Page 5 of 37
OG33.3-4 | Cervical Cancer Screening and Prevention — SDL Guide
Learning Objectives
- Describe the rationale and evidence base for cervical cancer screening in India
- Explain the natural history of HPV infection and CIN as the target of screening
- Demonstrate the technique of VIA and Pap smear in a simulated environment
- Enumerate screening modalities — VIA, VILI, Pap smear, HPV DNA testing — with their sensitivity, specificity, and practical requirements
- Describe HPV vaccination schedules, target populations, and available vaccines in India
- Interpret an abnormal VIA or Pap smear result and outline the appropriate management pathway
INSTRUCTIONS
Cervical cancer is one of the most preventable cancers: a well-organised screening programme can detect and treat pre-invasive disease before it becomes invasive. India bears nearly one-quarter of the global burden of cervical cancer deaths, and the majority of these deaths occur in women who have never been screened. This module teaches you the practical skills of cervical cancer screening — how to perform VIA and Pap smear, how to interpret results, and how to counsel women about vaccination — so that you can contribute meaningfully to reducing this burden from your first day in clinical practice.
References
- DC Dutta's Textbook of Gynaecology, 8th edition, Chapter 33 (textbook)
- NHM India — Operational Guidelines for Cervical Cancer Screening, 2016 (guideline)
- WHO Guidelines for Screening and Treatment of Cervical Pre-cancer Lesions for Cervical Cancer Prevention, 2nd edition, 2021 (guideline)
- Shaw's Textbook of Gynaecology, 17th edition (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
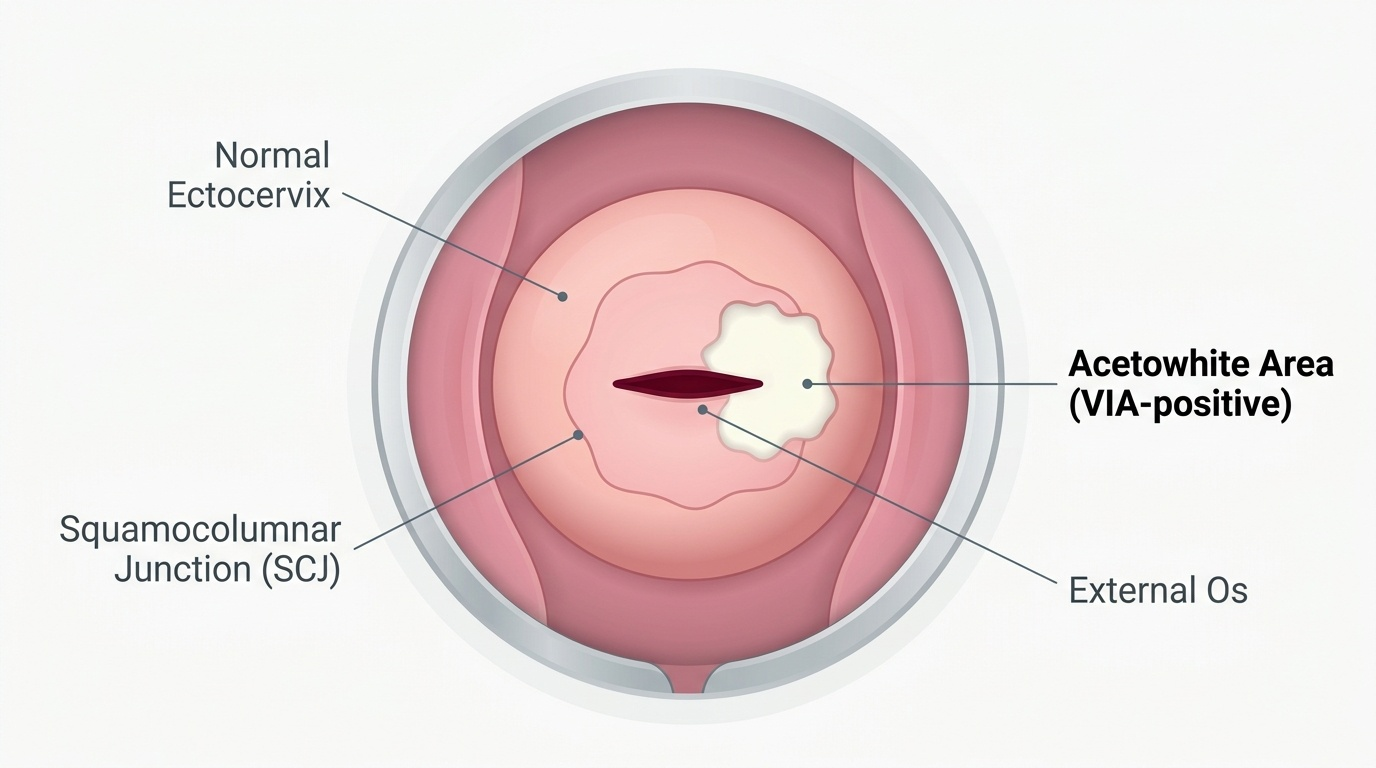
During a community outreach camp in a rural district, a 38-year-old multipara woman comes forward after a health worker explains cervical cancer screening. She has never had a Pap smear and is unaware that HPV vaccination exists. You perform VIA, applying 3–5% acetic acid to the cervix. After one minute, you observe a sharply demarcated acetowhite area just inside the external os at the transformation zone. She asks: 'Does this mean I have cancer?' What do you tell her? What is the next step — treat her today or refer her for colposcopy? Could her adolescent daughter have been protected from this disease entirely? This module equips you to answer each of those questions with confidence.
WHY THIS MATTERS
India accounts for approximately 18–20% of global cervical cancer deaths despite having only about 17% of the world's women, meaning Indian women face a disproportionately high risk. Nearly 80% of cervical cancer cases in India are diagnosed at advanced stages (Stage III–IV), when treatment is far less effective — the direct consequence of absent or inadequate screening. The WHO global strategy to eliminate cervical cancer as a public health problem sets a 90-70-90 target: 90% of girls fully vaccinated by age 15, 70% of women screened with a high-performance test by age 35 and again by age 45, and 90% of women with identified disease receiving treatment. As a future clinician, you will be at the front line of all three pillars — vaccinating girls, screening women, and referring those with abnormal results for treatment.
RECALL
Recall the following from earlier learning: (1) The transformation zone of the cervix is where squamocolumnar metaplasia occurs and where HPV-driven carcinogenesis begins — screening targets this zone because pre-invasive changes (CIN) are detectable there before invasion occurs. (2) CIN (cervical intraepithelial neoplasia) is graded 1 through 3; CIN 1 is low-grade and often regresses spontaneously, while CIN 2 and CIN 3 (HSIL) are high-grade precancerous lesions that require treatment. (3) Most HPV infections in immunocompetent women clear within 1–2 years; only persistent high-risk HPV infection (types 16, 18, and others) leads to CIN and invasive cancer — this natural history creates the window for effective secondary prevention. (4) Acetic acid applied to the cervix causes reversible coagulation of nuclear proteins in abnormal (dysplastic) cells with high nuclear-to-cytoplasmic ratios, producing temporary whitening (acetowhitening) — the basis of VIA.
Clinical Indication: Why Cervical Cancer Screening Matters
Cervical cancer is one of the few malignancies that can be prevented at both primary and secondary levels, making screening a uniquely powerful public health intervention. The biological rationale for screening rests on the well-characterised natural history of HPV-driven cervical carcinogenesis: HPV infection of the transformation zone → CIN 1 (low-grade) → CIN 2/3 (high-grade) → microinvasive cancer → invasive cancer. This progression typically spans 10–15 years, providing a substantial window in which pre-invasive disease can be detected and treated before invasion occurs. When detected at the CIN 2/3 stage and treated with cryotherapy or LEEP, women are cured with minimal morbidity, avoiding the far greater burden of treating invasive cervical cancer.
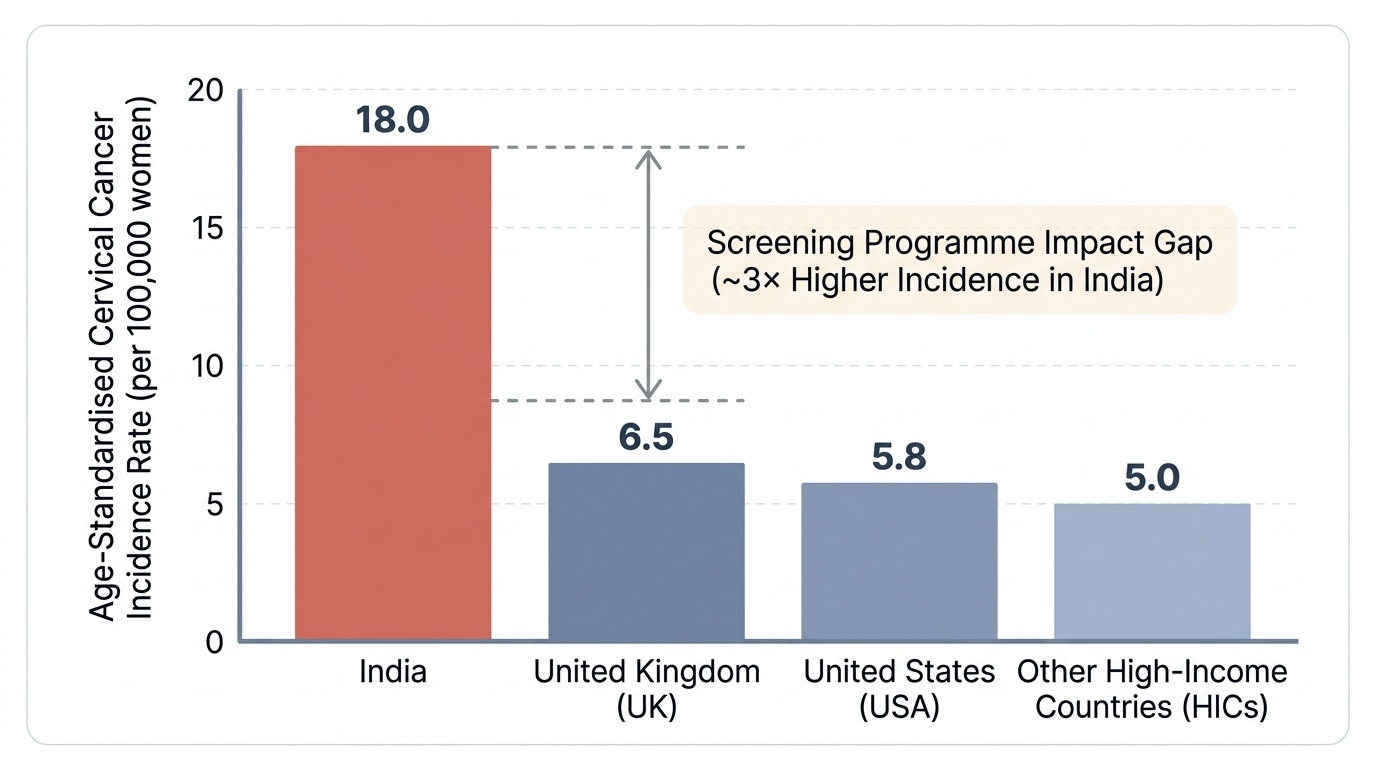
In India, the epidemiological burden is stark. Approximately 1.23 lakh (123,000) new cases of cervical cancer are diagnosed annually, with an age-standardised incidence rate of approximately 18 per 100,000 women — far higher than the rates in countries with established screening programmes (e.g., ~6.5 in the UK, ~5.8 in the USA). Mortality is approximately 67,000 deaths per year. The critical driver of this gap is not biology but health system access: Indian women at highest risk — rural, low-income, multiparous, limited healthcare contact — are precisely those least likely to have been screened. The National Health Mission (NHM) of India has embedded cervical cancer screening as a component of the Comprehensive Primary Health Care package at the health and wellness centre level, aiming to screen all women aged 30–65 years at least once every five years.
The WHO global elimination strategy (2020) provides the strategic framework. It sets three targets to be achieved by 2030: 90% of girls fully vaccinated with HPV vaccine by age 15 (primary prevention); 70% of women screened with a high-performance test by age 35 and again by age 45 (secondary prevention); and 90% of women with cervical disease receiving treatment (tertiary). These 90-70-90 targets operationalise a vision of cervical cancer as an eliminable disease within a generation — achievable only if every healthcare provider participates.
Provided image
Anatomy and Governing Principles of Screening
The transformation zone (TZ) is the anatomical target of all cervical screening methods because it is the site where cervical carcinogenesis invariably begins. Understanding its location and behaviour explains both how screening works and why certain tests are more effective than others. The TZ is the region between the original squamocolumnar junction (SCJ) — the historical boundary between the squamous ectocervix and the columnar endocervix established in foetal life — and the current SCJ, which migrates with age, hormonal status, and parity. Squamous metaplasia (replacement of columnar by squamous epithelium, mediated by subcolumnar reserve cells) is a normal, ongoing process within this zone; it is during active metaplasia that HPV integration and CIN develop most readily.
In adolescents and women of reproductive age, the TZ is typically everted onto the ectocervix, making it fully visible on speculum examination — ideal for VIA and Pap smear. After the menopause, oestrogen withdrawal causes the cervix to involute and the SCJ to recede into the endocervical canal, making the TZ less accessible and reducing the reliability of visual methods in older women. This explains why satisfactory colposcopy (visualisation of the entire TZ and SCJ) is possible in most premenopausal but not always in postmenopausal women, and why endocervical sampling (ECC) is needed when the SCJ is not visible.
The principles of a good screening test apply directly to cervical cancer methods. Sensitivity (the ability to detect true pre-cancerous disease — CIN 2+) must be high enough to reduce cancer incidence; specificity (avoiding over-referral of normal women) must be high enough to keep the programme cost-effective and to avoid unnecessary treatment anxiety and complications. No current single test achieves perfect sensitivity and specificity simultaneously: VIA is high-sensitivity but low-specificity in practice; cytology (Pap smear) is relatively specific but has only moderate sensitivity for a single test (~55% sensitivity for CIN 2+); HPV DNA testing has the highest sensitivity (~95%) but requires laboratory infrastructure. The choice of screening method in any given setting reflects the balance between accuracy, feasibility, and resources available.
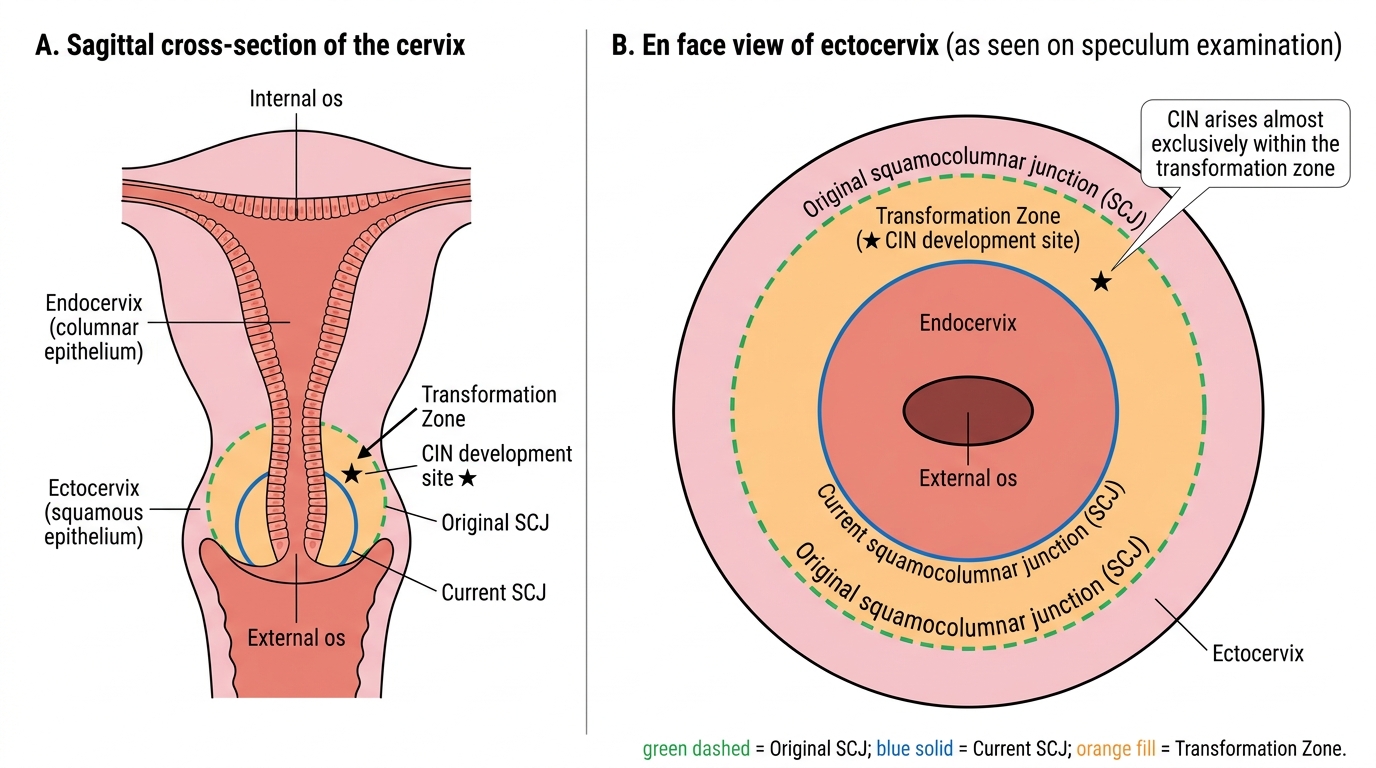
Cervical Transformation Zone: Anatomical Cross-Section and Colposcopic View
Screening Methods: VIA, VILI, Pap Smear, and HPV DNA Testing
Four screening methods are used in India, each with distinct technical requirements, performance characteristics, and applications. Understanding how to perform them correctly and how to interpret results is the core practical skill of this SDL.
Visual Inspection with Acetic Acid (VIA) is the method of choice for low-resource settings because it requires no laboratory, no electricity, and minimal equipment. The technique is: (a) Insert a bivalve speculum under good light (torch or LED headlamp). (b) Visualise the entire cervix and transformation zone. (c) Apply 3–5% acetic acid (not glacial — this causes burns) liberally to the cervix using a swab or spray. (d) Wait exactly 1 minute and re-inspect. A VIA-positive result is a sharply demarcated dense acetowhite area within or touching the transformation zone (TZ) or external os, that persists at 1 minute. Acetowhitening that is faint, irregular, or outside the TZ may be normal metaplasia or cervicitis (a common cause of false positives). A VIA-negative result is a cervix with no acetowhite area in the TZ. Polyps, nabothian follicles, and inflammatory changes may mimic VIA positivity — experience reduces false-positive rates. Sensitivity of VIA for CIN 2+ is approximately 60–80%; specificity approximately 70–85%.
Visual Inspection with Lugol's Iodine (VILI) applies Lugol's iodine (Schiller's test) to the cervix after VIA. Normal squamous epithelium stains mahogany-brown (rich in glycogen); columnar epithelium and abnormal squamous cells (low glycogen) do not take up iodine. A VILI-positive result is a mustard-yellow or saffron-yellow non-staining area in the TZ. VILI is often used in combination with VIA to increase sensitivity; it is most useful in postmenopausal women where VIA acetowhitening may be less clear.
Pap smear (conventional cytology) samples exfoliated cells from the TZ using an Ayre's spatula (ectocervix) and an endocervical brush or cytobrush (endocervix); cells are spread on a glass slide and fixed immediately with 95% alcohol or fixative spray. The sample is stained by the Papanicolaou method and reported by a cytologist using the Bethesda 2014 system: NILM (negative for intraepithelial lesion or malignancy), ASCUS (atypical squamous cells of undetermined significance), LSIL (low-grade squamous intraepithelial lesion = HPV/CIN 1 changes), HSIL (high-grade squamous intraepithelial lesion = CIN 2/3), ASC-H (atypical squamous cells — cannot exclude HSIL), AGC (atypical glandular cells), and carcinoma. Sensitivity of a single Pap smear for CIN 2+ is approximately 55%; specificity is approximately 97%. Repeated 3-yearly smears improve cumulative sensitivity. Liquid-based cytology (LBC) is an improved variant where cells are rinsed into a preservative vial rather than smeared — reduces obscuring blood/inflammation and allows the same sample to be tested for HPV DNA.
HPV DNA testing detects the presence of high-risk HPV genotypes (16, 18, and 12 others) in cervical cells, using PCR or hybrid capture on a cervical swab. It is now recognised by WHO and NHM India as the preferred primary screening test because of its superior sensitivity (~95% for CIN 2+), long-lasting negative predictive value (a negative HPV test at age 35 confers protection for 5 years), and the ability in some formulations (co-testing) to provide risk stratification by genotype (HPV 16/18 vs other high-risk types). Women with a positive HPV test are then triaged with cytology or referred for colposcopy. The limitation in India is laboratory infrastructure requirement and cost.
Provided image
| Method | Sensitivity CIN2+ | Specificity | Infrastructure | NHM India status |
|---|---|---|---|---|
| VIA | 60–80% | 70–85% | Minimal (torch, acetic acid) | Recommended for PHC |
| VILI | 70–85% | 75–85% | Minimal (Lugol's iodine) | Adjunct to VIA |
| Pap smear | 55% (single) | ~97% | Cytology lab, pathologist | Urban facilities |
| HPV DNA | ~95% | ~90% | PCR/hybrid capture lab | Recommended (primary) |