Page 29 of 37
OG34.5 | Major Operative Gynaecology — SDL Guide (Part 2)
Myomectomy, Ovarian Surgery, and Staging Laparotomy
These abdominal procedures share the same operative principles as hysterectomy — systematic exposure, haemostasis before division, identification of the ureter — but each has specific technical considerations that reflect its unique objective (fibroid removal with uterine preservation, ovarian tumour management, or cancer staging).
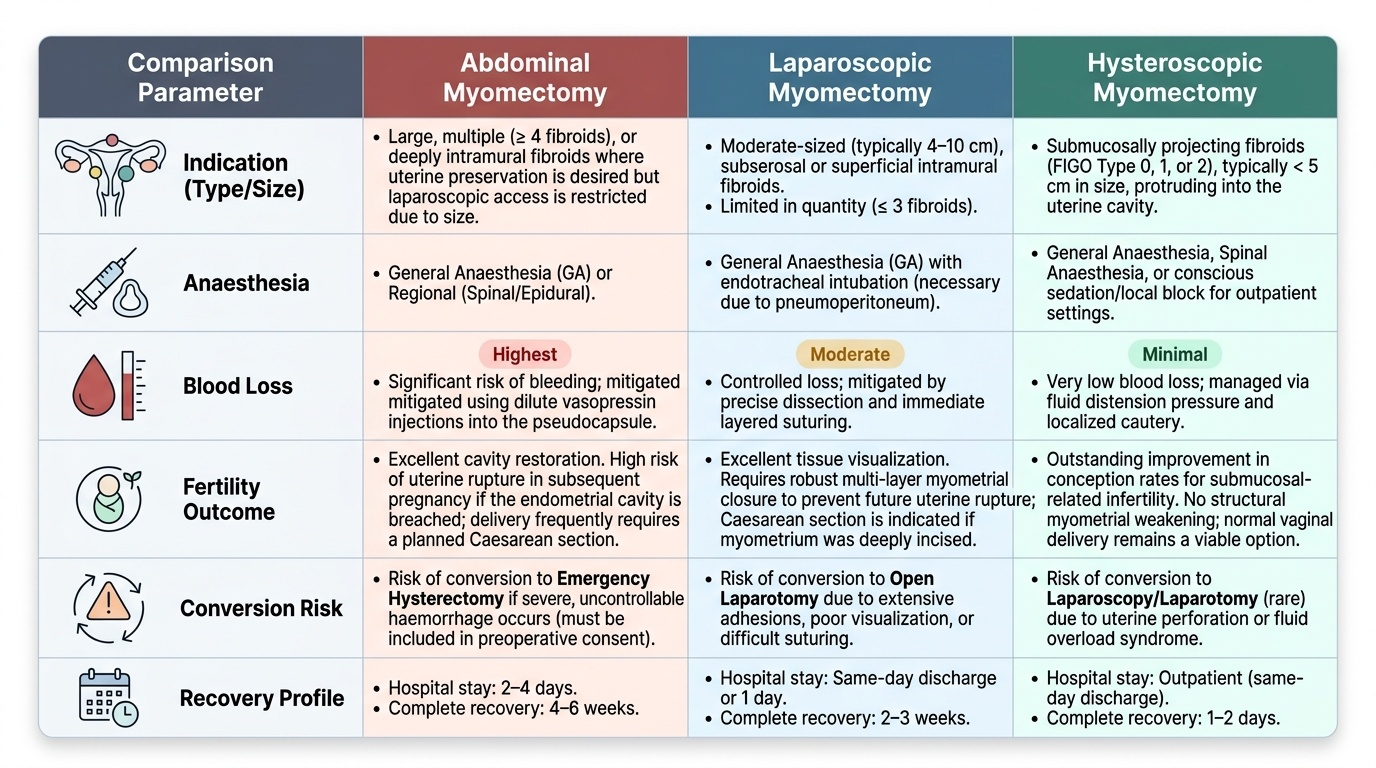
Abdominal myomectomy is performed when fibroids are too large, multiple, or deeply intramural for a laparoscopic approach. The key technical steps are: (1) dilute vasopressin injection into the pseudocapsule (vasoconstriction reduces blood loss by 30–40%); (2) incise the uterine serosa over the fibroid; (3) grasp the fibroid with a tenaculum or myoma screw and use the pseudocapsule as a surgical plane (blunt and sharp dissection within the capsule minimises myometrial damage); (4) close the myometrial defect in layers (multiple interrupted sutures, eliminating dead space to prevent haematoma); (5) close the uterine serosa. The most important intraoperative decision is whether to convert to hysterectomy if haemorrhage cannot be controlled — this must be discussed in the consent process. Postoperative complications specific to myomectomy include: haematoma in the myometrial wound, fever (from degenerating fibroid remnants), and — of most concern for future pregnancies — uterine rupture in a subsequent pregnancy (particularly if the endometrial cavity was entered). Patients must be counselled that delivery after myomectomy may need to be by caesarean section.
Ovarian surgery: the choice between ovarian cystectomy (remove cyst, preserve ovary) and salpingo-oophorectomy (remove ovary + tube) depends on age, suspected histology, and whether the ovary is salvageable. For a presumed benign cyst in a premenopausal woman, cystectomy within the capsule is preferred to preserve ovarian function. For postmenopausal women, a suspicious or indeterminate mass, or for cancer staging, salpingo-oophorectomy is performed. The infundibulopelvic ligament is the key vascular pedicle — the ureter must be identified before it is clamped.
Staging laparotomy for suspected ovarian malignancy follows the systematic protocol described in og16-ovarian-cancer: midline incision, peritoneal washings, systematic inspection, TAH+BSO, omentectomy, lymph node dissection, and random peritoneal biopsies. The surgical goal (optimal cytoreduction, residual disease <1 cm) is the primary survival determinant in advanced ovarian cancer.
Provided image
Vaginal Hysterectomy and Pelvic Floor Repair
Vaginal hysterectomy (VH) combined with pelvic floor repair is the standard surgical treatment for symptomatic uterovaginal prolapse. The vaginal approach differs fundamentally from the abdominal approach in that the surgeon works from below rather than from above, accessing the same ligamentous pedicles — uterosacral, cardinal, uterine artery — but from the vaginal vault rather than from the open peritoneal cavity. Its advantages over the abdominal route are significant: no abdominal incision (faster recovery, less post-operative pain, shorter hospital stay), direct access to the prolapsed vaginal structures that need repair, and the ability to address cystocoele and rectocoele in the same operative field without repositioning the patient. The appropriate selection criteria for VH are: a uterus that is small and mobile (typically ≤12 weeks' gestational size and well descended into the vaginal canal), adequate vaginal access (a nulliparous vagina may be too narrow for safe delivery of the uterus), and no indication for abdominal exploration (e.g., adnexal mass, endometriosis requiring peritoneal access, or suspected malignancy).
The steps of vaginal hysterectomy are, in sequence:
1. Patient position: dorsal lithotomy with steep Trendelenburg if needed
2. Circumferential cervical incision: the vaginal epithelium is incised circumferentially around the cervix, creating anterior and posterior vaginal flaps
3. Anterior entry (vesicouterine pouch): the bladder is mobilised anteriorly by entering the potential space between the bladder and anterior lower uterine segment — this is the most critical step to avoid cystotomy
4. Posterior entry (Pouch of Douglas/recto-uterine pouch): the peritoneum of the recto-uterine pouch is entered posteriorly, providing access to the peritoneal cavity and the uterosacral ligaments
5. Pedicle ligation: uterosacral → cardinal → uterine artery → broad ligament/round ligament pedicles, clamped from below; the specimen (uterus + cervix) is delivered through the vagina
6. Vault closure: the vaginal vault is closed, incorporating the uterosacral ligaments to prevent post-hysterectomy vault prolapse
Anterior colporrhaphy (repair of cystocoele — anterior vaginal wall descent with bladder): the anterior vaginal wall is opened, the paravaginal fascial defect is identified and plicated (fascial repair), and the vaginal wall is closed with interrupted sutures, reducing the cystocoele. A catheter remains for 24–48 hours post-operatively.
Posterior colporrhaphy (repair of rectocoele — posterior vaginal wall descent with rectum): the posterior vaginal wall is opened, the rectal bulge is reduced by plicating the levator ani muscles in the midline, and the vaginal wall is closed. Wound infection and pain are the main early complications.
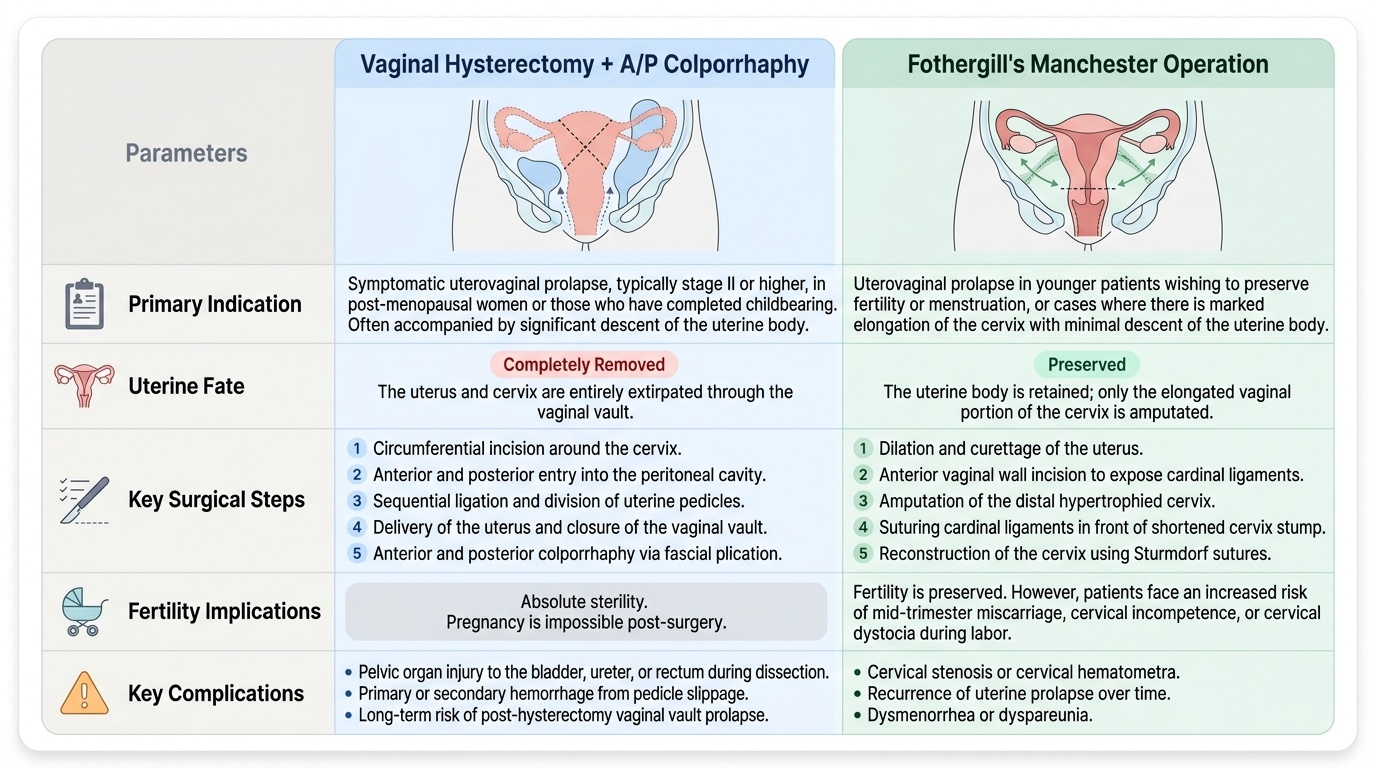
Fothergill's (Manchester) operation: specifically designed for cervical elongation with moderate prolapse when the patient wishes to retain her uterus. Steps: (1) anterior colporrhaphy; (2) amputation of the elongated cervix (Sturmdorf sutures to cover the cervical stump with vaginal epithelium); (3) the divided cardinal ligaments are sutured in front of the cervical stump, elevating the uterus and shortening the elongated supports. The uterus is preserved, which is advantageous for women desiring future pregnancy — though subsequent deliveries must be by caesarean section (weakened cervix) and miscarriage risk is increased from cervical incompetence.
Provided image
SELF-CHECK
A 65-year-old woman undergoes vaginal hysterectomy and anterior colporrhaphy for second-degree uterovaginal prolapse. On post-operative day 1, she cannot void and a bladder ultrasound shows 600 mL residual urine. What is the most likely cause and management?
A. Ureteric injury from the anterior dissection — requires urgent cystoscopy
B. Urinary retention due to post-operative oedema, pain, and disruption of bladder neck anatomy — manage with catheterisation and time
C. Bladder laceration during anterior colporrhaphy — requires surgical repair
D. Normal post-operative finding; no intervention needed
Reveal Answer
Answer: B. Urinary retention due to post-operative oedema, pain, and disruption of bladder neck anatomy — manage with catheterisation and time
Post-operative urinary retention is the most common urological complication after vaginal hysterectomy and anterior colporrhaphy, occurring in 5–15% of cases. It results from local oedema, pain-related voiding inhibition, and disruption of the bladder neck anatomy during the cystocele repair. Management is temporary urethral or suprapubic catheterisation — usually self-resolves within days to weeks. Ureteric injury would present with loin pain and raised creatinine; bladder laceration would have been noted intraoperatively; 600 mL painless retention is not 'normal'.
Laparoscopy and Hysteroscopy — Technique and Monitoring
Laparoscopy and hysteroscopy are endoscopic approaches that provide direct visualisation of the peritoneal cavity and uterine cavity respectively. Both require specialised distension media to create the operative field, and both carry unique complications distinct from open surgery. As a student, understanding the basic technique and the real-time monitoring parameters distinguishes active learning in theatre from passive observation.
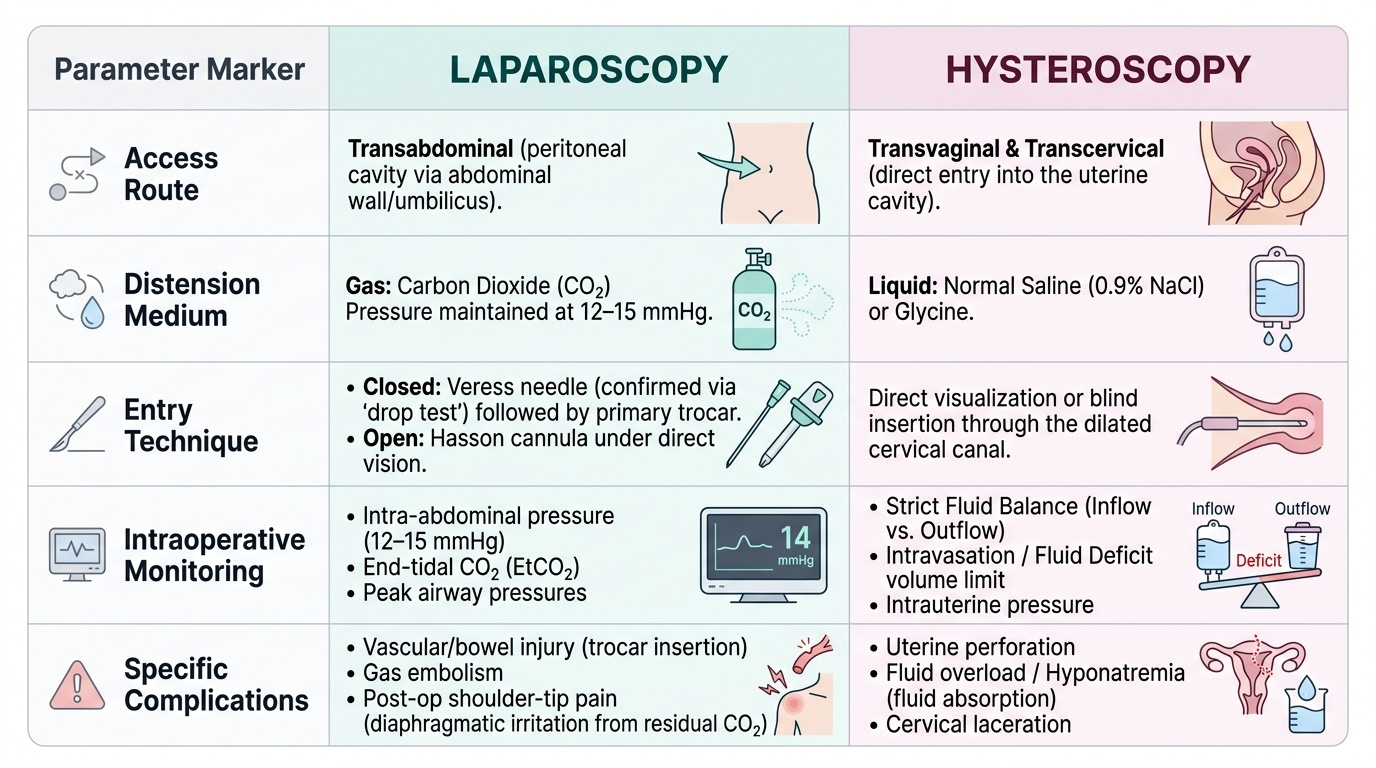
Diagnostic and operative laparoscopy involves creating a pneumoperitoneum (gas-filled space in the peritoneal cavity for visual access and instrument manipulation). The standard approach: (1) Veress needle insertion at the umbilicus (or left upper quadrant Palmer's point if prior abdominal surgery) — confirmed by the 'drop test' (saline drops when the needle tip is intraperitoneal) and aspiration check (no blood or bowel content); (2) CO₂ insufflation to a pressure of 12–15 mmHg; (3) primary trocar (5 or 10 mm) at the umbilicus; (4) secondary trocars placed under direct vision in the lower quadrants; (5) systematic inspection: uterus, tubes, ovaries, appendix, bowel, and diaphragm surface. Open (Hasson) entry is used when Veress needle entry is unsafe (prior surgery, adhesions, suspected bowel overlying umbilicus). Complications specific to laparoscopy: vascular injury (major vessel injury from trocar — rare but immediately life-threatening), bowel injury (often recognised post-operatively), gas embolism, port-site hernia, and post-operative shoulder-tip pain from diaphragmatic irritation by residual CO₂.
Hysteroscopy requires distension of the uterine cavity with a clear medium to allow visualisation. Two types of media are used: CO₂ (for diagnostic hysteroscopy — excellent visualisation but not suitable for operative work or bleeding); normal saline (isotonic, used for operative hysteroscopy). The critical safety parameter in operative hysteroscopy is fluid deficit monitoring — the difference between irrigating fluid inflow and outflow. When using normal saline, a deficit of 1,000 mL is the threshold to stop the procedure (risk of fluid overload and pulmonary oedema); with hypotonic media (glycine, sorbitol), the threshold is 750 mL (risk of dilutional hyponatraemia which can cause cerebral oedema and fatal neurological complications). The scrub nurse or operating theatre assistant must continuously monitor and announce the fluid deficit throughout operative hysteroscopy — the surgeon must respond to approaching thresholds by completing or abandoning the procedure.
Provided image
SELF-CHECK
During hysteroscopic transcervical resection of the endometrium (TCRE) with glycine distension medium, the cumulative fluid deficit reaches 800 mL with 40% of the procedure remaining. The patient is under spinal anaesthesia and begins to complain of a headache and neck stiffness. What is the immediate action?
A. Continue the procedure — the deficit has not exceeded 1,000 mL
B. Administer IV frusemide and continue if deficit stays below 1,000 mL
C. Stop the procedure immediately; check serum sodium; manage hyponatraemia
D. Switch to normal saline irrigation and continue
Reveal Answer
Answer: C. Stop the procedure immediately; check serum sodium; manage hyponatraemia
With hypotonic distension media (glycine, sorbitol), the safe fluid deficit threshold is 750 mL — the 800 mL deficit has already exceeded this. Headache and neck stiffness in an awake patient suggest early cerebral oedema from dilutional hyponatraemia (water intoxication), which is an emergency. The procedure must be stopped immediately. Serum sodium is checked urgently — hyponatraemia below 125 mEq/L requires careful correction with hypertonic saline (avoid rapid correction — risks central pontine myelinolysis). Continuing the procedure or simply giving frusemide without stopping risks fatal neurological injury.