Page 21 of 37
OG34.3 | Gestational Trophoblastic Disease — SDL Guide (Part 2)
Investigations and Serial β-hCG Monitoring
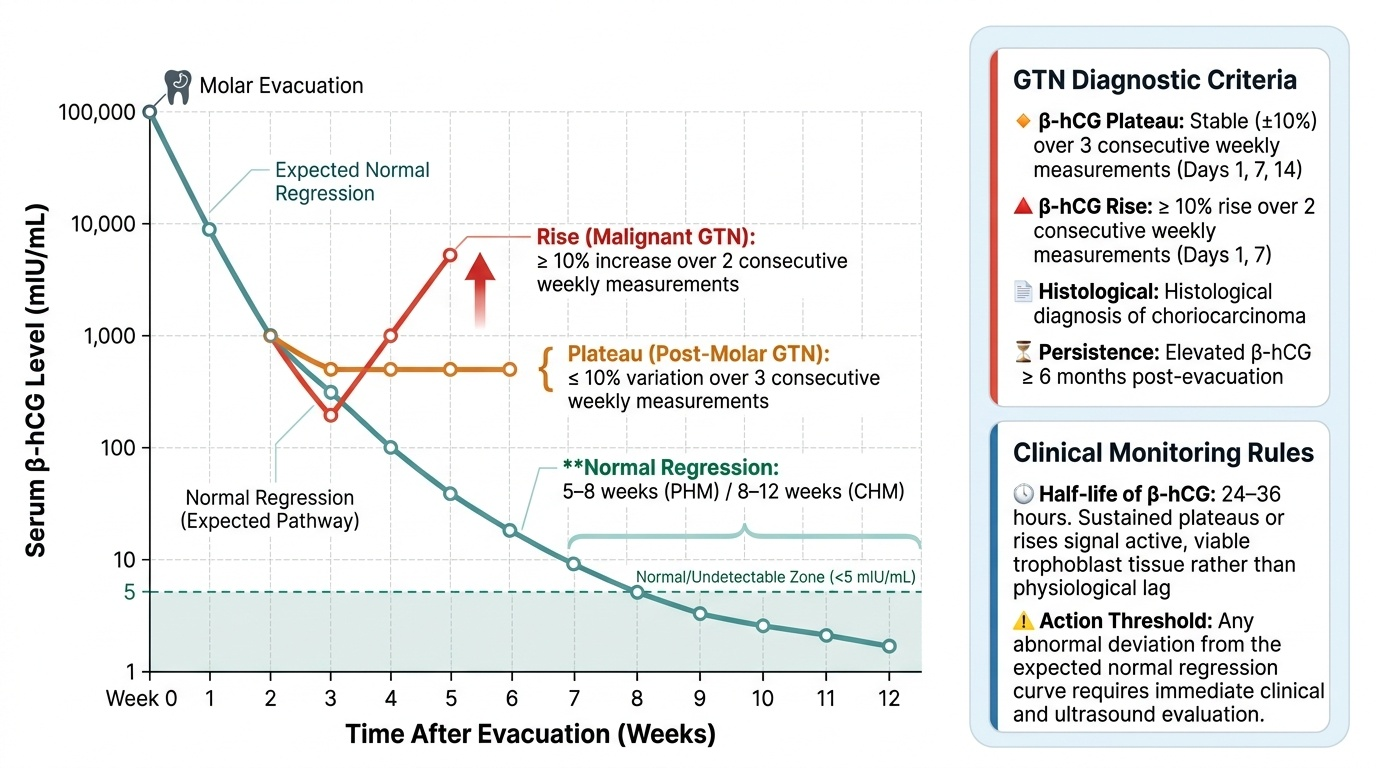
The defining investigation in GTD is serum β-hCG measurement, which functions simultaneously as a diagnostic biomarker, a treatment response monitor, and a surveillance tool for recurrence. No other solid tumour has a tumour marker as reliable, quantitative, and sensitive as β-hCG is in GTD — it is secreted by virtually all trophoblastic tissue and falls to zero when all GTD cells are eradicated. This makes β-hCG the prototype of the ideal tumour marker: it is 100% sensitive for residual disease, it changes quantitatively and proportionally to tumour cell numbers, and it can be monitored serially with inexpensive blood tests. Understanding the expected post-molar regression curve — and recognising abnormal deviations from it — is a core clinical skill that can save a patient from progressing silently to metastatic choriocarcinoma. The critical insight is that β-hCG has a half-life of approximately 24–36 hours, so a sustained plateau or rise in weekly measurements cannot be explained by physiological lag — it signals active trophoblastic cell secretion, indicating either retained viable molar tissue or malignant transformation to GTN.
The post-molar β-hCG monitoring protocol (standard practice after suction evacuation) uses weekly serum β-hCG measurements. Normal regression after CHM evacuation: β-hCG typically normalises within 8–12 weeks. After PHM, normalisation is usually faster (within 5–8 weeks). Three abnormal patterns require oncological evaluation:
1. Plateau: <10% rise or fall over three consecutive weekly measurements
2. Rise: ≥10% rise over two consecutive weekly measurements
3. Elevated β-hCG beyond 8 weeks (CHM) or 6 weeks (PHM) after evacuation without a clear downward trajectory
The diagnostic criteria for post-molar GTN (requiring treatment) per FIGO/RCOG are: (1) plateau of β-hCG for ≥3 weeks (days 1, 7, 14); (2) rise of β-hCG for ≥2 consecutive weeks (days 1, 7); (3) elevated β-hCG ≥6 months after evacuation; (4) histological diagnosis of choriocarcinoma regardless of β-hCG.
Beyond β-hCG, the investigation of suspected GTN includes: Pelvic ultrasound (transvaginal) to assess uterine dimensions, identify myometrial invasion (heterogeneous vascular lesion within myometrium), and detect theca lutein cysts. Chest X-ray is the first-line investigation for pulmonary metastases (present in ~4–5% of moles at time of evacuation, and in ~80% of choriocarcinoma). CT chest/abdomen/pelvis is the gold-standard staging investigation once GTN is diagnosed — it quantifies the number and site of metastases for WHO/FIGO scoring. MRI brain is performed if CNS metastases are suspected (headache, focal neurological signs, or ultra-high β-hCG >50,000 mIU/mL in high-risk GTN). FDG-PET has a limited role in GTN staging but may detect disease where CT and MRI are negative in selected cases.
Provided image
Differential Diagnosis
The differential diagnosis of GTD involves two related challenges: distinguishing a molar pregnancy from other causes of first-trimester complications, and — in the context of a proven molar pregnancy — distinguishing post-molar GTN from normal β-hCG regression or from retained products of conception.
First-trimester differential (before or around diagnosis): A partial mole must be distinguished from an incomplete or missed abortion — both can present with similar early-pregnancy bleeding, normal-sized uterus, and only modest β-hCG elevation. The distinction requires histological examination of evacuation tissue; ultrasound is not reliably specific for PHM (sensitivity ~40%). A complete mole is more clinically distinctive (uterus large for dates, hyperemesis, 'snowstorm' ultrasound), but early CHM before hydrops is well established can be mistaken for a complete abortion or even a normal early intrauterine pregnancy on ultrasound. Ectopic pregnancy is also in the differential of a positive pregnancy test with bleeding; β-hCG is typically much lower and rises more slowly. Twin pregnancy (normal + molar) is a rare entity — one normal foetus co-exists with molar tissue; this requires specialist management.
Post-molar differential (β-hCG not normalising): Retained products of conception following evacuation can maintain modestly elevated β-hCG without the progressive pattern of GTN; a repeat ultrasound and uterine cavity assessment help distinguish. New intrauterine pregnancy — contraception must be maintained throughout post-molar surveillance precisely to avoid this diagnostic confusion. Quiescent GTD is a rare entity where β-hCG remains slightly elevated for months without rising, representing dormant trophoblastic tissue that may eventually resolve spontaneously or progress — management is under ongoing study.
Choriocarcinoma after non-molar pregnancy: A woman with irregular uterine bleeding, haemoptysis, or neurological symptoms after any recent pregnancy — including term delivery — should have β-hCG measured. The differential of persistent post-partum bleeding includes subinvolution, retained placenta, and choriocarcinoma; the latter is the diagnosis that cannot be missed because it is highly curable if treated promptly and potentially lethal if delayed.
| Condition | β-hCG Level | Ultrasound | Key Distinguishing Feature |
|---|---|---|---|
| Complete mole | Very high (often >100,000) | Snowstorm, no fetus | Trophoblastic proliferation on histology |
| Partial mole | Moderately elevated | Fetal parts + hydropic villi | Triploid on FISH/flow cytometry |
| Incomplete abortion | Low-moderately elevated | Retained products, no villi | No trophoblastic hyperplasia on histology |
| Post-molar GTN | Plateau or rising | Vascular myometrial lesion | Meets FIGO diagnostic criteria |
| New pregnancy | Rising (normal doubling) | IUP or no IUP (ectopic) | LMP/history; resolves conceptually with scan |
| Choriocarcinoma (post-term) | Elevated (variable) | Uterine mass, metastases | Antecedent pregnancy; absent villi on biopsy |
SELF-CHECK
A 32-year-old woman had suction evacuation of a complete hydatidiform mole 10 weeks ago. Her β-hCG at weeks 2, 4, 6, 8, and 10 post-evacuation was 8,000 → 4,200 → 3,800 → 3,650 → 3,620 mIU/mL. She is asymptomatic. What is the correct next step?
A. Reassure — β-hCG is declining and will normalise with further waiting
B. Diagnose post-molar GTN (plateau criterion met) and initiate WHO/FIGO scoring and chemotherapy workup
C. Repeat evacuation of the uterine cavity
D. Start methotrexate empirically without further staging investigations
Reveal Answer
Answer: B. Diagnose post-molar GTN (plateau criterion met) and initiate WHO/FIGO scoring and chemotherapy workup
The β-hCG has plateaued: from week 6 to week 10 (three consecutive measurements over 3 weeks), the values are 3,800 → 3,650 → 3,620 — a <10% change across three weekly measurements meets the FIGO plateau criterion for post-molar GTN. The next step is to confirm the diagnosis, calculate the WHO/FIGO prognostic score (requiring CT chest/abdomen/pelvis), and then determine whether she is low-risk (→ methotrexate) or high-risk (→ EMA-CO). Treatment should not begin without staging. Repeat evacuation is not appropriate once GTN is suspected and adds bleeding risk.
Management of Low-Risk GTN
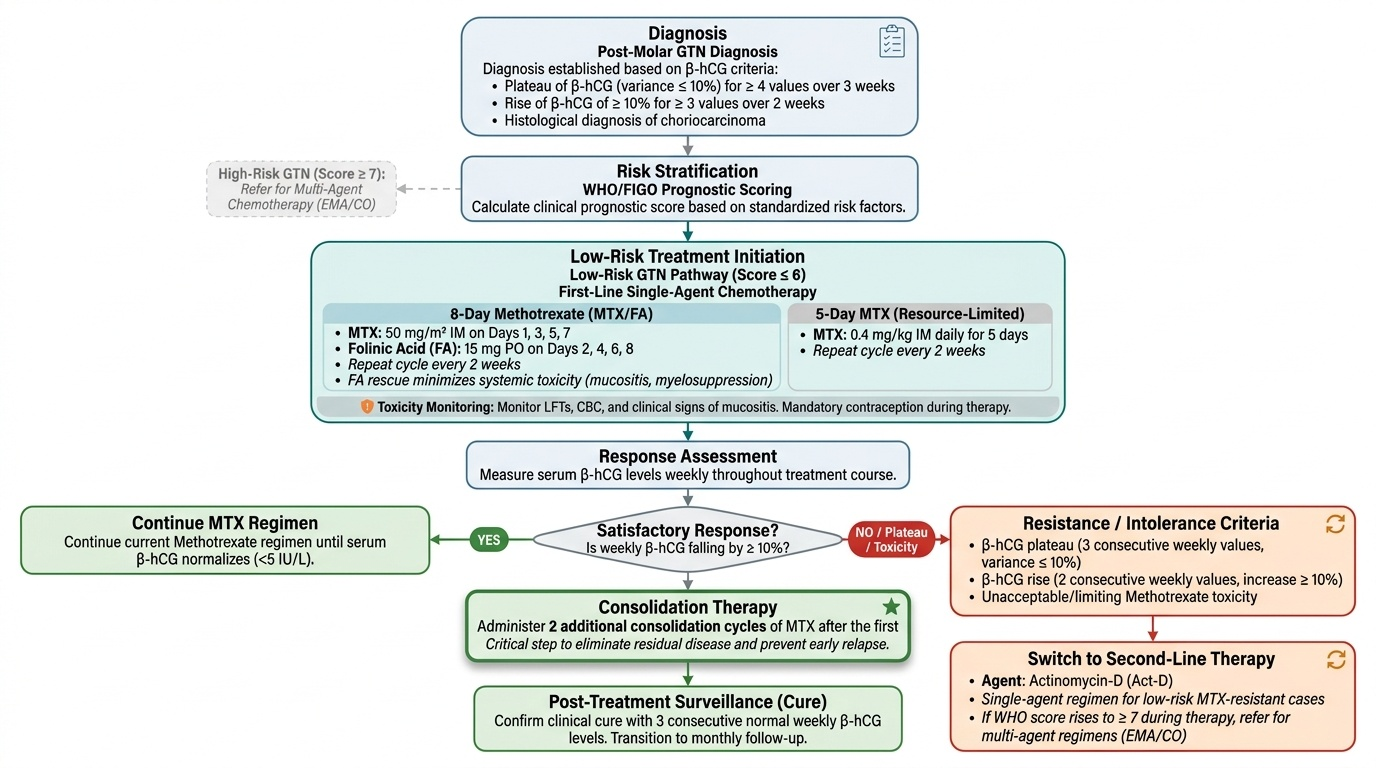
Low-risk GTN (WHO/FIGO prognostic score ≤6) is treated with single-agent chemotherapy, achieving cure rates of 85–95% with primary treatment. The two agents used are methotrexate and actinomycin-D, with methotrexate being the preferred first-line agent in most international protocols due to its long track record, predictable toxicity profile, and lower emetic potential compared to actinomycin-D.
Methotrexate regimens in low-risk GTN: the most widely used schedule is methotrexate 50 mg/m² IM on days 1, 3, 5, 7 alternating with folinic acid (leucovorin) 15 mg oral on days 2, 4, 6, 8, repeating every 2 weeks. The folinic acid rescue prevents methotrexate toxicity (mucositis, myelosuppression) by rescuing normal host cells while allowing the anti-folate effect against the rapidly dividing trophoblast. An alternative simpler regimen (used in resource-limited settings) is methotrexate 0.4 mg/kg IM daily for 5 days, every 2 weeks. Toxicities of methotrexate include mucositis, bone marrow suppression, hepatotoxicity (liver function should be monitored), and teratogenicity (contraception is mandatory).
Response assessment: β-hCG is measured weekly throughout treatment. A satisfactory response is a fall of ≥10% in β-hCG per week. Treatment continues until β-hCG normalises, then two consolidation courses are given after the first normal β-hCG value to eliminate any residual subclinical disease — this consolidation is a critical step that prevents early relapse.
Criteria for cure (post-treatment): three consecutive normal weekly serum β-hCG values (<2 mIU/mL or <5 mIU/mL depending on assay).
Resistance to methotrexate is defined as: (1) β-hCG plateau or rise after two consecutive courses of methotrexate; or (2) development of new metastases during methotrexate. First-line switch is to actinomycin-D (500 μg IV every 2 weeks, or 1.25 mg/m² every 2 weeks). If resistance to both single agents develops, recalculate the prognostic score — if now ≥7, switch to EMA-CO multi-agent regimen.
Contraception during surveillance and treatment: oral contraceptive pill is the recommended method (does not affect β-hCG and also suppresses endogenous LH which can cross-react with some β-hCG assays). IUCDs should be avoided until β-hCG normalises (risk of uterine perforation in highly vascular GTN). Pregnancy must be delayed for at least 12 months after completing surveillance.
Provided image