Page 2 of 37
OG33.1-2 | Cervical Cancer — SDL Guide (Part 2)
Diagnosis, Investigations, and Differential Diagnosis
The definitive diagnosis of cervical cancer always requires tissue histology — clinical or colposcopic appearances alone are insufficient. However, the diagnostic workup serves two distinct purposes: confirming the diagnosis and accurately staging the disease, because management is entirely stage-driven.
The diagnostic sequence begins with a careful clinical examination: inspection of the vulva and vagina for spread, speculum examination to assess the cervix (size, character, and extent of visible lesion), and bimanual pelvic examination to assess parametrial involvement, uterine mobility, and adnexal status. Rectal examination may be added to assess posterior parametrial and rectal involvement. Colposcopy allows magnified examination of the cervix after application of 3–5% acetic acid (acetowhitening identifies dysplastic/malignant areas) and Lugol's iodine (non-staining areas = iodine-negative = abnormal). Colposcopy-directed punch biopsy of the most suspicious area provides histological diagnosis. For endocervical lesions not visible on colposcopy, endocervical curettage (ECC) or cone biopsy is required. In cases where the lesion is visible and bleeds readily, a wedge biopsy or simple punch biopsy under direct vision is adequate.
For staging investigation, MRI of the pelvis is the most important single investigation — it delineates tumour size, depth of invasion, parametrial involvement, bladder/rectal involvement, and pelvic lymph node status with the highest soft-tissue contrast. CT of the chest, abdomen, and pelvis is used to assess para-aortic nodes and distant metastases. PET-CT (where available) provides superior sensitivity for detecting nodal and distant metastatic disease compared to CT alone and has been incorporated into FIGO 2018 staging — nodal involvement confirmed on either imaging (r-suffix) or pathology (p-suffix) now upgrades the stage to IIIC. Cystoscopy is performed when Stage IVA (bladder mucosal involvement) is suspected — bullous oedema alone is not sufficient for Stage IVA; actual biopsy-proven mucosal invasion is required. Proctoscopy/sigmoidoscopy is similarly performed when rectal mucosal involvement is suspected. Blood tests include full blood count (anaemia), renal function and urea (ureteric obstruction from parametrial disease can cause obstructive uropathy), and tumour marker SCC antigen (useful for monitoring treatment response in squamous cancers).
| Feature | Cervicitis | Cervical polyp | Cervical ectropion | Cervical cancer |
|---|---|---|---|---|
| Age | Reproductive | Reproductive | Reproductive/post-pill | ≥40 yr, peak 45-55 |
| Bleeding | Contact, irregular | Contact | Contact | Postcoital, intermenstrual |
| Discharge | Mucopurulent | Mucoid | Mucoid | Blood-stained, offensive |
| Examination | Red, inflamed os | Pedunculated mass | Eversion of endocervix, smooth | Hard, friable mass or ulcer |
| Biopsy | Inflammatory cells | Benign endometrial/endocervical | Benign columnar cells | Malignant cells |
| Management | Antibiotics | Polypectomy | Cryotherapy/observation | Stage-based oncology |
FIGO 2018 Staging of Cervical Cancer
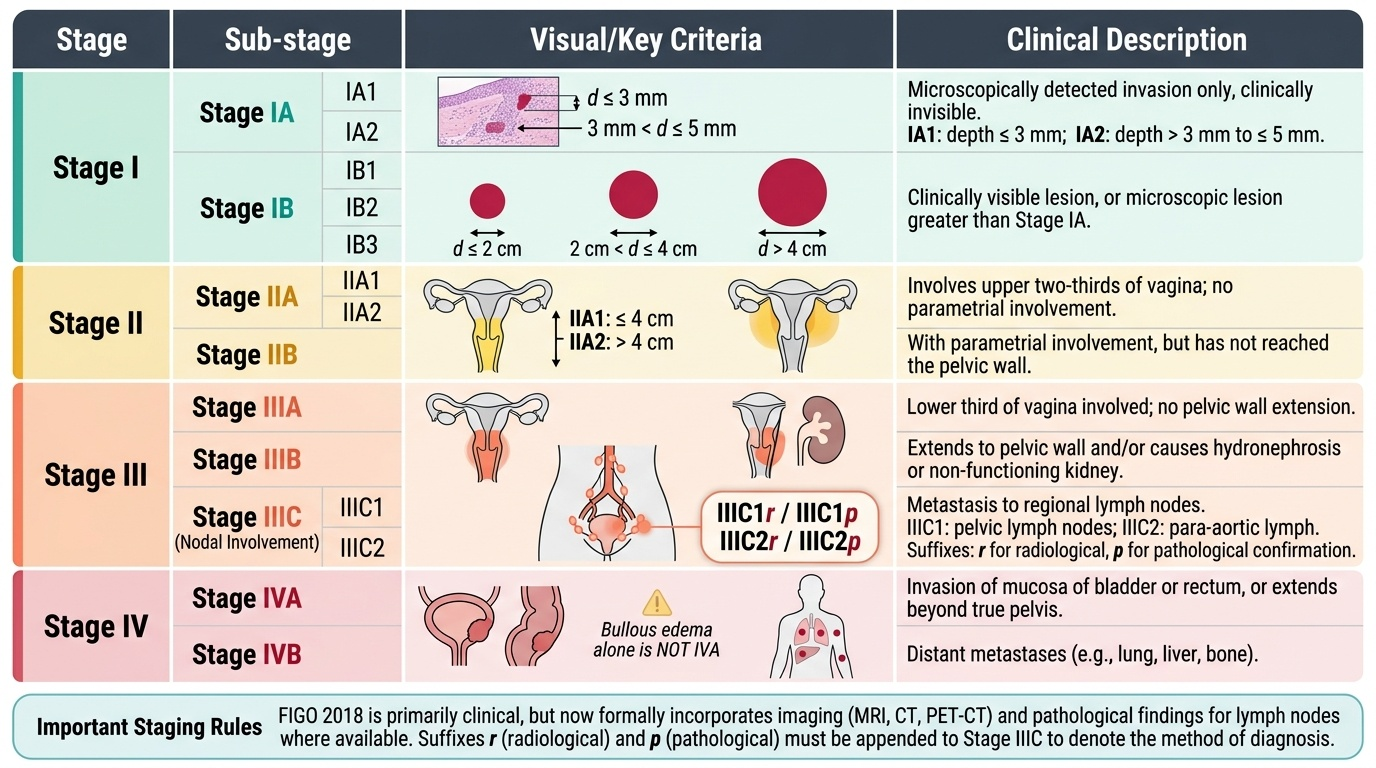
Accurate staging is the single most important clinical decision in managing cervical cancer, as it determines whether surgery, chemoradiation, or palliation is the appropriate treatment. The FIGO 2018 staging system (published in the International Journal of Gynecology and Obstetrics, 2019) superseded the previous 2009 FIGO system with two major innovations: first, the subdivision of Stage IB into three sub-stages based on tumour size; second, the addition of Stage IIIC to capture nodal involvement (pelvic and para-aortic) confirmed by either radiological (r suffix) or pathological (p suffix) means. These changes reflect evidence that lymph node status is among the most powerful prognostic factors and should influence treatment planning.
Provided image
The system is as follows. Stage I: tumour strictly confined to the cervix. IA = microscopically detected invasion only (clinically invisible); IA1 = stromal invasion depth ≤3 mm; IA2 = depth >3 mm and ≤5 mm (lateral extent no longer used). IB = clinically visible lesion, or microscopic lesion greater than Stage IA; IB1 = visible lesion ≤2 cm in greatest dimension; IB2 = lesion >2 cm and ≤4 cm; IB3 = lesion >4 cm. Stage II: tumour invades beyond the uterus but not to the lower third of the vagina or pelvic side wall. IIA = no parametrial involvement (IIA1 ≤4 cm, IIA2 >4 cm); IIB = with parametrial involvement, not reaching pelvic wall. Stage III: tumour extends to pelvic wall, or involves lower third of vagina, or causes hydronephrosis/non-functioning kidney, or involves pelvic/para-aortic lymph nodes. IIIA = lower-third vaginal involvement, no pelvic wall extension; IIIB = pelvic wall involvement and/or hydronephrosis/non-functioning kidney; IIIC1 = pelvic lymph node metastasis (add 'r' for radiological or 'p' for pathological — e.g., IIIC1r = radiologically confirmed pelvic nodes); IIIC2 = para-aortic lymph node metastasis. Stage IV: tumour invades mucosa of bladder or rectum, or extends beyond true pelvis. IVA = spread to adjacent organs (bladder or rectal mucosa — bullous oedema alone is NOT IVA); IVB = distant metastases (lung, liver, bone).
Important staging rules: (1) FIGO 2018 is primarily a clinical staging system (accessible to settings without advanced imaging), but now formally incorporates imaging and pathological nodal data where available — a major departure from the purely clinical 2009 system. (2) If there is doubt about which stage to assign, the lower (earlier) stage is chosen (to avoid overstaging). (3) The stage is assigned at the time of first treatment and does not change even if the tumour recurs.
SELF-CHECK
A woman has a 3.5 cm cervical tumour visible on speculum examination. MRI shows left parametrial involvement extending to within 5 mm of the pelvic side wall but not reaching it. There is no hydronephrosis and no lymph node involvement on imaging. What is the correct FIGO 2018 stage?
A. IB2
B. IIB
C. IIIB
D. IIIC1r
Reveal Answer
Answer: B. IIB
Parametrial involvement (without reaching the pelvic side wall) places this tumour in Stage II. The absence of vaginal involvement and the tumour being >2 cm (IIA1 cut-off) with parametrial disease defines Stage IIB. IIIB requires extension to the pelvic side wall or hydronephrosis. There are no lymph nodes involved, so IIIC does not apply.
Principles of Management: Surgery and Radiotherapy by Stage
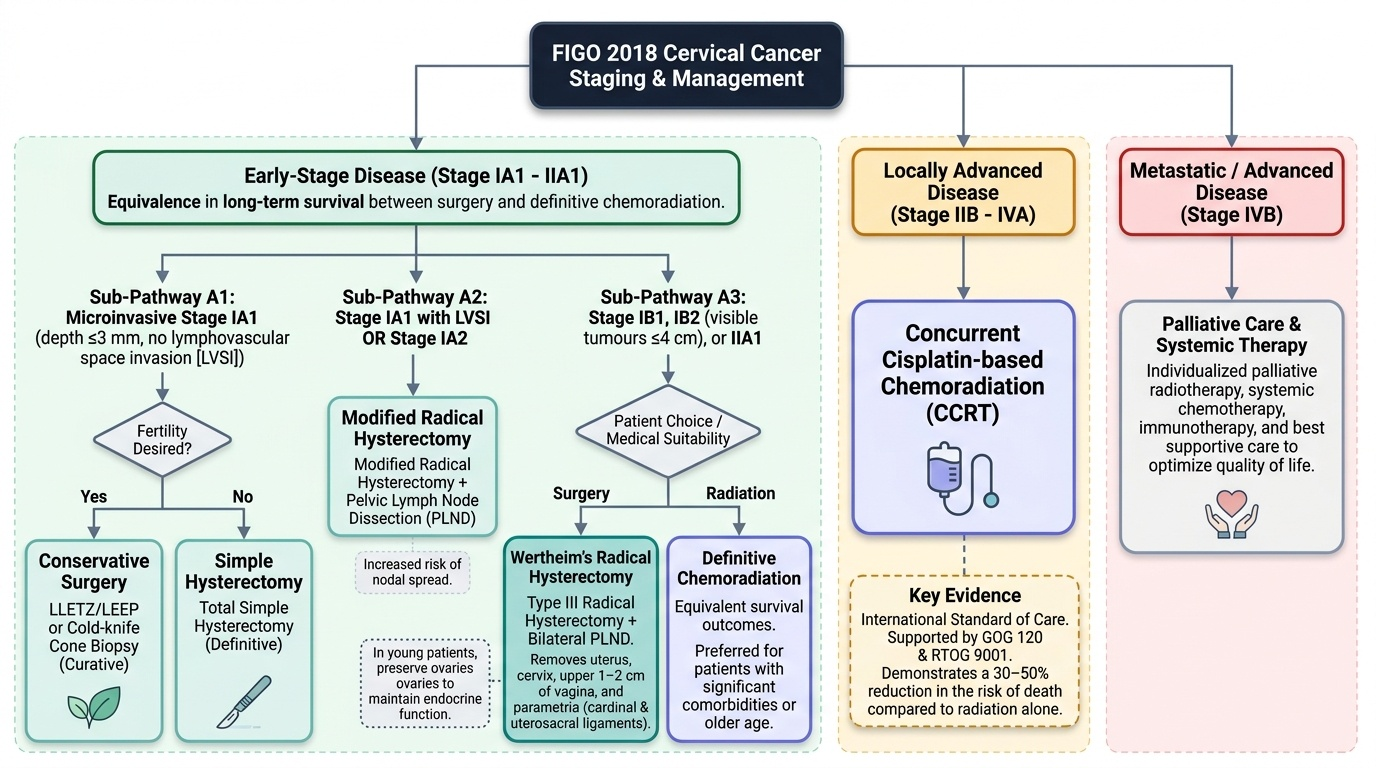
Management of cervical cancer is stage-directed and requires a multidisciplinary approach involving the gynaecological oncologist, radiation oncologist, and medical oncologist. The fundamental principle is that for early-stage disease (IA–IIA1), radical surgery and definitive chemoradiation achieve equivalent long-term survival — the choice between them depends on patient age, comorbidities, fertility desire, and institutional expertise. For locally advanced disease (IIB–IVA), concurrent cisplatin-based chemoradiation is the internationally recognised standard of care, following landmark randomised controlled trials (including GOG 120 and RTOG 9001) that demonstrated a survival benefit of approximately 30–50% reduction in the risk of death compared to radiation alone.
For microinvasive Stage IA1 (depth ≤3 mm, no lymphovascular space invasion): if fertility is to be preserved, large loop excision of the transformation zone (LLETZ/LEEP) or cold-knife cone biopsy is curative; if fertility is not desired, simple (total) hysterectomy is definitive. If lymphovascular space invasion is present in IA1, or in all IA2 tumours, the risk of nodal spread rises and the procedure is upgraded to modified radical hysterectomy with pelvic lymph node dissection.
For Stage IB1 and IB2 (visible tumours ≤4 cm): Wertheim's (Type III radical) hysterectomy with bilateral pelvic lymph node dissection is the surgical standard. The radical hysterectomy removes the uterus, cervix, upper 1–2 cm of vagina, and the parametria including cardinal and uterosacral ligaments. In young women who wish to preserve ovarian function, the ovaries may be conserved (as cervical cancer is not oestrogen-sensitive and ovarian metastasis is rare in SCC). Definitive chemoradiation (external beam radiation to the pelvis followed by intracavitary brachytherapy, concurrent with weekly cisplatin 40 mg/m²) is equally effective for IB1 and IB2 and is the preferred treatment in women who are poor surgical candidates. Adjuvant chemoradiation is given after surgery if high-risk pathological features are found (positive surgical margins, parametrial involvement, involved lymph nodes — the Sedlis criteria for intermediate risk).
For Stage IB3 and IIA2 (tumours >4 cm): Primary surgery has a higher risk of requiring adjuvant radiation anyway; therefore concurrent chemoradiation is typically preferred, with external beam pelvic radiation (45–50 Gy in 25–28 fractions) concurrent with weekly cisplatin, followed by brachytherapy boost to the cervix (total point-A dose 85–90 Gy equivalent).
For Stage IIB to IVA (parametrial, pelvic side wall, bladder/rectal involvement): Concurrent cisplatin-based chemoradiation is the definitive treatment. Surgery is not curative at this stage. Extended-field radiation is added when para-aortic nodes are involved (IIIC2).
For Stage IVB (distant metastases): treatment is palliative, with systemic chemotherapy (cisplatin + paclitaxel, with or without bevacizumab per GOG 240 trial data showing improved overall survival). Radiation may be used palliatively to control haemorrhage or pelvic pain.
Provided image