: Abdominal palpation reveals a firm, irregular, non-tender pelvic mass arising from the pelvis. Bimanual pelvic examination demonstrates a firm, irregular, enlarged uterus that moves with the cervix — distinguishing it from an ovarian mass (which moves independently of the cervix). The mass is non-fluctuant and non-tender unless degeneration has occurred. Speculum examination may reveal a submucous fibroid protruding through the cervix.
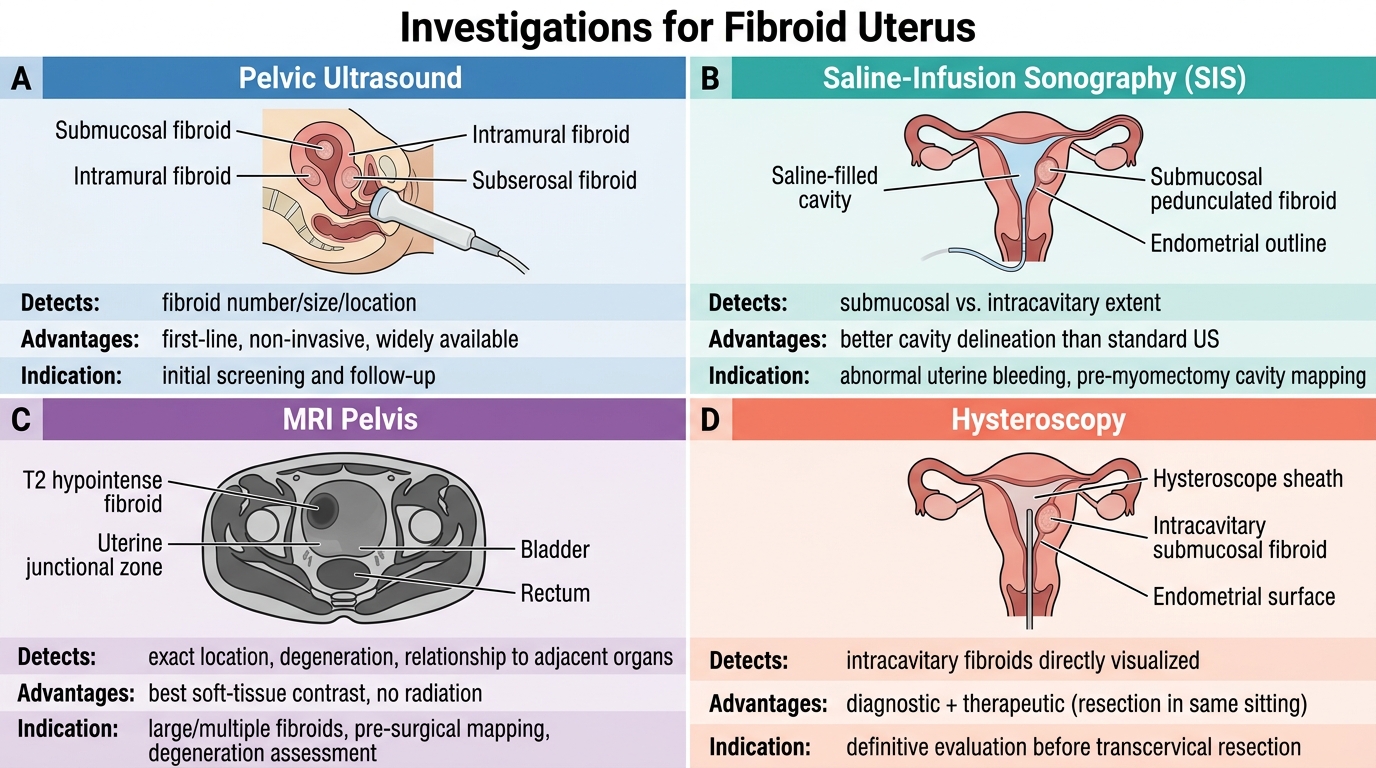
Pelvic ultrasound (transvaginal or transabdominal) is the first-line investigation — it identifies the number, size, location (FIGO classification), and echogenicity of fibroids. Fibroids typically appear as well-defined, hypoechoic to isoechoic, solid masses with posterior shadowing. Colour Doppler shows a peripheral vascular pattern. Saline-infusion sonography (SIS/sonohysterography) is useful for delineating the degree of intrauterine extension of submucous fibroids (differentiating types 0, 1, and 2) and for detecting endometrial polyps. MRI is the gold standard for complete fibroid mapping when surgery is planned — it accurately delineates size, number, and location (including broad-ligament and cervical fibroids), characterises degenerations, and is superior to ultrasound for multiple or large fibroids. Hysteroscopy directly visualises the uterine cavity and is essential for diagnosing and treating submucous fibroids (types 0–2).
Laboratory investigations: Full blood count (to assess anaemia), serum ferritin (iron stores), LFT, RFT (if hydronephrosis suspected), and thyroid function (to exclude hypothyroidism as a cause of menorrhagia). An endometrial biopsy or D&C is indicated if there is suspicion of endometrial pathology — particularly in women over 40 with abnormal uterine bleeding. Serum CA-125 may be elevated in large fibroids but is non-specific.
Investigations for Fibroid Uterus: Comparative Overview