Page 1 of 37
OG33.1-2 | Cervical Cancer — SDL Guide
Learning Objectives
- Classify cervical cancer by histological type and describe the role of HPV in its aetiology
- Apply FIGO 2018 staging criteria to assign the correct stage for a given clinical scenario
- Outline the investigations required to stage and evaluate a woman with suspected cervical cancer
- Describe the principles of surgical and radiation-based management according to stage
- Identify complications of treatment and outline a follow-up schedule
INSTRUCTIONS
Cervical cancer is the fourth most common cancer in women worldwide and the second most common in India, where it remains a leading cause of cancer-related death in women of reproductive age. This self-directed learning module equips you to recognise its clinical presentation, apply precise FIGO 2018 staging, and articulate evidence-based management principles — skills that are tested in final MBBS and are directly relevant to your work in gynaecology wards and outpatient clinics.
References
- DC Dutta's Textbook of Gynaecology, 8th edition, Chapter 33 (textbook)
- Shaw's Textbook of Gynaecology, 17th edition (textbook)
- FIGO 2018 Staging for Cancer of the Cervix Uteri, Int J Gynecol Obstet 2019;145:129-135 (guideline)
- Williams Gynecology, 4th edition (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 45-year-old woman presents to a rural primary health centre with a three-month history of foul-smelling vaginal discharge and postcoital bleeding. On speculum examination you find a 5 cm cauliflower-like growth on the ectocervix that bleeds on contact. Bimanual examination reveals the cervix is fixed, the right parametrium is indurated and extends to the pelvic side wall, and there is no lower vaginal involvement. She has no urinary symptoms. You refer her to the district hospital. What stage is this tumour? What further investigations does she need before treatment can begin? What is the primary modality of treatment? This SDL walks you through each of those decisions systematically, from the basic biology of the cancer to its FIGO 2018 classification and evidence-based management.
WHY THIS MATTERS
Cervical cancer is the second most frequent cancer in Indian women (after breast cancer), accounting for approximately 1.23 lakh new cases and 67,000 deaths annually. As a final-year student rotating through gynaecology, you will encounter women with abnormal vaginal bleeding in outpatient clinics; identifying those who require urgent colposcopy-directed biopsy versus those who can be managed conservatively is a core clinical skill. In final MBBS written papers and viva voce examinations, cervical cancer staging (especially the FIGO 2018 sub-divisions of Stage IB and the IIIC nodal additions) is one of the highest-yield factual questions. Understanding both surgical and radiation-based management options is essential for bedside teaching discussions.
RECALL
Before starting, recall the following from your earlier learning: (1) The transformation zone of the cervix — the junction between the stratified squamous epithelium of the ectocervix and the columnar epithelium of the endocervical canal — is the site where cervical intraepithelial neoplasia (CIN) develops and where the great majority of cervical cancers originate. (2) Human papillomavirus (HPV) is a DNA virus that infects squamous epithelial cells; serotypes 16 and 18 are classified as high-risk because their oncoproteins directly interfere with cell-cycle control proteins. (3) Lymphatic drainage of the cervix flows first to paracervical and parametrial nodes, then to obturator, internal and external iliac, and finally to common iliac and para-aortic nodes — a sequence that underpins the nodal sub-staging added in FIGO 2018. (4) The uterine blood supply (uterine artery and ureter relationship) is critical during surgery: the ureter runs approximately 1.5 cm lateral to the cervix before entering the trigone of the bladder, placing it at risk during radical hysterectomy.
Clinical Presentation: Symptoms and Signs of Cervical Cancer
The clinical presentation of cervical cancer varies considerably with the stage at which it is detected, and recognising the earliest symptoms is what distinguishes a doctor who intervenes early from one who misses the window of curative intent. In early-stage disease (Stage I–IIA), the most characteristic symptom is postcoital bleeding — fresh bleeding during or immediately after intercourse caused by the friable surface of the tumour or the exposed transformation zone. Equally characteristic is intermenstrual bleeding (irregular spotting between menstrual periods) and an increased volume of abnormal vaginal discharge, which is often watery, blood-stained, or frankly offensive in advanced lesions due to tumour necrosis and secondary infection. Women who are premenopausal may dismiss these symptoms as menstrual irregularity; postmenopausal women who experience any vaginal bleeding must be considered to have genital tract malignancy until proven otherwise.
As the tumour enlarges and invades adjacent structures, symptoms become more prominent. Pelvic or low-back pain suggests parametrial infiltration, ureteric obstruction, or involvement of pelvic side-wall structures including nerve roots. Urinary symptoms — frequency, dysuria, haematuria, or an inability to void — raise the suspicion of bladder involvement (Stage IVA). Rectal symptoms — rectal bleeding, altered bowel habit, or pain during defaecation — suggest rectal mucosal involvement or posterior parametrial spread. Lower-limb lymphoedema is a late sign of massive pelvic lymph node involvement or direct pelvic side-wall infiltration blocking lymphatic return.
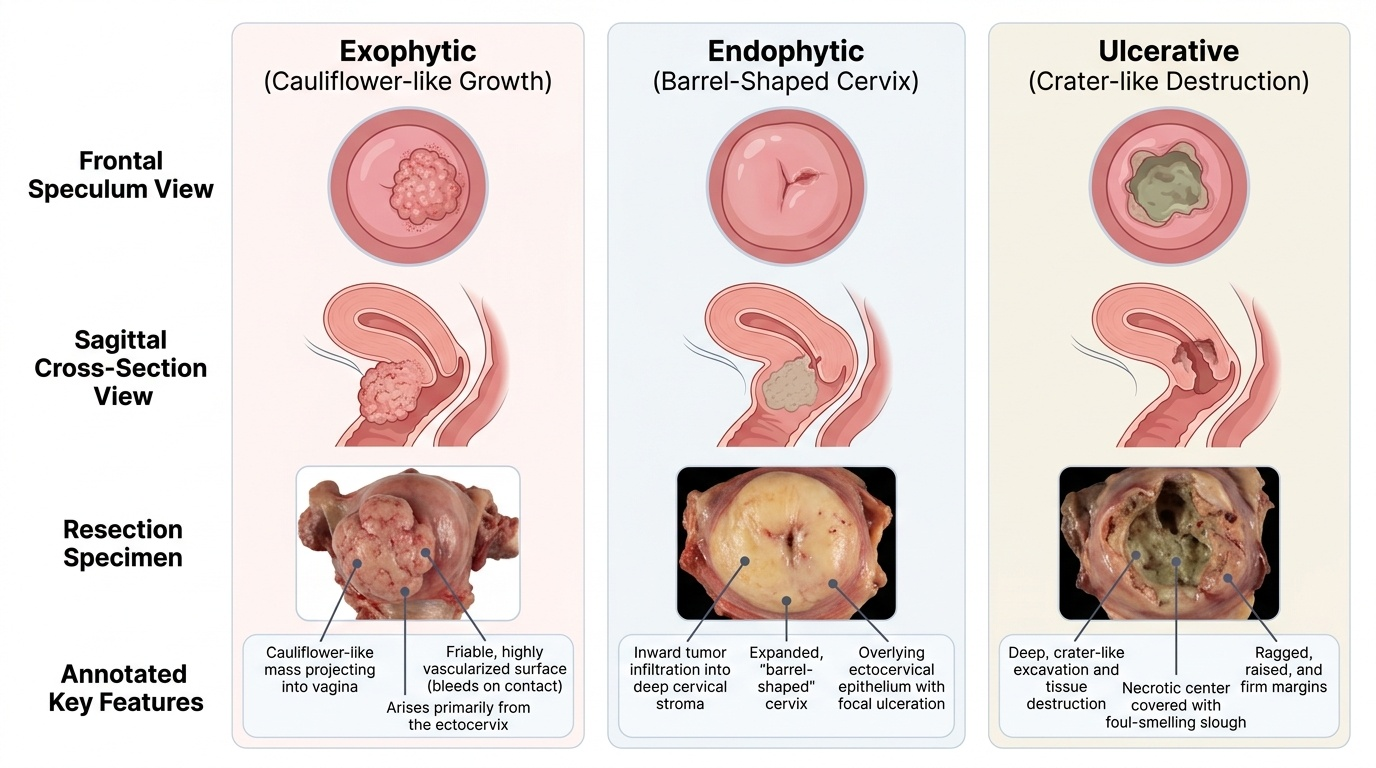
On speculum examination, early invasive cancers may appear merely as an area of acetowhite epithelium or a small irregular lesion at the transformation zone that bleeds readily on contact with the speculum. Larger tumours present as an exophytic mass (cauliflower-like proliferative growth, most common), an endophytic lesion (barrel-shaped, indurated cervix with an ulcerated crater, tumour growing inward), or an ulcerative type (necrotic cavity with foul odour). The cervix in advanced cases can be completely replaced by tumour. On bimanual examination, the clinician assesses parametrial induration (the 'cobblestone' feel of tumour spreading into the parametria) and whether it extends to the pelvic side wall — findings that drive the distinction between Stage IIB and Stage IIIB, which has major management implications.
Provided image
Aetiology and Pathophysiology: HPV, Risk Factors, and Carcinogenesis
Cervical cancer is unique among the common gynaecological malignancies in having a well-defined, sexually transmitted infectious cause: persistent infection with high-risk strains of human papillomavirus (HPV). HPV is a small, non-enveloped double-stranded DNA virus that infects basal epithelial cells, particularly at the transformation zone where metaplastic squamous epithelium is undergoing active cell division and is most vulnerable to viral integration. Of the more than 100 HPV genotypes identified, approximately 14 are classified as high-risk oncogenic types; HPV 16 and HPV 18 together account for approximately 70% of all cervical cancers globally, with HPV 16 predominating in squamous cell carcinoma and HPV 18 in adenocarcinoma.
The molecular mechanism of carcinogenesis centres on two viral oncoproteins. E6 oncoprotein binds and targets the tumour-suppressor protein p53 for ubiquitin-mediated proteasomal degradation, abolishing the p53-dependent apoptotic response to DNA damage — cells with damaged DNA that should be eliminated instead survive. E7 oncoprotein binds and inactivates the retinoblastoma protein (Rb), releasing the transcription factor E2F from Rb-mediated repression, thereby driving uncontrolled progression through the G1/S cell-cycle checkpoint. Together, E6 and E7 create a cell with defective DNA repair and unchecked proliferation, the preconditions for malignant transformation. In low-risk HPV types (e.g., HPV 6 and 11, which cause genital warts), E6 and E7 have much lower affinity for p53 and Rb, explaining why those types do not cause cancer.
Established risk factors for cervical cancer can be understood as factors that either increase the probability of HPV acquisition or favour progression from infection to invasive cancer. Early age at first sexual intercourse (before full squamous metaplasia of the transformation zone is complete, around age 20), multiple sexual partners (increasing HPV exposure), a partner with multiple partners, and a history of other sexually transmitted infections (particularly Herpes simplex virus type 2, Chlamydia) all increase acquisition risk. Immunosuppression — whether from HIV infection, organ transplantation, or prolonged corticosteroid use — impairs cell-mediated viral clearance and dramatically accelerates progression from CIN to invasive cancer; HIV-positive women have a 5-fold elevated risk. Cigarette smoking is an independent co-carcinogen: tobacco metabolites are detectable in cervical mucus, and smoking impairs local immune surveillance. Long-term (>5 years) use of combined oral contraceptives confers a modest increase in risk (approximately 1.5–2-fold), probably by altering the cervical microenvironment. High parity increases the time the transformation zone is everted and exposed, increasing vulnerability.
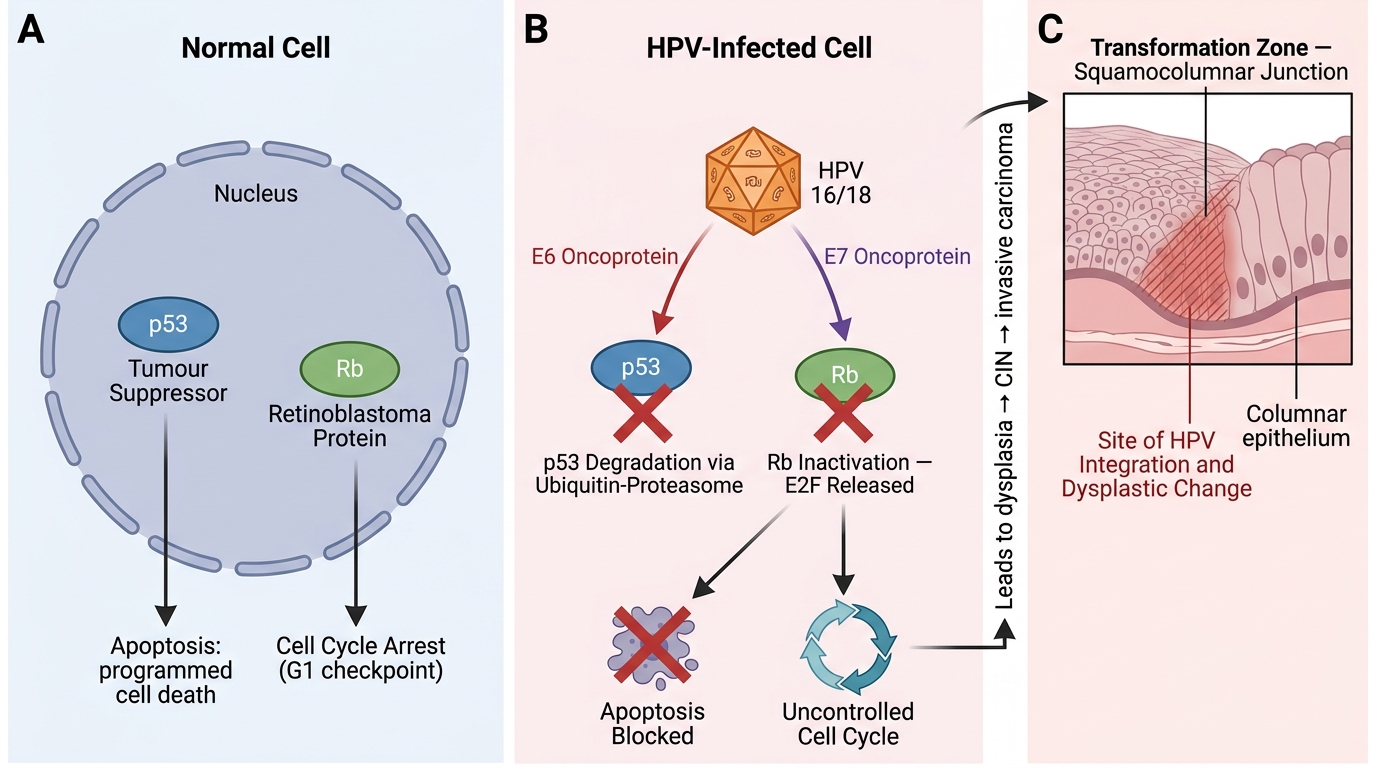
HPV E6/E7 Oncoprotein Mechanisms in Cervical Carcinogenesis
Pathology: Histological Types and Macroscopic Appearances
Understanding the histological landscape of cervical cancer is essential both for prognosis and for guiding management, as different subtypes have different natural histories, responses to chemotherapy, and associations with HPV. The vast majority of cervical cancers arise at the transformation zone, where squamous metaplasia creates a dynamic cellular interface susceptible to HPV-driven genetic instability.
Squamous cell carcinoma (SCC) accounts for approximately 70–80% of all cervical cancers and arises from the squamous epithelium of the ectocervix or metaplastic squamous cells of the transformation zone. Microscopically, well-differentiated SCCs show keratin pearl formation; moderately differentiated tumours show intercellular bridges; poorly differentiated tumours are large-cell, non-keratinising. Adenocarcinoma constitutes approximately 15–20% and arises from the mucin-secreting columnar (glandular) epithelium of the endocervical canal. Its incidence has increased over recent decades — likely related to the increasing prevalence of HPV 18 and to better screening detecting SCC at earlier (pre-invasive) stages, thereby unmasking a proportionally larger adenocarcinoma denominator. Adenocarcinoma is more difficult to detect on visual inspection and Pap smear (as the lesion is endocervical and may not exfoliate to the ectocervical surface), tends to cause more endophytic, barrel-shaped growth, and has a somewhat worse stage-for-stage prognosis. Adenosquamous carcinoma contains both malignant squamous and glandular components and accounts for about 3–5%. Rare histologies include small cell neuroendocrine carcinoma (highly aggressive, poor prognosis, association with HPV 18, often treated with cisplatin/etoposide chemotherapy similar to small cell lung cancer) and clear cell carcinoma (historically associated with diethylstilboestrol exposure, now mainly sporadic).
Macroscopically, the growth pattern — exophytic, endophytic (barrel), or ulcerative — influences how advanced the stage is perceived on clinical examination and how readily the tumour bleeds. Barrel-shaped endophytic cervical cancers are particularly important: the external os may appear nearly normal on speculum inspection, leading to underestimation of the extent of disease unless EUA (examination under anaesthesia) with biopsy is performed.

Provided image
SELF-CHECK
A biopsy of a cervical lesion shows malignant cells with intercellular bridges but no keratin pearls. Which histological type of cervical cancer does this represent?
A. Well-differentiated squamous cell carcinoma
B. Moderately differentiated squamous cell carcinoma
C. Adenocarcinoma
D. Small cell neuroendocrine carcinoma
Reveal Answer
Answer: B. Moderately differentiated squamous cell carcinoma
Moderately differentiated (Grade 2) squamous cell carcinoma shows intercellular bridges (prickle cells) but lacks keratin pearl formation (seen in well-differentiated Grade 1 tumours). Adenocarcinoma would show glandular structures. Small cell neuroendocrine carcinoma has a distinctive small blue cell appearance.