Page 10 of 37
OG33.5 | Benign and Premalignant Cervical Lesions — SDL Guide (Part 2)
Management of Benign Cervical Lesions
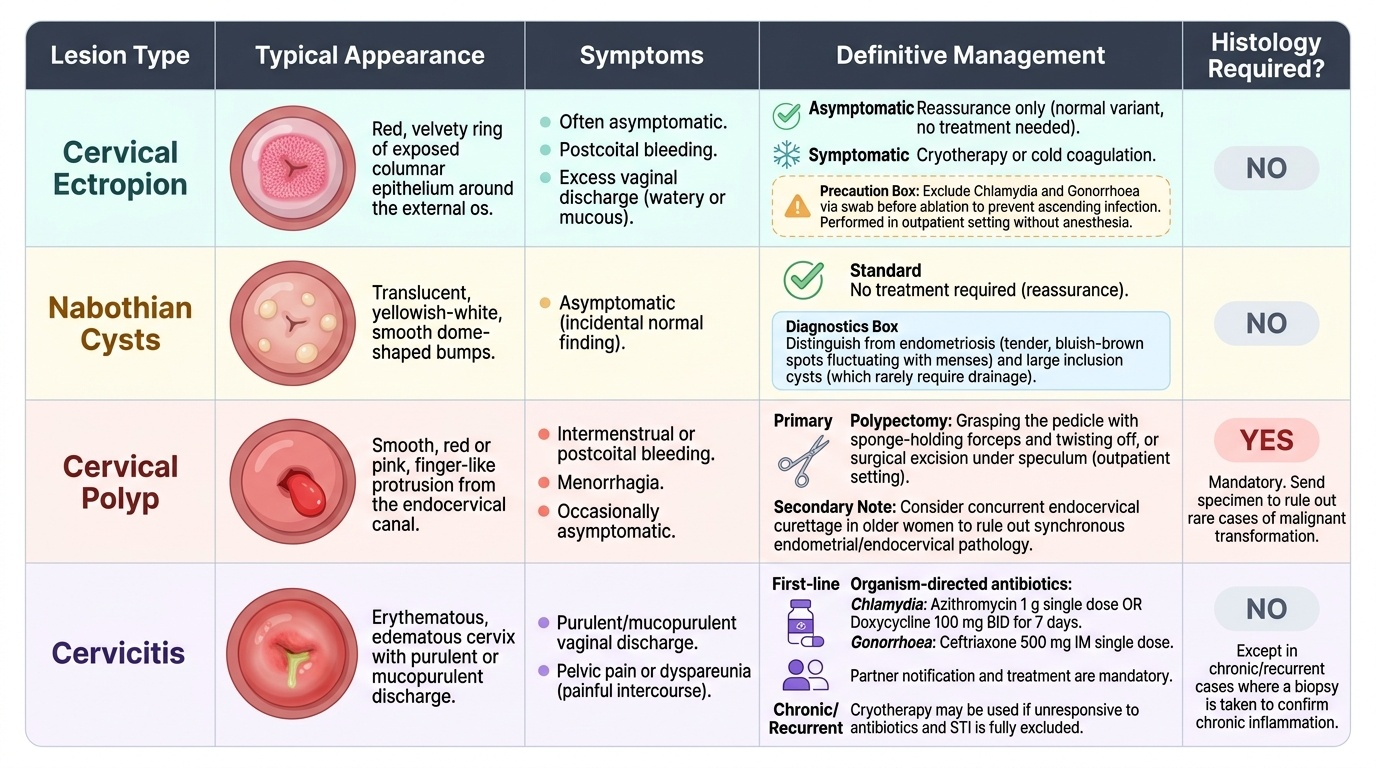
Benign cervical lesions are common and frequently alarming to patients who worry about cancer. Accurate diagnosis and confident management with appropriate counselling is therefore as clinically important as the treatment itself.
Cervical ectropion in an asymptomatic woman requires no treatment — reassurance that it is a normal variant is sufficient. When symptoms (postcoital bleeding, excess discharge) are troublesome, cryotherapy or cold coagulation destroys the columnar epithelium and promotes squamous re-epithelialisation. Before any ablative treatment, chlamydia and gonorrhoea must be excluded by cervical swab, as treating active infection with ablation can cause ascending spread. The procedure is performed in an outpatient setting without anaesthesia; mild cramping during the freeze is expected. After treatment, a watery discharge for 2–4 weeks is normal as the necrotic tissue sloughs.
Nabothian cysts are asymptomatic normal findings and require no treatment. They must be distinguished from endometriosis deposits on the cervix (which are bluish-brown, tender, and fluctuate with the menstrual cycle) and from large inclusion cysts, which may rarely require drainage.
Cervical polyps are treated by polypectomy — grasping the pedicle with sponge-holding forceps and twisting it off, or surgical excision under speculum in an outpatient setting. A curettage of the endocervical canal is sometimes performed simultaneously to check for synchronous endometrial or endocervical pathology in older women. The specimen must always be sent for histological examination, as rare cases of malignant transformation have been reported in cervical polyps.
Cervicitis requires organism-directed antibiotics: uncomplicated chlamydial cervicitis is treated with azithromycin 1 g single dose or doxycycline 100 mg twice daily for 7 days; gonococcal cervicitis with ceftriaxone 500 mg IM single dose (per current resistance-informed guidelines). Partner notification and treatment are mandatory. Recurrent or chronic cervicitis unresponsive to antibiotics, or with histological features of chronic inflammation on biopsy, may be treated with cryotherapy after exclusion of STI.
Provided image
Management of CIN: Ablative and Excisional Methods
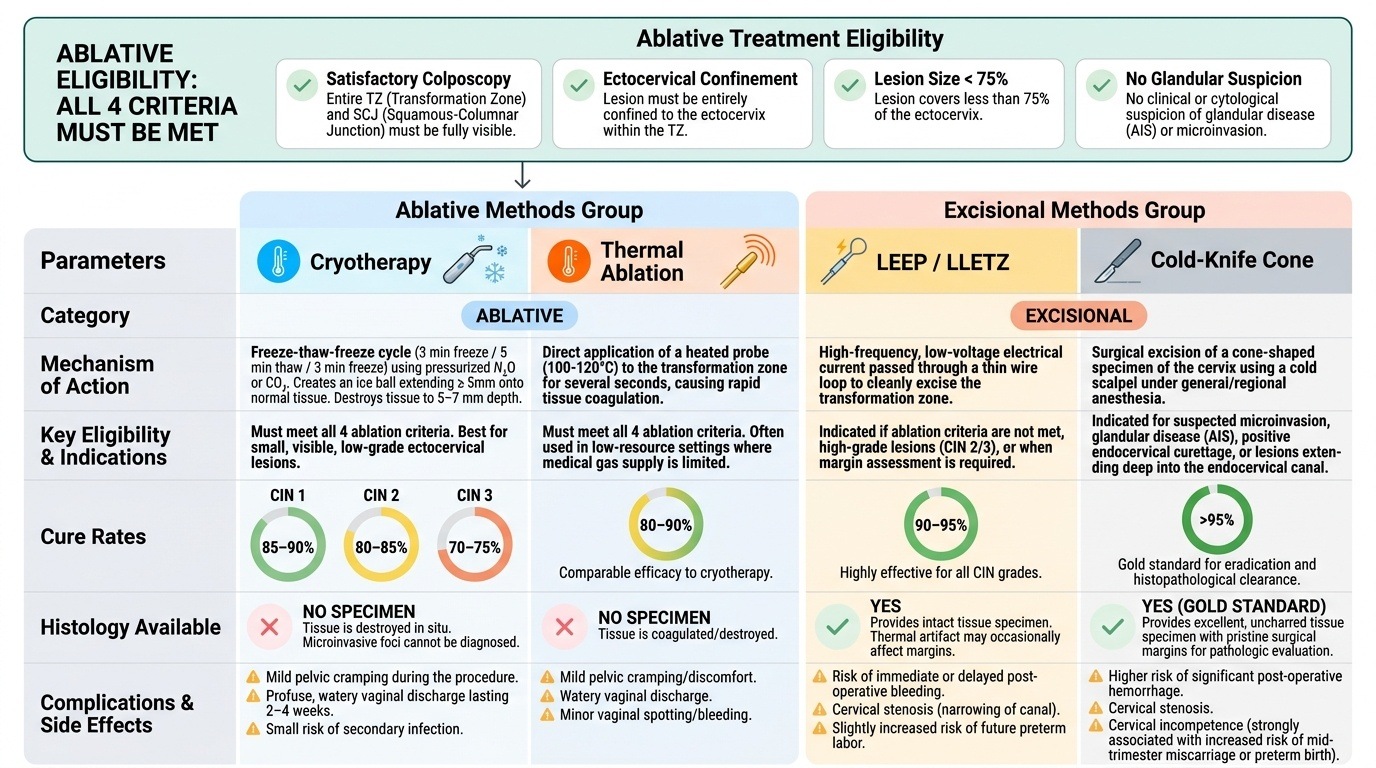
Management of CIN 2 and CIN 3 requires either ablation (destruction of the abnormal transformation zone tissue in situ) or excision (surgical removal of the TZ for both treatment and histological examination). The choice between methods is determined by whether the lesion is eligible for ablation, whether a histological specimen is required, and whether glandular involvement or microinvasion must be excluded.
Eligibility for ablative treatment requires all four criteria to be met: (1) satisfactory colposcopy (entire TZ and SCJ visible), (2) lesion confined to the ectocervix within the TZ, (3) lesion covering less than 75% of the ectocervix, and (4) no suspicion of glandular disease (adenocarcinoma in situ) or invasion. If any criterion is not met, excisional treatment (LEEP or cone biopsy) is mandatory.
Cryotherapy destroys the TZ by application of a metal cryoprobe (cooled by pressurised nitrous oxide or CO₂ gas) directly onto the cervix. The standard protocol is the freeze-thaw-freeze cycle: freeze for 3 minutes (ice ball must extend at least 5 mm beyond the probe edge onto normal tissue to ensure adequate depth), thaw for 5 minutes at room temperature, then freeze again for 3 minutes. This double-freeze technique destroys tissue to approximately 5–7 mm depth and is effective for small, eligible TZ lesions (CIN 1/2). Cure rates are approximately 85–90% for CIN 1, 80–85% for CIN 2, and somewhat lower (~70–75%) for CIN 3, which is why many guidelines prefer excisional treatment for CIN 3. Cryotherapy does not provide a histological specimen — this is a key limitation, as any microinvasive focus in the lesion would be destroyed without diagnosis. Side effects include cramping during the procedure, a profuse watery discharge for 2–4 weeks (patient counselling essential), and a small risk of secondary infection.
Thermal ablation (cold coagulation) uses a heated probe (100–120°C) applied to the TZ for several seconds; despite the name 'cold coagulation', it destroys tissue by heat. It has comparable efficacy to cryotherapy and is used where cryotherapy gas supply is unavailable. Similar eligibility criteria apply.
LEEP (loop electrosurgical excision procedure) — also called LLETZ (large loop excision of the transformation zone) — uses a thin wire loop energised by a diathermy current to excise the entire TZ as a single specimen. It is performed under local anaesthesia (cervical ring block with 1% lignocaine with adrenaline). The LEEP specimen provides full histological assessment of the excised tissue, allowing confirmation of CIN grade, assessment of deep and lateral margins (clearance), and exclusion of microinvasion — a major advantage over ablative methods. LEEP is the treatment of choice for CIN 2/3, for lesions not meeting ablation eligibility criteria, and whenever glandular disease cannot be excluded. Thermal artefact at the resection margins may reduce histological interpretability. Complications include: primary haemorrhage (during procedure, managed by diathermy or sutures), secondary haemorrhage (7–14 days post-procedure, from sloughing eschar, may require silver nitrate cautery or re-suturing), cervical stenosis (particularly in women with small cervices or after deep excision), and theoretical risk of cervical incompetence / preterm labour with repeated deep excisions.
Cold-knife cone biopsy (CKC) uses a scalpel under general or regional anaesthesia to excise a cone-shaped portion of the cervix including the entire TZ. It provides the cleanest histological margins (no thermal artefact) and the largest specimen, making it the gold standard when: (a) the colposcopic-cytological discordance is significant (e.g. cytology suggests HSIL but biopsy shows only CIN 1), (b) microinvasion is suspected on biopsy or colposcopy, (c) glandular involvement (AIS — adenocarcinoma in situ) is present, (d) the lesion extends high into the endocervical canal, or (e) LEEP has failed or margins are involved. CKC has a higher risk of haemorrhage and cervical incompetence than LEEP.
Provided image
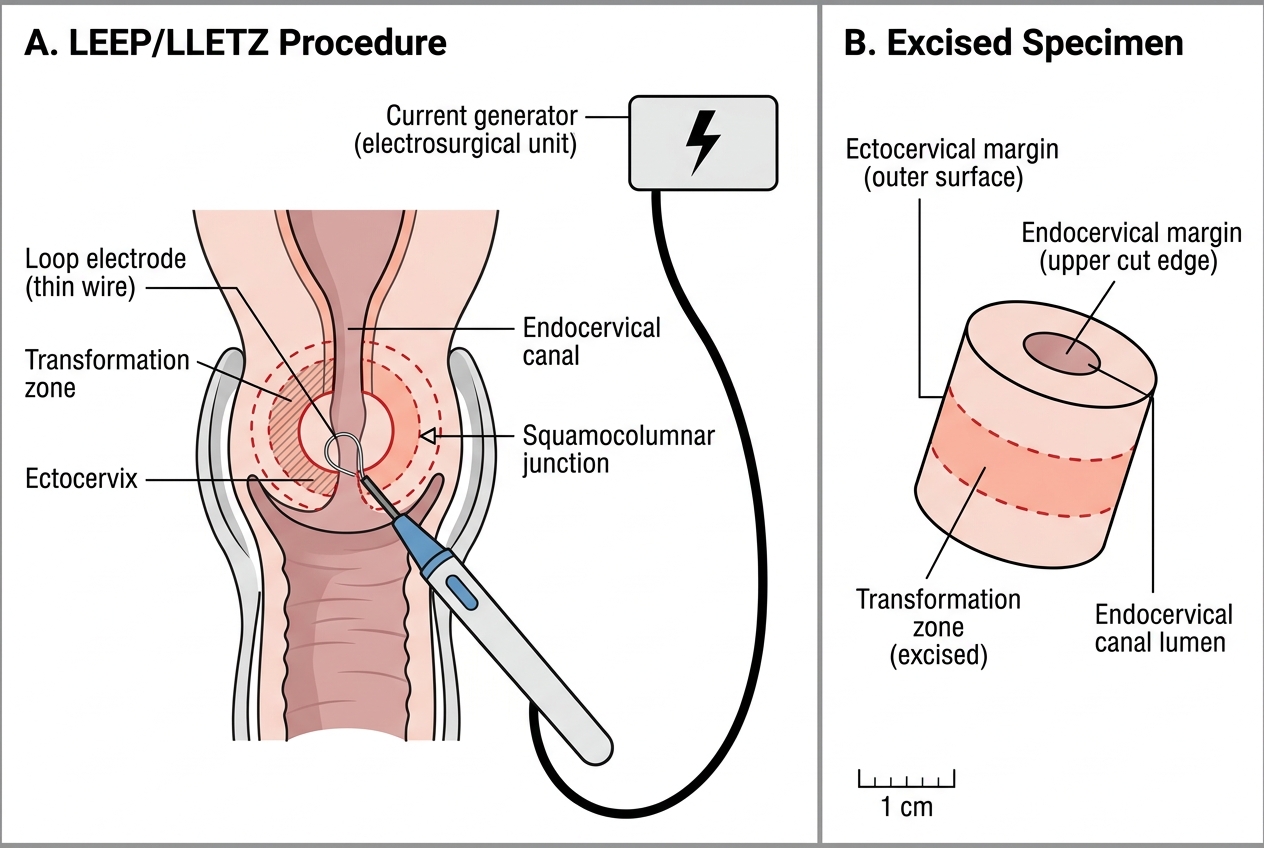
LEEP/LLETZ Procedure: Loop Electrode Excision of the Transformation Zone
SELF-CHECK
A 35-year-old woman is found to have CIN 3 on colposcopy-directed biopsy. Colposcopy shows that the lesion extends into the endocervical canal and the squamocolumnar junction cannot be fully visualised. Which treatment is most appropriate?
A. Cryotherapy — freeze-thaw-freeze protocol
B. Thermal ablation
C. LEEP/LLETZ
D. Cold-knife cone biopsy
Reveal Answer
Answer: D. Cold-knife cone biopsy
When the squamocolumnar junction cannot be fully visualised (unsatisfactory colposcopy) or the lesion extends into the endocervical canal, ablative methods (cryotherapy, thermal ablation) are contraindicated because the full extent of the lesion cannot be assessed. LEEP is also insufficient when the lesion extends high into the canal (risk of incomplete excision). Cold-knife cone biopsy (CKC) is the treatment of choice for endocervical lesions with poor colposcopic visualisation — it provides the largest, deepest specimen with clean thermal-artefact-free margins.
Self-Assessment
Before reviewing the summary, test your recall by answering these consolidation questions: Which CIN grade most commonly regresses spontaneously? (CIN 1.) What is the untreated 30-year cumulative invasion risk of CIN 3? (~31% per McCredie et al.) What are the four eligibility criteria for ablative treatment (cryotherapy/thermal ablation)? (Satisfactory colposcopy, lesion confined to TZ, <75% ectocervix, no glandular/invasion suspicion.) What is the freeze-thaw-freeze protocol for cryotherapy? (Freeze 3 min → thaw 5 min → freeze 3 min.) When is cold-knife cone biopsy preferred over LEEP? (Endocervical lesion with poor visualisation, microinvasion suspected, glandular involvement, CKC histology needed with clean margins.) What distinguishes LEEP from cryotherapy in terms of diagnostic value? (LEEP provides a histological specimen for margin assessment; cryotherapy does not.)
A key examination scenario type: 'A woman has CIN 2 on biopsy. Colposcopy is satisfactory and the lesion is small, confined to the TZ, with no glandular features. What is the preferred treatment?' — Answer: Either cryotherapy (if eligible and LEEP not available) or LEEP/LLETZ (preferred because it provides histology). 'The same woman has a lesion that extends into the canal.' — Answer: LEEP or CKC (ablative methods contraindicated; endocervical extension violates eligibility for cryotherapy).
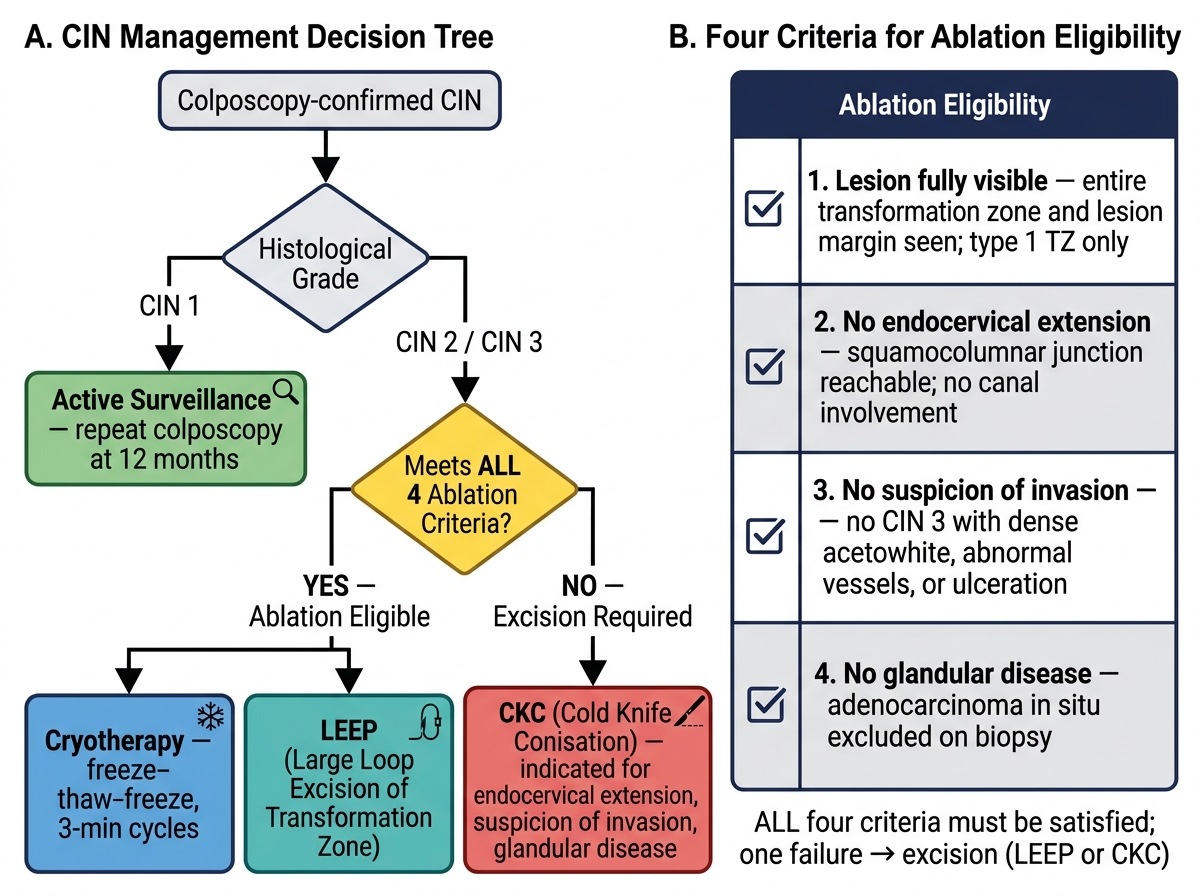
Decision Tree for Management of Cervical Intraepithelial Neoplasia (CIN)
SELF-CHECK
After cryotherapy for CIN 2, a patient contacts the clinic 10 days later with heavy vaginal bleeding. What is the most likely cause and what is the immediate management?
A. Primary haemorrhage from unrecognised invasion — arrange urgent CT staging
B. Secondary haemorrhage from eschar sloughing — inspect, apply silver nitrate or suture if needed
C. Normal post-cryotherapy discharge — reassure and discharge
D. Cervical stenosis — dilate with Hegar dilators
Reveal Answer
Answer: B. Secondary haemorrhage from eschar sloughing — inspect, apply silver nitrate or suture if needed
Secondary haemorrhage typically occurs 7–14 days post-cryotherapy or LEEP as the necrotic eschar separates. The immediate management is speculum examination to identify the bleeding point, with silver nitrate cautery, haemostatic agent, or a suture for persistent bleeding. Primary haemorrhage occurs during or immediately after the procedure. Cervical stenosis presents weeks to months later with dysmenorrhoea and reduced menstrual flow. A watery discharge for 2–4 weeks is normal — but heavy red bleeding at day 10 is secondary haemorrhage.
CLINICAL PEARL
Before any ablative treatment (cryotherapy or thermal ablation) for CIN or ectropion, always exclude active cervicitis by swab testing for chlamydia and gonorrhoea. Applying a cryoprobe to a cervix with active Chlamydia trachomatis infection disrupts the local mucosal barrier and can precipitate ascending infection and pelvic inflammatory disease (PID), potentially causing tubal damage and infertility. This screening step is non-negotiable in women of reproductive age before any cervical procedure. Similarly, never perform cryotherapy during menstruation or with suspected pregnancy — both are absolute contraindications.