Page 3 of 37
OG33.1-2 | Cervical Cancer — SDL Guide (Part 3)
Prognosis, Follow-up, and Complications of Treatment
Prognosis in cervical cancer is primarily determined by FIGO stage at diagnosis, with 5-year survival rates declining steeply from early to advanced stages: Stage IA — approximately 95–98%; Stage IB — 80–90%; Stage IIA — 70–75%; Stage IIB — 65–70%; Stage IIIA/IIIB — 40–50%; Stage IVA — 20–25%; Stage IVB — <15%. Lymph node involvement is the single most powerful independent prognostic factor after stage — women with positive pelvic nodes have a 5-year survival approximately 40–50% lower than node-negative patients at the same clinical stage. Other adverse prognostic factors include large tumour volume, poorly differentiated histology, and lymphovascular space invasion.
Post-treatment surveillance follows a structured schedule to detect recurrence early — approximately 70% of recurrences occur within the first two years. The standard follow-up is: 3-monthly visits for the first 2 years (clinical examination, vault smear), then 6-monthly visits for years 3–5, and annually thereafter. At each visit, the clinician examines the vaginal vault for local recurrence, the inguinal and supraclavicular nodes for distant nodal disease, and evaluates any new symptoms. Imaging (CT or PET-CT) is reserved for symptomatic women or those with rising SCC antigen.
Complications of Wertheim's radical hysterectomy include: (a) ureteric injury or uretero-vaginal fistula — the ureter's proximity to the cardinal ligament makes it vulnerable; (b) bladder dysfunction (neurogenic atony, from sacrifice of parasympathetic pelvic plexus) requiring prolonged catheterisation; (c) lymphocyst formation and lymphoedema from pelvic lymphadenectomy; (d) vault haematoma; (e) early ovarian failure if ovaries removed in premenopausal women. Complications of chemoradiation include early effects (radiation cystitis, proctitis, diarrhoea, myelosuppression from cisplatin, nausea) and late effects (radiation fibrosis of the small bowel causing obstruction/malabsorption, vesico-vaginal or recto-vaginal fistulae, vaginal stenosis, ureteric stricture, secondary malignancies). The risk of radiation fistulae is higher when surgery precedes radiation (combined modality treatment), which is why primary chemoradiation is preferred over surgery-then-radiation in locally advanced disease.
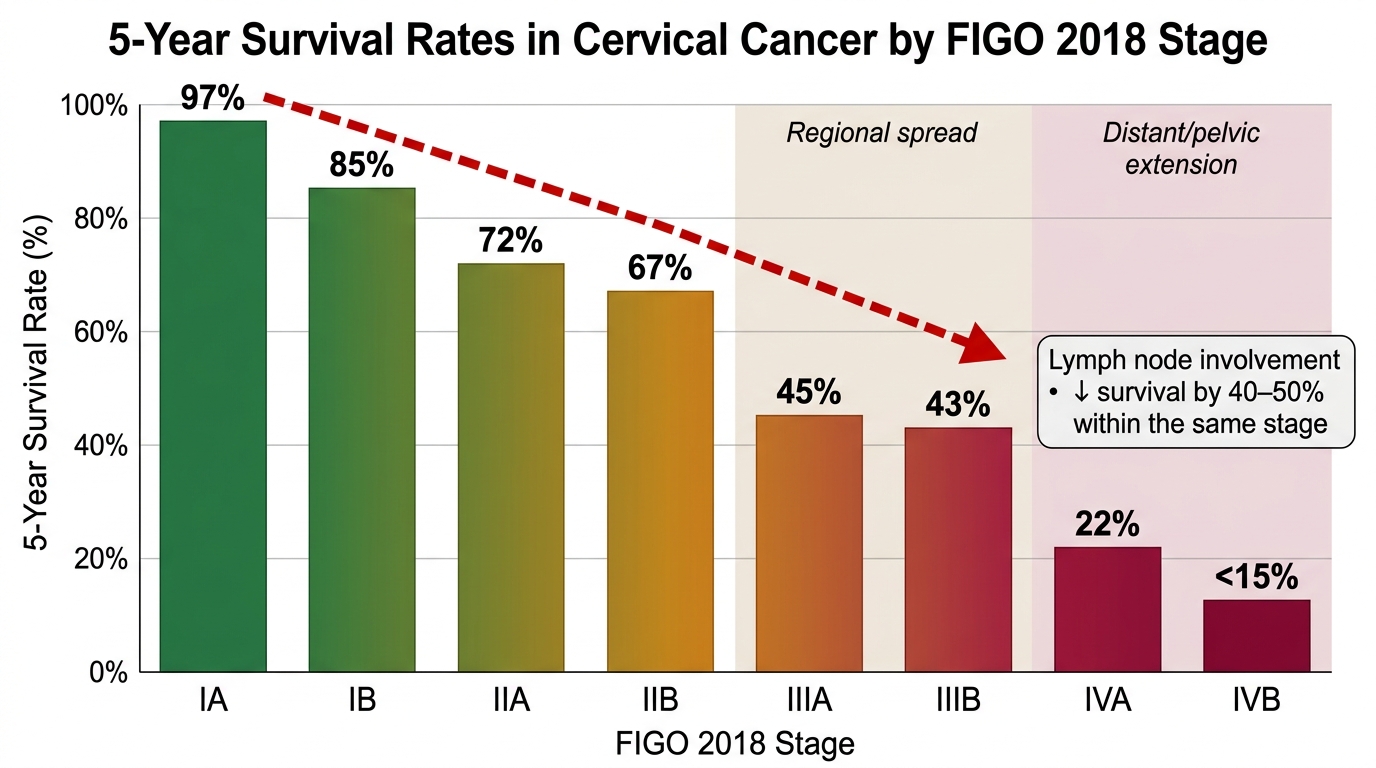
5-Year Survival Rates by FIGO 2018 Stage in Cervical Cancer
SELF-CHECK
During a Wertheim's radical hysterectomy, the surgeon transects the cardinal ligaments close to the pelvic side wall. Which structure is at greatest risk of inadvertent injury during this step?
A. Internal iliac artery
B. Ureter
C. Obturator nerve
D. Sigmoid colon
Reveal Answer
Answer: B. Ureter
The ureter runs approximately 1.5 cm lateral to the cervix and passes under the uterine artery ('water flows under the bridge') before entering the bladder trigone. When the cardinal ligaments are transected during radical hysterectomy, the ureter — which runs within or close to the cardinal ligament — is the structure most at risk. Ureteric injury (ligation, kinking, or transection) is the most surgically significant complication of radical hysterectomy.
Self-Assessment and Case Integration
This section consolidates the key factual and clinical reasoning skills from the module. Before attempting the self-check questions below, review the FIGO 2018 staging table and the stage-directed management algorithm. Common examination pitfalls include: (a) confusing Stage IIB (parametrial involvement not reaching pelvic wall) with Stage IIIB (pelvic wall involvement); (b) forgetting the IIIC sub-stages and the r/p notation; (c) describing the wrong histological type as most common; (d) misidentifying the correct management for Stage IB2 (chemoradiation or radical hysterectomy — both are acceptable, but primary surgery with expected adjuvant radiation is avoided in many centres); (e) confusing complications of surgery versus radiation. Practise by assigning stages to clinical vignettes before looking up the answer — the staging exercise is exactly how examination questions are constructed.
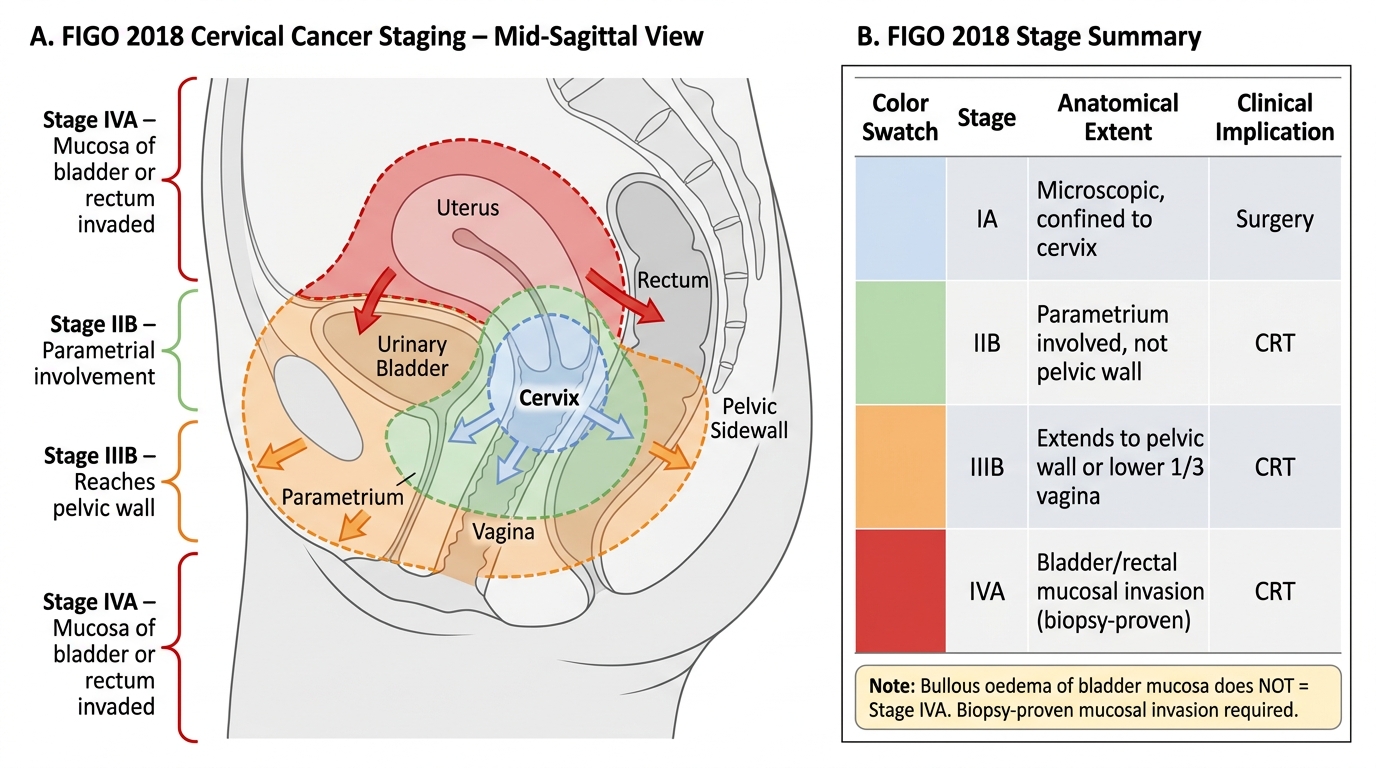
Cervical Cancer FIGO 2018 Staging — Extent of Spread
SELF-CHECK
A 52-year-old woman has FIGO 2018 Stage IVA cervical cancer. What is the PRIMARY modality of treatment?
A. Wertheim's radical hysterectomy
B. Pelvic exenteration
C. Concurrent cisplatin-based chemoradiation
D. Cisplatin + paclitaxel systemic chemotherapy alone
Reveal Answer
Answer: C. Concurrent cisplatin-based chemoradiation
Stage IVA indicates spread to the mucosa of the bladder or rectum, but the tumour is still within the true pelvis and there are no distant metastases. Concurrent chemoradiation (external beam radiation + cisplatin + brachytherapy boost) is the standard of care for Stages IIB through IVA. Surgery is not curative at this stage. Pelvic exenteration is a salvage procedure for isolated central recurrence after radiation. Systemic chemotherapy alone is palliative and reserved for IVB.
CLINICAL PEARL
A critical distinction that often causes errors in staging: bullous oedema of the bladder mucosa on cystoscopy does NOT define Stage IVA. Only biopsy-proven invasion of the bladder mucosa (or rectal mucosa) upgrades the stage to IVA. Oedema is a reactive finding secondary to radiation or parametrial compression of lymphatics; the tumour has not actually penetrated the bladder wall. Always request a biopsy of any cystoscopic abnormality before upstaging to IVA, as this decision converts potentially curative chemoradiation to palliative management.