Page 20 of 37
OG34.3 | Gestational Trophoblastic Disease — SDL Guide
Learning Objectives
- Describe the clinical presentation of gestational trophoblastic disease (GTD) across the spectrum from hydatidiform mole to choriocarcinoma
- Distinguish complete from partial hydatidiform mole on genetic, histological, and clinical grounds
- Classify gestational trophoblastic neoplasia (GTN) using FIGO anatomical staging (I–IV)
- Apply the WHO/FIGO prognostic scoring system to determine low-risk (≤6) vs high-risk (≥7) GTN
- Interpret serial serum β-hCG trends (plateau, rise, normalisation) as the primary monitoring tool for GTN
- Outline the management of low-risk GTN (single-agent methotrexate/actinomycin-D) and high-risk GTN (EMA-CO)
- Frame this SDL as the oncologic staging and management view of GTD, cross-referencing OG9.5 for the acute early-pregnancy presentation
INSTRUCTIONS
Gestational trophoblastic disease (GTD) is a unique group of tumours that arise from placental trophoblastic tissue following any pregnancy — whether a molar pregnancy, abortion, ectopic, or even a normal term delivery. GTD is medically remarkable: choriocarcinoma, one of the most aggressive human malignancies, is also one of the most curable cancers known — with cure rates exceeding 90% even in metastatic disease when treated at a specialist centre. This module covers the oncological staging and management of GTD. The acute clinical presentation of molar pregnancy and initial emergency management is covered in OG9.5 (cluster 169, the early-pregnancy complications module) — this SDL picks up where that one ends, taking the perspective of long-term oncological management.
References
- DC Dutta's Textbook of Gynecology, 7th ed., Ch 11 — Gestational Trophoblastic Disease (textbook)
- Shaw's Textbook of Gynaecology, 17th ed., Ch 12 — Gestational Trophoblastic Disease (textbook)
- FIGO Oncology Committee — FIGO Staging for Gestational Trophoblastic Neoplasia 2000 (updated 2009) (guideline)
- RCOG Green-top Guideline No. 38 — Management of Gestational Trophoblastic Disease (2020) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman returns to the gynaecology clinic six weeks after suction evacuation of a complete hydatidiform mole. She had been referred for serial β-hCG monitoring. Her β-hCG at evacuation was 95,000 mIU/mL. Over the following three weekly measurements it has trended: 42,000 → 38,500 → 37,900 mIU/mL. She is now complaining of irregular vaginal bleeding and a persistent feeling of nausea. Ultrasound shows a 3 cm heterogeneous lesion within the uterine myometrium with prominent vascularity. Her chest X-ray shows two small nodular densities in the right lower lobe. The team is concerned about malignant transformation — but what is the specific diagnosis, how is it staged, and what determines whether she needs one drug or six?
WHY THIS MATTERS
Gestational trophoblastic disease represents one of the great success stories of oncology: a disease that, if managed with serial β-hCG monitoring and appropriate chemotherapy, is curable in nearly all cases — even in the setting of widespread metastasis. India has a high incidence of hydatidiform mole compared to Western countries (approximately 1 in 400 pregnancies vs 1 in 1,000–2,000 in Western populations), though data vary by region and ascertainment. Every gynaecologist must be able to identify the risk factors for malignant transformation after a molar pregnancy, initiate and interpret the β-hCG monitoring protocol, calculate the WHO/FIGO prognostic score, and ensure timely referral to a GTD treatment centre. Failure to follow up a molar pregnancy with serial β-hCG is a recognised medicolegal risk — persistent GTN can progress silently to metastatic choriocarcinoma if monitoring is abandoned. This module frames GTD from the oncological staging perspective; the acute clinical presentation and initial surgical management of molar pregnancy are covered in OG9.5 (cluster 169 — Early Pregnancy Complications), which you should read in conjunction with this SDL.
RECALL
Before proceeding, activate relevant prior knowledge. From OG9.5 (early-pregnancy complications), recall the clinical diagnosis of molar pregnancy: excessive uterine size for dates, 'snowstorm' appearance on ultrasound, markedly elevated β-hCG, and the procedure of suction evacuation — this SDL begins after that initial management. From physiology, recall that β-hCG is produced by the syncytiotrophoblast and normally peaks at 10 weeks of pregnancy then declines — understanding this normal curve is essential for interpreting post-molar β-hCG trends. From biochemistry, recall that β-hCG has a serum half-life of approximately 24–36 hours — which means a marked plateau or rise in serial weekly measurements signals abnormal trophoblastic activity rather than retained normal pregnancy tissue. From genetics, recall the concept of ploidy: diploid (46 chromosomes, normal) vs triploid (69 chromosomes) — complete and partial moles differ in ploidy, and this explains their different biology and malignant potential.
Clinical Presentation and the GTD Spectrum
Gestational trophoblastic disease (GTD) encompasses a spectrum from benign hydatidiform mole to frankly malignant gestational trophoblastic neoplasia (GTN), all sharing the common feature of abnormal trophoblastic proliferation following a pregnancy. The clinical presentations vary considerably depending on where on this spectrum a patient sits, and understanding the natural history of each entity guides surveillance and intervention decisions.
A hydatidiform mole typically presents in the first trimester with: (1) disproportionate uterine enlargement (uterus large for dates in ~50% of complete moles, though may be normal or even small in partial moles); (2) hyperemesis — due to markedly elevated β-hCG stimulating thyroid-stimulating hormone receptors (β-hCG has structural homology with TSH); (3) vaginal bleeding — the most consistent presenting symptom, often passage of grape-like vesicles (pathognomonic of complete mole); (4) pre-eclampsia before 20 weeks (a classic teaching point — pre-eclampsia developing before the usual gestational threshold is suspicious for molar pregnancy or multiple pregnancy); (5) bilateral theca lutein cysts on ultrasound (from excessive β-hCG stimulation of the ovary, present in ~25–30% of complete moles). These features and the initial management — ultrasound diagnosis, suction evacuation, tissue histology — are covered in OG9.5. This SDL picks up from the point of tissue diagnosis and focuses on oncological staging and management.
Post-molar GTN presents typically 4–8 weeks after evacuation, though the interval can extend to months. The clinical flags are: persistently elevated or rising β-hCG on serial monitoring, irregular vaginal bleeding, new respiratory symptoms (haemoptysis, dyspnoea from pulmonary metastases), or neurological symptoms (brain metastases). In some cases there are no symptoms — the diagnosis is made purely from serial β-hCG surveillance (the rationale for mandatory post-molar monitoring).
Choriocarcinoma arising after a non-molar pregnancy (spontaneous abortion, ectopic, or even term delivery) poses a diagnostic challenge because there is no antecedent mole to trigger the clinician's suspicion. Any woman of reproductive age with abnormal uterine bleeding, haemoptysis, or unexplained neurological symptoms after a recent pregnancy should have a serum β-hCG measured — the diagnosis can be confirmed biochemically before histological sampling and before potentially life-threatening surgical intervention into a highly vascular tumour.
Placental-site trophoblastic tumour (PSTT) and epithelioid trophoblastic tumour (ETT) are rare, slow-growing GTN variants arising from intermediate trophoblast. They have characteristic features that distinguish them from choriocarcinoma: β-hCG is relatively low (often <1,000 mIU/mL despite uterine disease), and they are relatively resistant to standard chemotherapy — hysterectomy is the primary treatment.
Provided image
Pathology and Classification of GTD
The pathological classification of GTD rests on the cell of origin within the trophoblast and the degree of malignancy. Understanding the genetic basis of complete vs partial mole explains their entirely different clinical behaviours and is a reliable knowledge anchor for examinations.
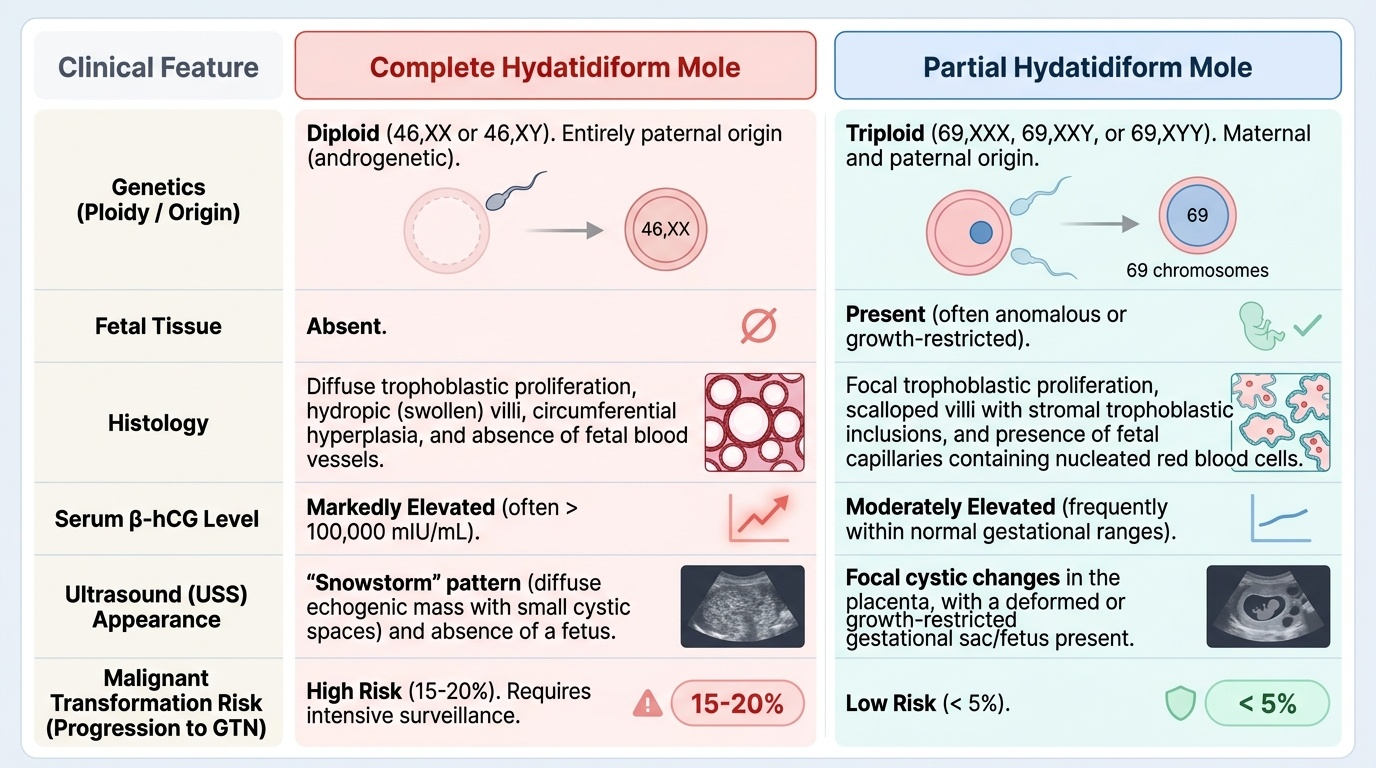
Complete hydatidiform mole (CHM) is genetically diploid (46,XX in 90%, or 46,XY in 10%) and androgenetic — both chromosome sets originate from paternal sperm (dispermy fertilising an empty egg, or a single sperm that duplicates). Because the maternal chromosomes are absent, there is no fetal or embryonic tissue. Histologically, CHM shows generalised trophoblastic hyperplasia and diffuse hydropic change (swelling) of the villi. The hallmark clinical feature is markedly elevated β-hCG. The risk of malignant transformation to GTN is approximately 15–20%.
Partial hydatidiform mole (PHM) is genetically triploid (69,XXX, 69,XXY, or 69,XYY), arising from fertilisation of a normal egg by two sperm (dispermy). It retains a maternal contribution and typically shows fetal or embryonic tissue (though the fetus is abnormal and non-viable). Histologically, only some villi are hydropic, and there is focal trophoblastic hyperplasia. β-hCG is less dramatically elevated than in CHM. The risk of malignant transformation is much lower at approximately 0.5–5%.
Gestational trophoblastic neoplasia (GTN) is the term for the malignant entities in the GTD spectrum. It includes:
- Invasive mole: a hydatidiform mole (most commonly CHM) that invades the myometrium or uterine vasculature. The villi are recognisably molar. It can rarely cause uterine perforation or metastasise but usually responds well to chemotherapy.
- Choriocarcinoma: a frankly malignant tumour of cytotrophoblast and syncytiotrophoblast, characterised by absent chorionic villi (this is the key histological feature distinguishing it from invasive mole), sheets of haemorrhagic, necrotic tumour, and extensive vascular invasion. It can follow any form of pregnancy — molar, abortive, ectopic, or term. It is extremely chemosensitive.
- Placental-site trophoblastic tumour (PSTT): arises from intermediate trophoblast at the implantation site; secretes human placental lactogen (hPL) more than β-hCG; relatively chemoresistant; hysterectomy is the preferred treatment.
- Epithelioid trophoblastic tumour (ETT): another intermediate trophoblast tumour; forms nodular masses in the uterine fundus or lower segment; also relatively chemoresistant; hysterectomy preferred.
The pathological report of the suction evacuation specimen is critical: it determines whether the patient has CHM or PHM (setting the surveillance intensity) and whether GTN features (myoinvasion, absent villi with pleomorphic trophoblast sheets) are already present in the initial specimen.
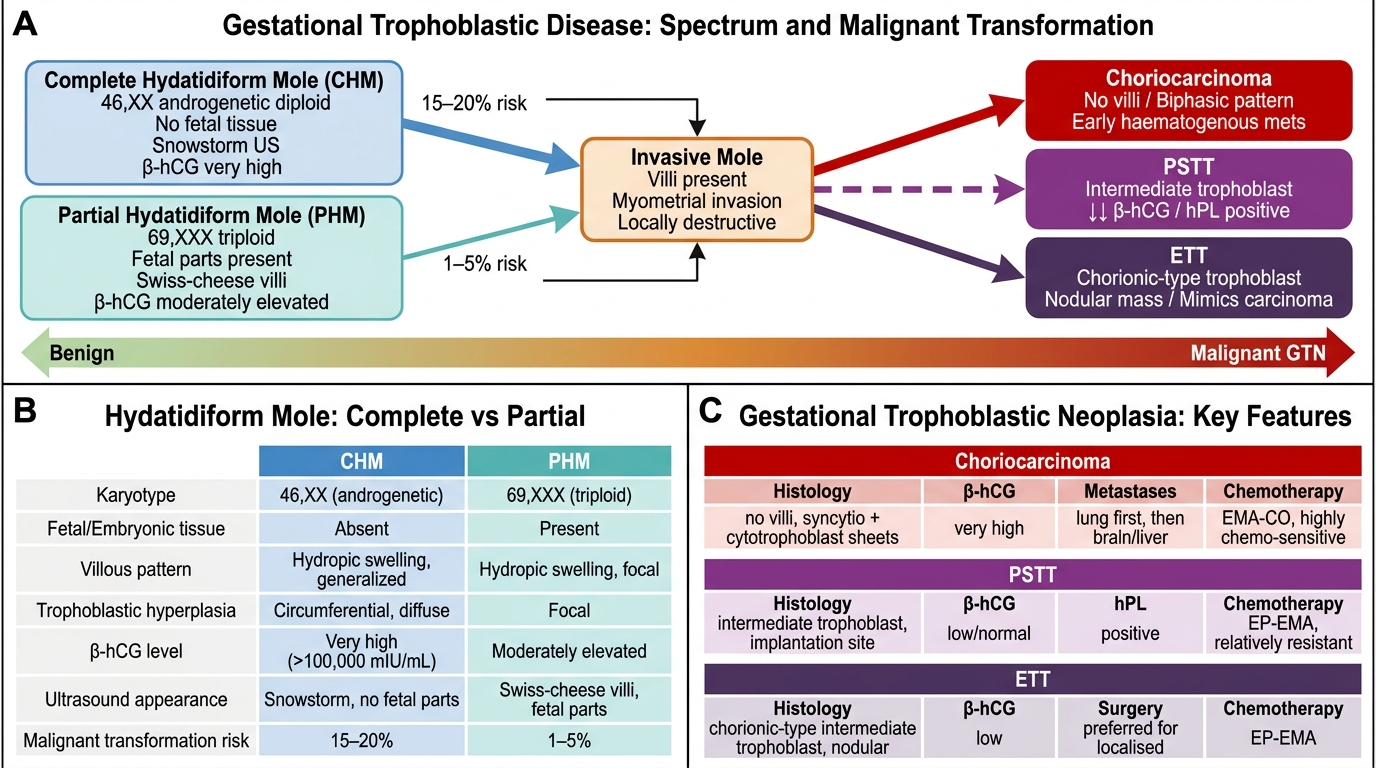
Gestational Trophoblastic Disease: Spectrum, Malignant Transformation Risk, and Key Distinguishing Features
FIGO Staging and WHO Prognostic Scoring
Gestational trophoblastic neoplasia is staged using two parallel systems that together determine the treatment regimen. The FIGO anatomical staging (2000) identifies where the disease is anatomically — confined to the uterus, spread to genital structures, reaching the lungs, or involving distant organs. The WHO/FIGO prognostic scoring system quantifies the biological and clinical risk of treatment failure with single-agent chemotherapy, capturing patient- and disease-specific variables that imaging cannot convey. Both systems must be applied together, and this dual-system approach is unique to GTN in oncology: the FIGO stage alone is insufficient to determine treatment (a Stage III patient with score 5 receives single-agent therapy, while a Stage III patient with score 9 requires multi-agent EMA-CO), and the prognostic score alone is insufficient without knowing whether the disease is confined to the uterus or has metastasised. This dual framework was developed because clinical experience showed that anatomical extent and biological risk do not always correlate — pulmonary metastases (Stage III) from a complete mole shortly after evacuation in a young woman may carry very low chemotherapy-failure risk, while uterine-confined disease after a term pregnancy many months later may carry substantially higher risk.
The FIGO anatomical staging for GTN is:
- Stage I: disease confined to the uterus
- Stage II: GTN extends outside the uterus but is limited to the genital structures (adnexa, vagina, broad ligament)
- Stage III: GTN extends to the lung(s), with or without known genital tract involvement
- Stage IV: all other distant metastatic sites (brain, liver, kidney, GI tract)
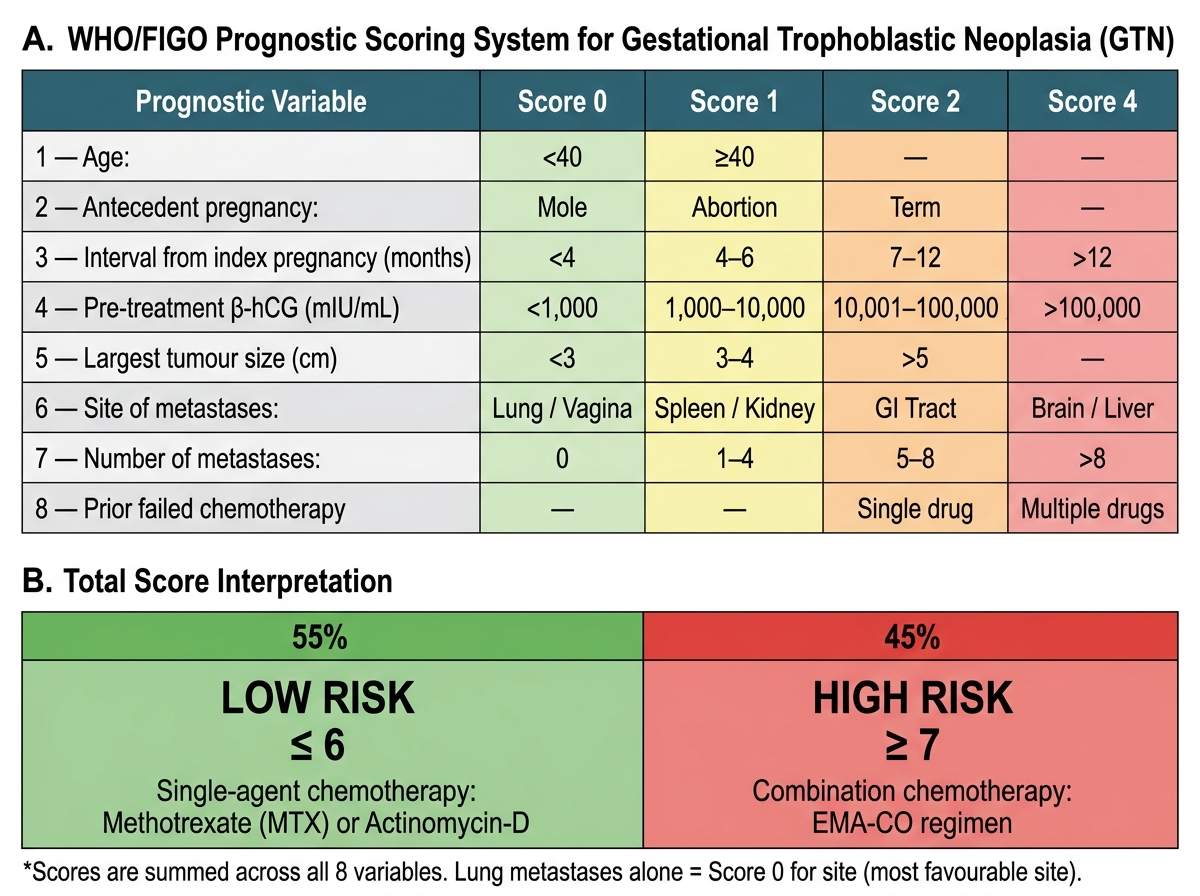
The WHO/FIGO Prognostic Scoring System assigns a numerical score based on eight prognostic variables. The total score determines the risk category:
- Low risk: total score ≤6 → single-agent chemotherapy (methotrexate or actinomycin-D)
- High risk: total score ≥7 → multi-agent chemotherapy (EMA-CO)
The eight scoring variables and their weights (0/1/2/4 points each) are: (1) Age (<40 = 0; ≥40 = 1); (2) Antecedent pregnancy (mole = 0; abortion = 1; term = 2); (3) Interval from index pregnancy to treatment (<4 months = 0; 4–6 months = 1; 7–12 months = 2; >12 months = 4); (4) Pre-treatment β-hCG (mIU/mL) (<1,000 = 0; 1,000–10,000 = 1; >10,000–100,000 = 2; >100,000 = 4); (5) Largest tumour size including uterus (<3 cm = 0; 3–4 cm = 1; ≥5 cm = 2); (6) Site of metastases (lung = 0; spleen/kidney = 1; GI tract = 2; liver/brain = 4); (7) Number of metastases (0 = 0; 1–4 = 1; 5–8 = 2; >8 = 4); (8) Prior chemotherapy (none = 0; single agent = 2; ≥2 agents = 4).
This staging and scoring framework makes GTN one of the few cancers where the treatment regimen is determined algorithmically and quantitatively — a powerful concept that has driven the extraordinary cure rates in this disease.
WHO/FIGO Prognostic Scoring System for GTN and Risk-Based Treatment Stratification
SELF-CHECK
A 24-year-old woman, 5 months after evacuation of a complete mole, has β-hCG 12,000 mIU/mL, a 4 cm uterine mass, and 3 lung nodules on CT. She has received no prior chemotherapy. Calculate her WHO/FIGO prognostic score using these variables: age <40 (0), antecedent pregnancy = mole (0), interval 4–6 months (1), β-hCG >10,000–100,000 (2), tumour 3–4 cm (1), metastases = lung (0), number of mets 1–4 (1), no prior chemotherapy (0). What is her score and risk category?
A. Score 4 — low risk
B. Score 5 — low risk
C. Score 7 — high risk
D. Score 9 — high risk
Reveal Answer
Answer: B. Score 5 — low risk
Score = 0 + 0 + 1 + 2 + 1 + 0 + 1 + 0 = 5. Score ≤6 = low risk → single-agent chemotherapy (methotrexate). Note: lung metastases alone score 0 for 'site' in the WHO system (lung is the most favourable metastatic site and does not upstage to high-risk by itself). High-risk threshold is ≥7.