Page 7 of 37
OG33.3-4 | Cervical Cancer Screening and Prevention — SDL Guide (Part 3)
Self-Assessment
This self-assessment section is designed to help you verify that you have mastered the core factual and procedural competencies covered in this module. Cervical cancer screening and prevention occupy a unique position in clinical medicine: they combine hands-on clinical skills (performing VIA, interpreting colposcopy), evidence-based test selection (VIA versus HPV DNA testing in different resource contexts), and public health reasoning (vaccination schedules, population-level programme design). The examination questions that draw on this topic test all three levels — isolated recall of Bethesda categories and vaccine schedules, application to clinical scenarios (which woman qualifies for same-visit cryotherapy?), and higher-order reasoning about programmatic decisions. Review each point below and ensure you can reproduce it from memory, then attempt the integrative scenario: a 40-year-old woman at a rural PHC has a VIA-positive result; trace the decision tree from the result to the final outcome.
- VIA technique: 3–5% acetic acid, wait exactly 1 minute, sharp demarcated acetowhite in the TZ = positive.
- VILI: Lugol's iodine, mustard-yellow non-staining in TZ = positive; complements VIA.
- Pap smear Bethesda terms: NILM (normal) → ASCUS → LSIL (CIN 1) → HSIL (CIN 2/3) → carcinoma; single-smear sensitivity ~55%.
- HPV DNA testing: highest sensitivity (~95%), preferred primary test (NHM India + WHO 2021); 5-year re-test interval if negative.
- HPV vaccine schedules: 2-dose (0, 6 months) for age 9–14; 3-dose (0, 1–2, 6 months) for age ≥15 or immunocompromised.
- Quadrivalent: HPV 6, 11, 16, 18; 9-valent: adds 31, 33, 45, 52, 58; Cervavac: India-made quadrivalent.
- Screen-and-treat criteria: VIA-positive + lesion in TZ + <75% cervix + no canal extension + no invasion suspicion → same-visit cryotherapy.
- Colposcopy: Grade 2 major changes (dense acetowhite, coarse punctation/mosaic, sharp borders) = high-grade CIN → directed biopsy.
- NHM India target: screen women aged 30–65 every 5 years; WHO 90-70-90 elimination targets.
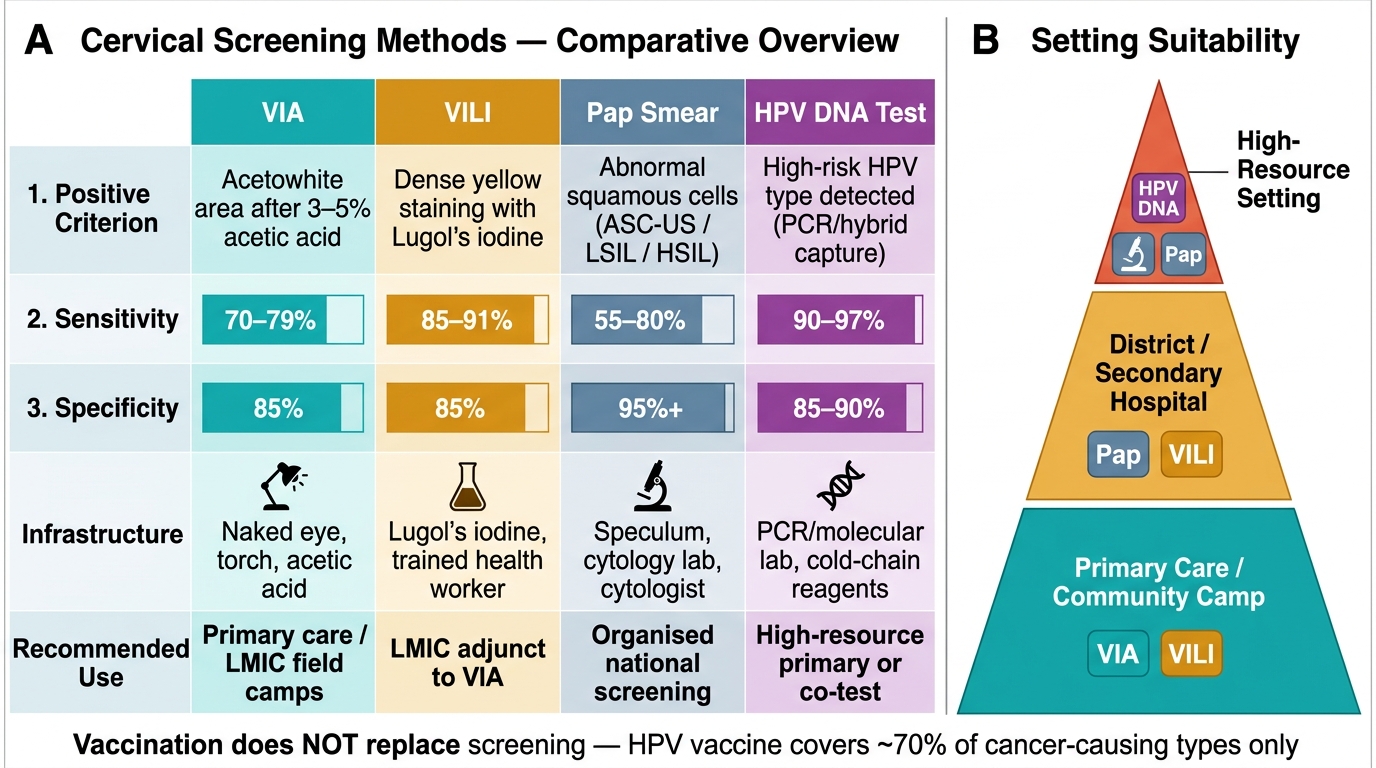
Comparative Overview of Cervical Screening Methods: VIA, VILI, Pap Smear, and HPV DNA Test
CLINICAL PEARL
A vaccinated woman still needs cervical cancer screening. This is one of the most common misconceptions in clinical practice: parents and women often believe that HPV vaccination completely eliminates the need for future smears or VIA. This is incorrect for two reasons. First, the quadrivalent vaccine covers HPV 16 and 18 (~70% of cervical cancers) but not all high-risk types (31, 33, 45, 52, 58 — responsible for approximately 15–20% more). Second, the vaccine provides no therapeutic benefit against HPV infections already present at the time of vaccination. Therefore, vaccinated women remain at risk from non-vaccine HPV types and from pre-existing infections, and must continue participating in the cervical screening programme from age 25–30 per the recommended schedule.