Page 9 of 37
OG33.5 | Benign and Premalignant Cervical Lesions — SDL Guide
Learning Objectives
- Distinguish benign cervical lesions (ectropion, nabothian cysts, polyps, cervicitis) from premalignant CIN on clinical and histological grounds
- Describe the natural history of CIN grades 1, 2, and 3 including spontaneous regression and progression rates
- Outline the principles of management of CIN using ablative methods (cryotherapy, thermal ablation) and excisional methods (LEEP, cold-knife cone biopsy)
- State the eligibility criteria for cryotherapy versus LEEP and describe the freeze-thaw-freeze protocol
- Identify the complications of cryotherapy and LEEP and outline post-treatment surveillance
INSTRUCTIONS
Most women referred for colposcopy after an abnormal screening result will be found to have either a benign cervical lesion (requiring reassurance and simple management) or a pre-invasive CIN lesion (requiring directed treatment to prevent progression to invasive cancer). This module gives you the clinical reasoning framework to distinguish these entities, understand their natural history, and apply the correct management strategy — knowledge that is directly tested in final MBBS and is essential for gynaecology outpatient practice.
References
- DC Dutta's Textbook of Gynaecology, 8th edition, Chapters 24 and 33 (textbook)
- Shaw's Textbook of Gynaecology, 17th edition (textbook)
- WHO Guidelines for Screening and Treatment of Cervical Pre-cancer Lesions, 2nd edition, 2021 (guideline)
- Ostor AG. Natural history of cervical intraepithelial neoplasia: a critical review. Int J Gynecol Pathol. 1993;12(2):186-92. (journal)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman attends the gynaecology outpatient clinic with a history of intermenstrual spotting and postcoital bleeding for three months. On speculum examination, you see a reddish, granular-appearing area surrounding the external os. A routine Pap smear returns as HSIL. Colposcopy reveals a dense acetowhite area with sharp borders and coarse punctation confined to the transformation zone; the entire squamocolumnar junction is visible. You take a directed biopsy. The histology report reads: 'CIN 2, involving the lower two-thirds of the epithelium. No evidence of invasion.' Her partner asks whether she has cancer. She asks whether her cervix will need to be removed. How do you counsel her, and what treatment will you offer? This module gives you the knowledge to answer both questions confidently.
WHY THIS MATTERS
Cervical ectropion and CIN together account for the majority of colposcopy referrals in a gynaecology outpatient clinic. The ability to distinguish a benign cervical lesion (which merely needs reassurance or simple treatment) from a premalignant CIN lesion (which requires definitive treatment to prevent invasive cancer) is a core clinical competency. In final MBBS examinations, the management of CIN — particularly the indications for cryotherapy versus LEEP, the freeze-thaw-freeze protocol, and the eligibility criteria for ablative versus excisional treatment — is a frequently tested topic. Moreover, understanding the natural history of CIN (that most CIN 1 regresses and does not require treatment, while CIN 3 has a substantial long-term risk of invasion without treatment) is essential for appropriate counselling and follow-up decisions.
RECALL
Recall the following: (1) The transformation zone (TZ) is the region of the cervix targeted by all screening tests; it is where squamous metaplasia creates conditions for HPV integration and CIN development. (2) CIN is graded by the proportion of the epithelial thickness replaced by dysplastic cells: CIN 1 = lower one-third (corresponding to LSIL), CIN 2 = lower two-thirds, CIN 3 = greater than two-thirds to full thickness, including carcinoma in situ (both CIN 2 and CIN 3 correspond to HSIL). (3) Colposcopy uses magnification and acetic acid to grade lesions: Grade 1 (minor — thin acetowhite, fine punctation/mosaic) and Grade 2 (major — dense acetowhite, coarse punctation/mosaic, sharp geographic borders) per the IFCPC 2011 classification. (4) A satisfactory colposcopy means the entire TZ and squamocolumnar junction are visible — a prerequisite for accurate directed biopsy and for cryotherapy eligibility.
Clinical Presentation of Benign and Premalignant Cervical Lesions
Benign and premalignant cervical lesions share a common clinical presentation — they may all cause contact bleeding, abnormal discharge, or an abnormal-looking cervix on speculum examination — and the clinician's first responsibility is to distinguish between them on both clinical grounds and histology. Pre-invasive CIN typically produces no symptoms at all; it is usually detected incidentally on a routine Pap smear or VIA screening test. When symptoms are present, they may overlap entirely with benign causes, which is why all symptomatic or visually abnormal cervices must be investigated with Pap smear and, where indicated, colposcopy-directed biopsy.
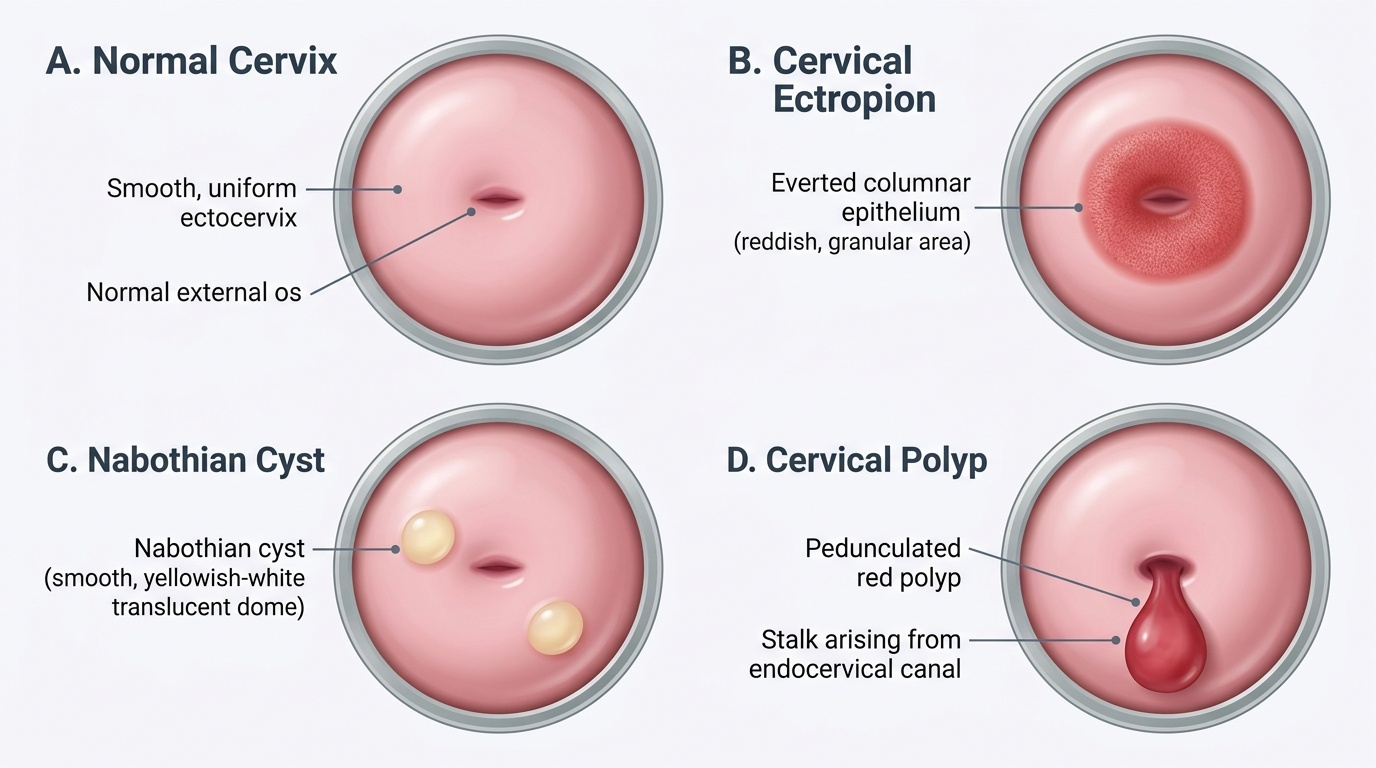
Cervical ectropion (also called ectopy or erosion — the latter term is a misnomer as there is no ulceration) is the most common benign cervical finding. It occurs when the columnar epithelium of the endocervical canal is everted onto the ectocervix, appearing as a reddish, velvety granular area surrounding the external os. It is physiological in adolescents and pregnant women (under the influence of oestrogen) and is seen in women taking combined oral contraceptives. Symptoms include excess mucoid discharge and postcoital spotting from the fragile columnar epithelium. The cervix is smooth and non-indurated on palpation — hardness suggests malignancy. Biopsy shows benign columnar mucosa only.
Nabothian cysts (mucus retention cysts) appear as smooth, yellowish, translucent domes on the ectocervix, resulting from blockage of the ducts of endocervical glands during squamous metaplasia. They are entirely benign, require no treatment, and are important to recognise to avoid unnecessary biopsy.
Cervical polyps are pedunculated growths arising from the endocervical mucosa, typically reddish, soft, and visible through the external os. They cause intermenstrual and postcoital bleeding. Management is polypectomy (twist-off or surgical removal at the pedicle) with histological examination of the specimen — rarely, a polyp may harbour CIN or carcinoma.
Cervicitis (acute: mucopurulent discharge, contact bleeding; chronic: firm, congested cervix) is usually caused by Neisseria gonorrhoeae, Chlamydia trachomatis, or mixed flora. Treatment is organism-directed antibiotic therapy. Untreated chlamydial cervicitis ascends to cause pelvic inflammatory disease; importantly, it can mimic CIN or ectropion on speculum inspection and must be excluded microbiologically before cryotherapy.
Provided image
Pathophysiology: Natural History of CIN and Benign Lesions
Understanding the natural history of CIN is the foundation of all management decisions, because it explains why CIN 1 can be observed safely while CIN 2/3 must be treated, and why the aim of treatment is prevention rather than cure of an existing malignancy. The natural history has been characterised through prospective cohort studies (most notably the landmark Ostor review of 1993, and the McCredie et al. New Zealand study of 2008) and shows a spectrum of outcomes depending on grade.
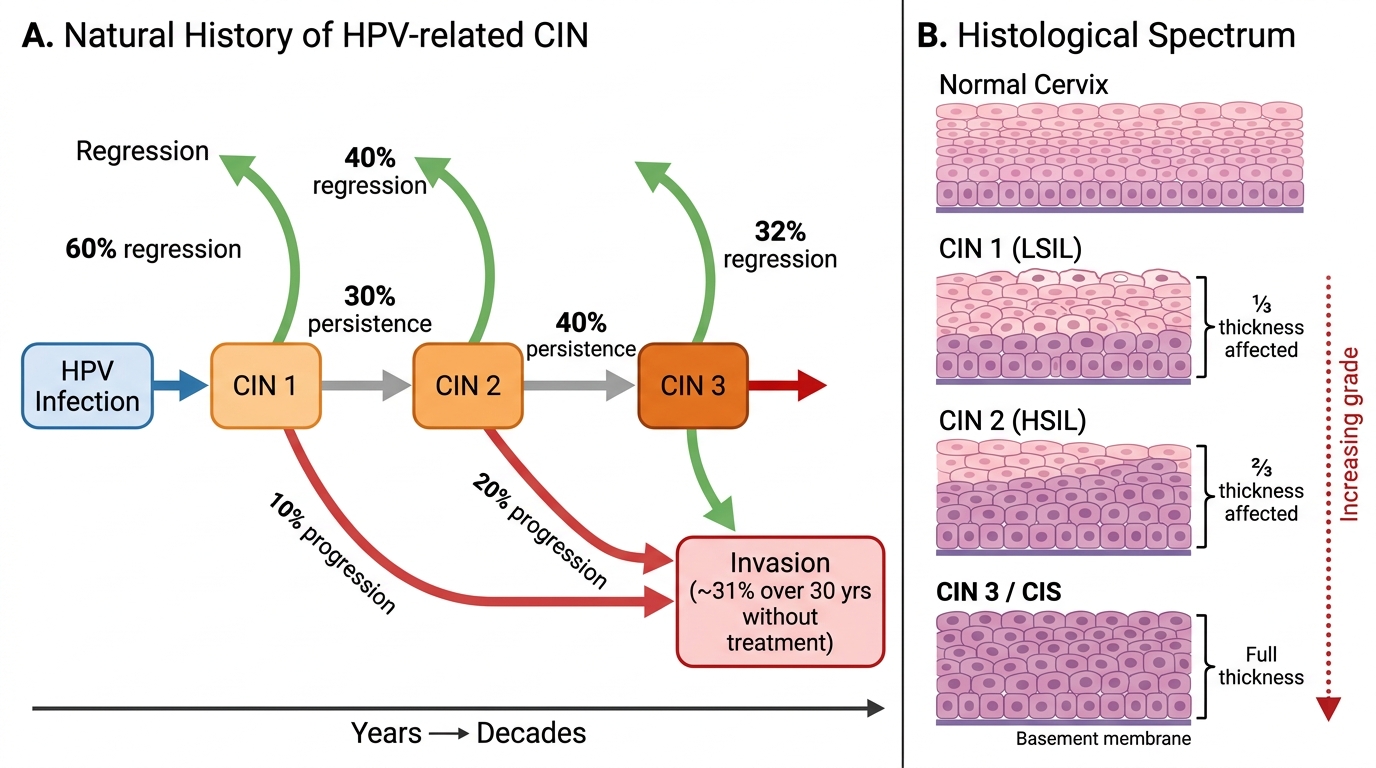
CIN 1 (LSIL, lower-third dysplasia, HPV cytopathic effect) represents a productive HPV infection with cytopathic changes and mild dysplasia. Approximately 60% of CIN 1 lesions regress spontaneously within 12–24 months as the immune system clears the HPV infection. Approximately 30% persist, and approximately 10% progress to CIN 2/3. Because spontaneous regression is the commonest outcome, the current evidence-based recommendation is surveillance rather than immediate treatment for CIN 1 — repeat colposcopy and cytology at 6–12 monthly intervals, with treatment only if the lesion persists beyond 24 months or progresses.
CIN 2 (HSIL, lower two-thirds dysplasia) occupies a transitional position. Regression occurs in approximately 40% of cases, persistence in approximately 40%, and progression to CIN 3 or invasion in approximately 20%. Because CIN 2 in women over 25 has a significant progression risk, and because regression cannot be reliably predicted at the individual level, treatment is recommended for most CIN 2 in adult women. In adolescents and young women aged <25 where regression rates are higher, a period of observation may be considered per local guidelines.
CIN 3 (carcinoma in situ, full-thickness dysplasia) has a high risk of progression to invasive cancer without treatment. The landmark McCredie study estimated an approximately 31% cumulative 30-year risk of invasive cancer in untreated CIN 3 (from the New Zealand study where women had their treatment withheld for research — now considered an ethical violation). All CIN 3 requires treatment, and there is no role for surveillance in confirmed CIN 3 in the current guidelines. The interval between CIN 3 and invasive cancer (typically 10–15 years) is the therapeutic window that cervical screening exploits.
Natural History of HPV-related CIN and Histological Grading
SELF-CHECK
A 26-year-old woman is found to have CIN 1 on directed biopsy after a Pap smear showing LSIL. She is otherwise healthy and HPV-negative on reflex testing. What is the most appropriate initial management?
A. Immediate cryotherapy to prevent progression
B. LEEP excision to obtain a histological specimen
C. Surveillance with repeat colposcopy and cytology at 12 months
D. Hysterectomy as definitive treatment
Reveal Answer
Answer: C. Surveillance with repeat colposcopy and cytology at 12 months
CIN 1 has a ~60% spontaneous regression rate and only ~10% progression risk; immediate treatment is not indicated. Surveillance with repeat colposcopy and cytology at 12 months (or 6 months if HPV-positive) is the evidence-based approach. Treatment is reserved for lesions that persist beyond 24 months or progress. Hysterectomy is never first-line for CIN — it is a last resort for recurrent disease after excisional treatment.
Diagnosis: Colposcopy, Biopsy, and Histological Classification
The diagnosis of CIN and its grade requires histological confirmation from a colposcopy-directed biopsy. Colposcopy alone can characterise the likely grade of lesion, but histology is the gold standard and is mandatory before any irreversible treatment is undertaken.
At colposcopy (after acetic acid application), the features that distinguish low-grade from high-grade disease are summarised by the IFCPC 2011 colposcopic classification. Grade 1 (minor) changes suggesting CIN 1 include: thin, translucent acetowhite epithelium with irregular, feathery borders; fine punctation or mosaic with regular spacing; geographic irregular margins. Grade 2 (major) changes suggesting CIN 2/3 include: dense, opaque acetowhite epithelium that appears rapidly and persists; coarse punctation or mosaic with irregular, widely spaced vessels; sharp, geographic or inner (ridge-sign, inner border sign) borders; extension to the squamocolumnar junction. Atypical vessels (irregular calibre, non-arborizing, corkscrew or spaghetti-type) raise the suspicion of frank invasion and should prompt urgent biopsy and haemostasis preparation. Additional features suggesting high-grade disease include: acetowhite iodine-negative areas on VILI, lesion abutting the SCJ, and large lesion size.
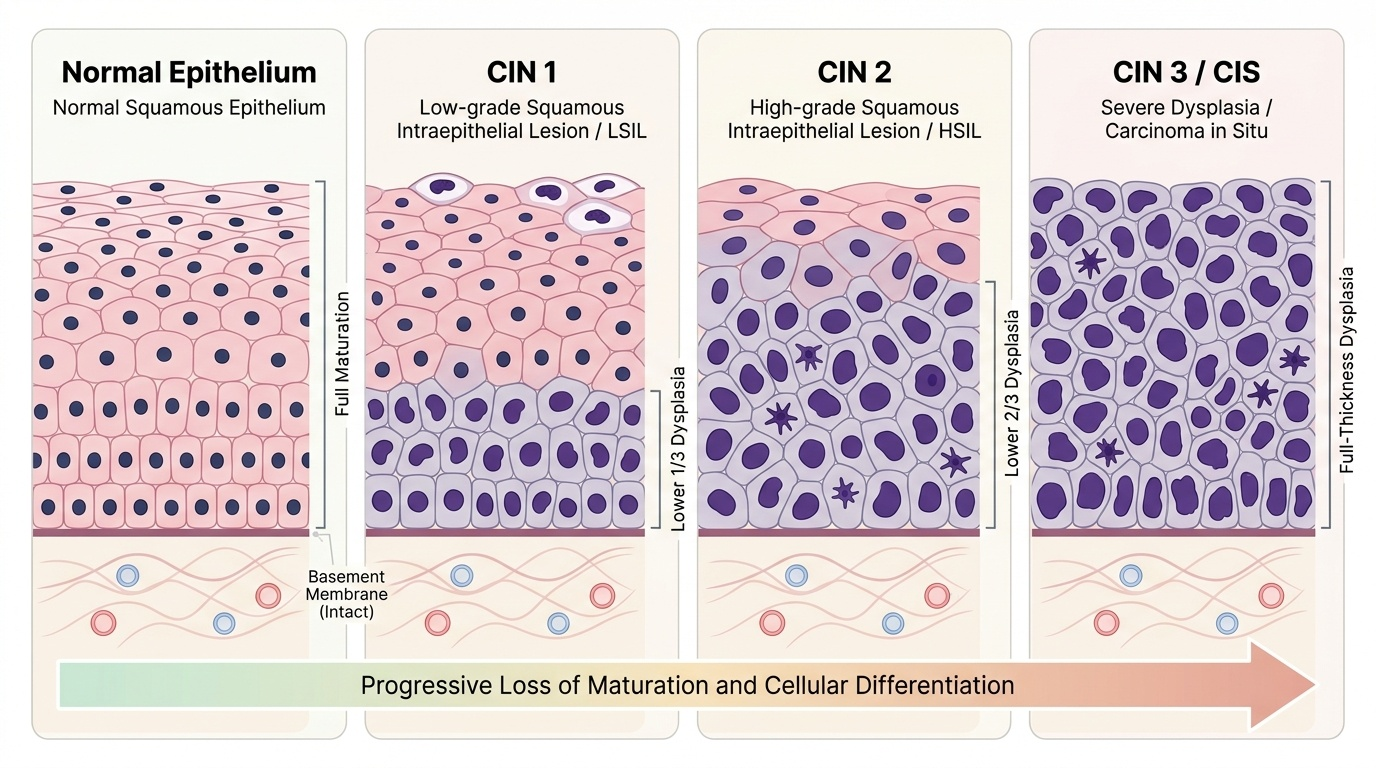
Directed punch biopsy from the most abnormal area (densest acetowhite, coarsest punctation) provides the diagnostic specimen. Multiple biopsies (2–4) are taken when the abnormality is extensive or multifocal. When the SCJ is not fully visible (unsatisfactory colposcopy), endocervical curettage (ECC) is added to sample the canal. The biopsy is processed by standard formalin fixation and haematoxylin-eosin staining. The pathologist reports the proportion of epithelial thickness replaced by dysplastic cells and assigns CIN 1, 2, or 3 (or the WHO-preferred designation SIL = squamous intraepithelial lesion, low or high grade). A report of 'CIN not excludable' or 'microinvasive carcinoma' should trigger cone biopsy.
Provided image