Page 6 of 37
OG33.3-4 | Cervical Cancer Screening and Prevention — SDL Guide (Part 2)
HPV Vaccination: Schedules, Vaccines Available, and Target Populations
HPV vaccination is the most potent primary prevention strategy against cervical cancer, with vaccine efficacy exceeding 95% for HPV type-specific CIN 2/3 in girls vaccinated before sexual debut. Understanding the available vaccines, their schedules, and target groups is an essential clinical skill because you will counsel parents, adolescent girls, and health workers about the national vaccination programme.
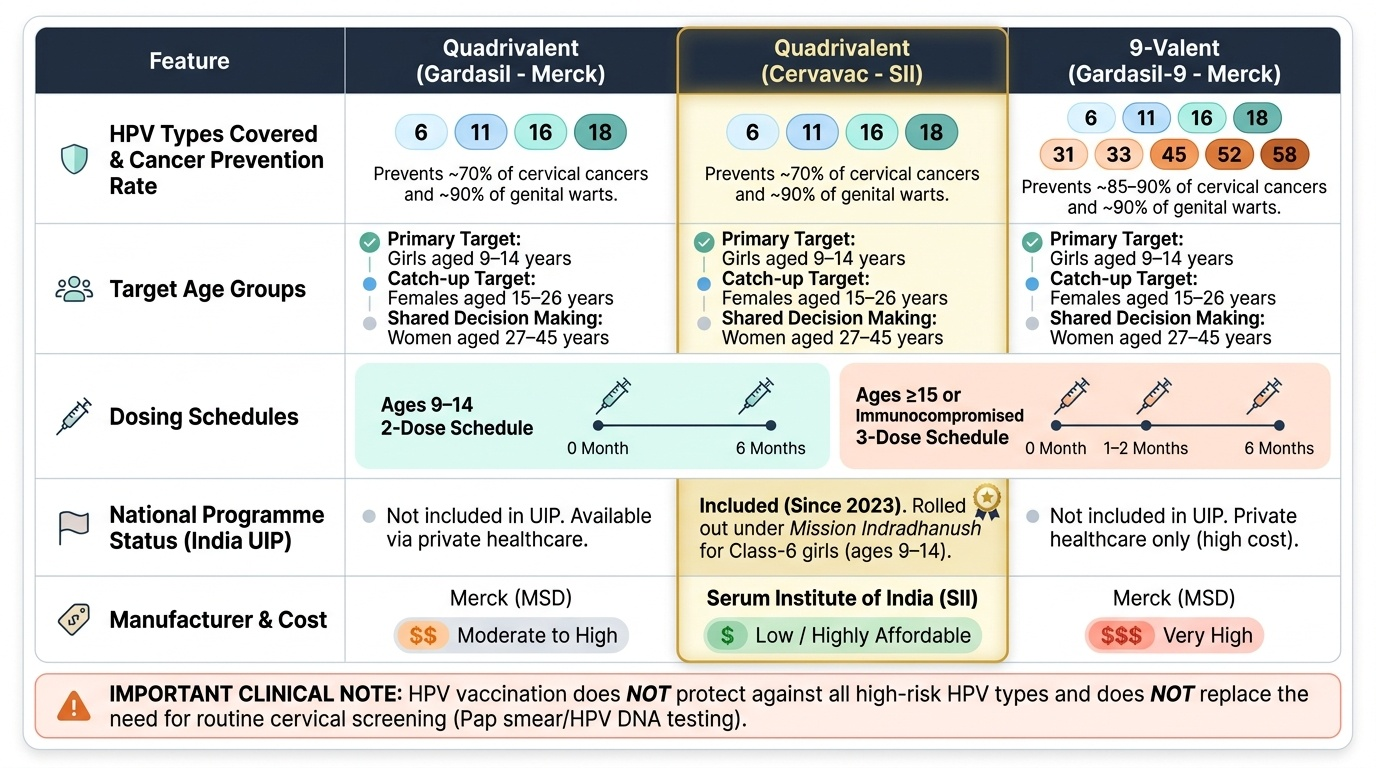
Two HPV vaccines are most widely used globally. The quadrivalent HPV vaccine (Gardasil, Merck) protects against HPV types 6, 11, 16, and 18 — types 16 and 18 together cause approximately 70% of cervical cancers, and types 6 and 11 cause approximately 90% of genital warts. The 9-valent HPV vaccine (Gardasil-9, Merck) extends protection to also cover HPV types 31, 33, 45, 52, and 58, raising cancer prevention coverage to approximately 85–90% of cervical cancers. India's indigenous vaccine Cervavac (Serum Institute of India) is a quadrivalent vaccine approved by DCGI in 2022, designed for the national immunisation programme at lower cost. A bivalent vaccine (Cervarix, GSK) covering only HPV 16/18 is also available.
Vaccination schedules follow age-based immunogenicity data. In girls aged 9–14 years, a two-dose schedule (doses at 0 and 6 months) is sufficient because immune responses in pre-adolescents are substantially more robust than in adults, generating antibody titres at least as high as the three-dose response in older women. In females aged ≥15 years, or in any individual who is immunocompromised (HIV-positive, transplant recipient, on immunosuppressive therapy), a three-dose schedule (0, 1–2 months, 6 months) is required because immune response is less predictable. The India Universal Immunisation Programme (UIP) launched HPV vaccination for class-6 girls (approximately age 9–14) under Mission Indradhanush from 2023, using Cervavac.
Vaccination is most effective before first sexual exposure to HPV, which is why the primary target is girls aged 9–14 years. However, catch-up vaccination may benefit unvaccinated or incompletely vaccinated females up to age 26, and shared decision-making is recommended for women aged 27–45 who may still benefit. The vaccine does NOT protect against all high-risk HPV types and does NOT replace the need for cervical screening — vaccinated women must still undergo regular screening because the vaccine does not cover all oncogenic types and provides no therapeutic benefit against existing infections.
Provided image
SELF-CHECK
A 12-year-old girl presents with her mother for HPV vaccination. How many doses of the HPV vaccine does she require, and what is the recommended schedule?
A. Three doses at 0, 1, and 6 months
B. Two doses at 0 and 6 months
C. Single dose — one dose is sufficient for girls under 14
D. Two doses at 0 and 3 months
Reveal Answer
Answer: B. Two doses at 0 and 6 months
Girls aged 9–14 years have a more robust immune response and generate antibody titres equivalent to a three-dose schedule when given only two doses at 0 and 6 months. The three-dose schedule (0, 1–2, 6 months) is reserved for those aged ≥15 years or immunocompromised individuals. A single dose is not the approved schedule for any age group in current WHO or NHM India guidelines.
Colposcopy: Technique and Interpretation of Findings
Colposcopy is the standard diagnostic investigation following an abnormal VIA, Pap smear, or HPV test result. It is not a screening test — it is a diagnostic procedure performed in a referral facility to identify the site and severity of abnormality and to guide biopsy. The colposcope is a binocular stereomicroscope with a variable magnification (typically ×6 to ×40) and a bright coaxial light source; the green filter reduces the red background and enhances the visibility of vascular patterns. A final-year student should understand the procedure and its findings well enough to participate in bedside teaching and to interpret a colposcopy report.
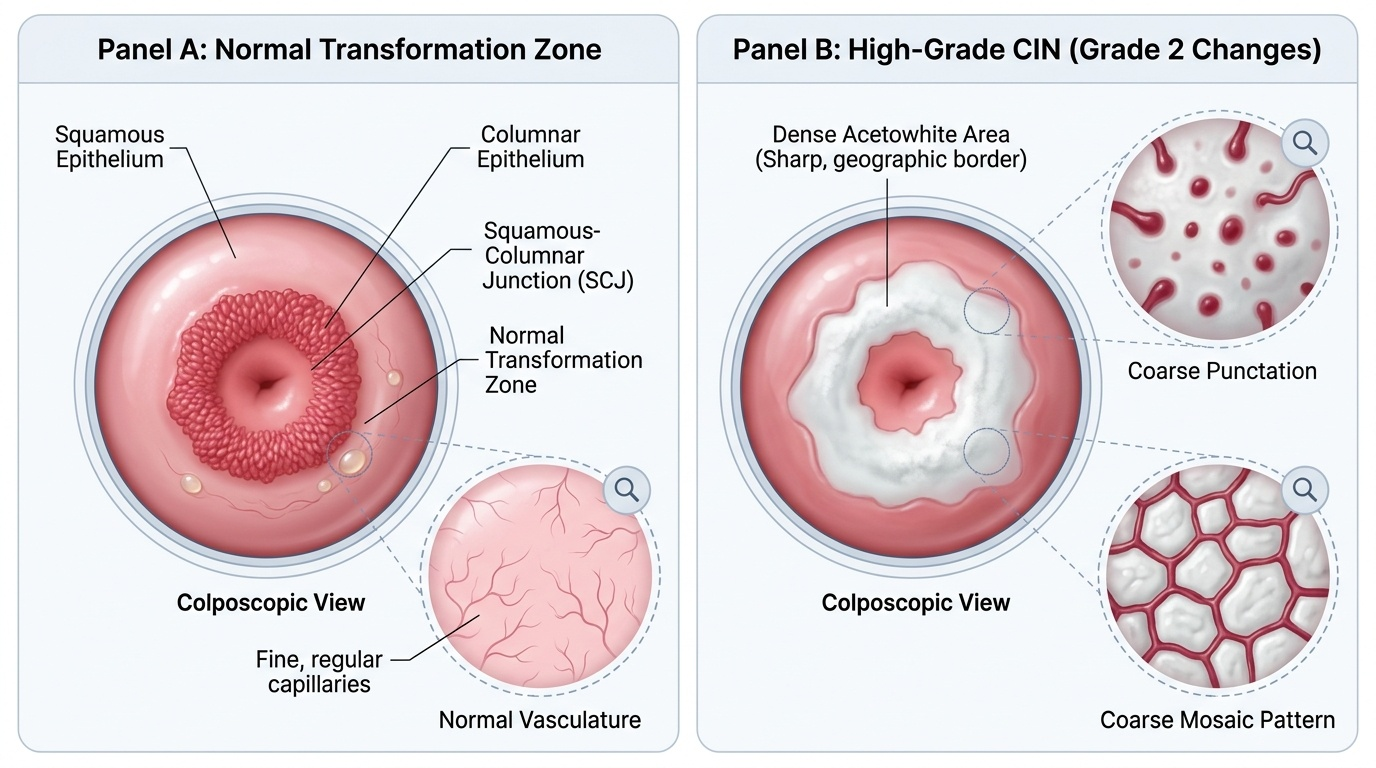
The procedure begins with insertion of a speculum and inspection of the cervix at low magnification. A saline wash removes mucus; then 3–5% acetic acid is applied and the cervix is inspected after one minute for acetowhite changes, noting their location (within or outside the TZ), density (thin/translucent vs dense/opaque), borders (irregular/feathered = low-grade vs sharp/geographic = high-grade), and whether they extend to the SCJ or into the endocervical canal. Lugol's iodine is then applied to confirm the Schiller's test negative area. The colposcopist classifies the examination as satisfactory (entire TZ and SCJ visible) or unsatisfactory (SCJ not fully visible, usually post-menopausal or with endocervical lesion), which determines whether directed biopsy alone or ECC is needed.
Abnormal colposcopic findings are graded by the IFCPC 2011 classification into Grade 1 (minor changes — thin acetowhite, fine punctation or mosaic, irregular border) and Grade 2 (major changes — dense acetowhite, coarse punctation or mosaic, sharp/geographic border, ridge sign, inner border sign). Atypical vessels (irregular calibre, course, and intercapillary distance — 'corkscrew', 'comma', 'spaghetti') raise the suspicion of invasive cancer. Directed punch biopsy is taken from the most abnormal area; multiple biopsies are taken if the abnormality is extensive. The biopsy provides the histological diagnosis (CIN 1/2/3 or invasive cancer), which determines subsequent management (surveillance vs treatment vs staging workup).
Provided image
SELF-CHECK
On colposcopy after a Pap smear showing HSIL, you see a dense acetowhite area with a sharp geographic border at the transformation zone. The entire squamocolumnar junction is visible. What is the correct next step?
A. Repeat Pap smear in 6 months
B. Refer directly for Wertheim's hysterectomy
C. Take colposcopy-directed punch biopsy from the most abnormal area
D. Apply Lugol's iodine and if VILI-positive, treat with cryotherapy immediately
Reveal Answer
Answer: C. Take colposcopy-directed punch biopsy from the most abnormal area
Dense acetowhite with sharp geographic borders is a Grade 2 (major) colposcopic change corresponding to high-grade CIN. The satisfactory colposcopy (entire SCJ visible) means directed biopsy can be taken from the most abnormal area to obtain histological diagnosis before any treatment decision. Empirical treatment without histology is not standard practice for major colposcopic changes — only the screen-and-treat (VIA+/cryotherapy) strategy allows same-visit treatment, and only for eligible lesions. Hysterectomy is not indicated without histological confirmation of CIN 2/3.
Applied Practice: Screening Algorithms and the Screen-and-Treat Strategy
Translating individual screening methods into an organised programme requires choosing the most appropriate algorithm for the clinical and resource context. India operates at multiple levels — from the tertiary referral hospital with full colposcopy and HPV DNA testing to the village-level health and wellness centre where only VIA and treatment may be available — and the screening pathway must be adapted accordingly.
The NHM India recommended approach for the community level uses either HPV DNA testing (preferred, for facilities with laboratory access) or VIA (where laboratory is unavailable) as the primary test for women aged 30–65 years. Women who test positive are triaged: at facilities offering colposcopy, VIA-positive or HPV-positive women are referred for colposcopic assessment and directed biopsy before treatment. At facilities with only basic equipment, the screen-and-treat strategy is used: women with a VIA-positive result who meet eligibility criteria (lesion in the TZ, not extending into the canal, covering <75% of the cervix, with no suspicion of invasion or glandular disease) are treated on the same visit with cryotherapy (nitrous oxide or carbon dioxide to freeze the cervical lesion) or LEEP/thermal ablation — eliminating the barriers of referral default and loss to follow-up that cause most treatment failures in low-resource settings.
The WHO 2021 guidelines recommend HPV DNA testing as the primary screening test, with either direct treatment (for VIA-confirmed positive) or colposcopy triage for those who are HPV-positive but VIA-negative. The 2021 update also supports ablative treatment without histological confirmation when HPV testing is the primary modality and visual assessment confirms the lesion is amenable to ablation — a shift from the traditional biopsy-before-treatment paradigm that was feasible only with laboratory infrastructure.
Challenges in India that undermine screening programme effectiveness include: (a) low awareness among women, particularly in rural communities, about the existence and importance of screening; (b) cultural stigma and privacy concerns about gynaecological examination; (c) healthcare provider shortage — too few trained staff to offer VIA at PHC level; (d) cold chain and supply issues for cryotherapy equipment; (e) referral chain gaps — women referred to colposcopy centres often default. Effective programme design addresses each of these: community health workers as initial contacts, fixed-day screening camps at the sub-centre, co-location of screening and treatment, and tracking systems for positive women.
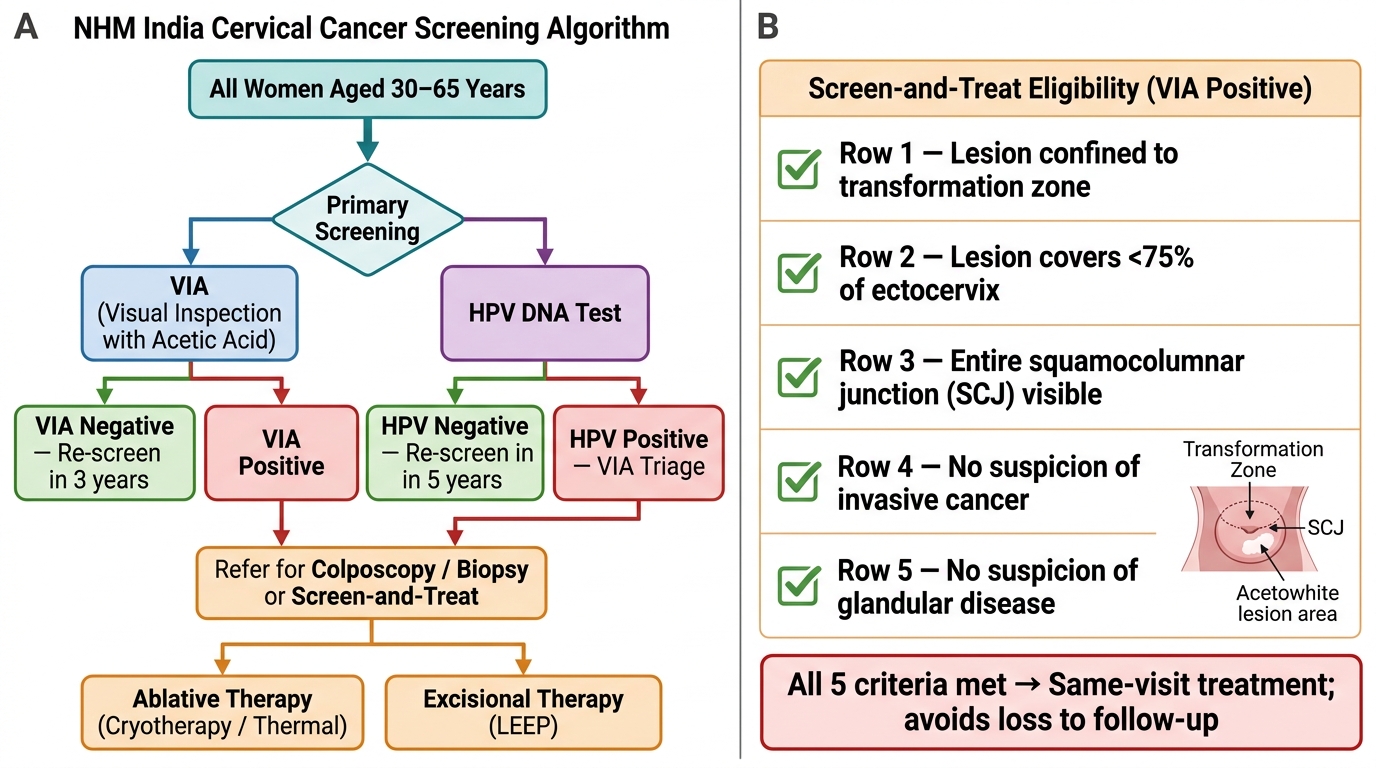
NHM India Cervical Cancer Screening Algorithm and Screen-and-Treat Eligibility Criteria
SELF-CHECK
A 36-year-old woman at a rural health sub-centre has a VIA-positive result with an acetowhite lesion at the transformation zone covering approximately 30% of the ectocervix, with the entire squamocolumnar junction visible. There is no suspicion of invasive cancer. What is the most appropriate immediate action according to the NHM India screen-and-treat strategy?
A. Refer for colposcopy-directed biopsy before any treatment
B. Perform Pap smear and await cytology report
C. Treat with cryotherapy on the same visit
D. Arrange HPV DNA testing to confirm before treatment
Reveal Answer
Answer: C. Treat with cryotherapy on the same visit
The screen-and-treat strategy allows immediate same-visit cryotherapy (or LEEP/thermal ablation) for VIA-positive women when the lesion meets eligibility criteria: confined to transformation zone, <75% of cervix, entire SCJ visible, no suspicion of invasion or glandular disease. This eliminates the loss-to-follow-up that occurs when women are referred to distant colposcopy centres. This scenario meets all eligibility criteria.