Page 30 of 37
OG34.5 | Major Operative Gynaecology — SDL Guide (Part 3)
Interpretation of Intraoperative Findings
Intraoperative findings often differ from what was anticipated on preoperative imaging, and the surgeon must make real-time decisions in response to unexpected findings. As a student observing in theatre, recognising these findings and understanding their implications deepens the educational value of each case far beyond a technical demonstration.
Unexpected pelvic adhesions: Dense adhesions — typically from endometriosis, previous PID, or prior surgery — can obliterate the normal tissue planes, obscure the ureter and bowel, and significantly increase the complexity and risk of the procedure. The surgeon may need to perform adhesiolysis before identifying the uterus and its ligaments. Bowel involvement requires a colorectal surgeon's participation. The cardinal rule: if a structure cannot be clearly identified, it cannot be safely divided — identify before you cut.
Unexpected adnexal/peritoneal pathology: An incidental ovarian mass at laparotomy for benign disease changes the operative plan — frozen section (intraoperative histology) may be requested to determine whether the mass is benign (proceed with cystectomy) or malignant (convert to staging laparotomy). Peritoneal deposits or miliary seedlings on the bowel or omentum suggest an occult malignancy — biopsy and staging must take priority. If the preoperative consent did not include BSO and peritoneal disease is found, the surgeon must balance the clinical imperative (complete cancer staging) against the consent obtained.
Macroscopic assessment of the hysterectomy specimen: The surgeon examines the removed uterus on the back table. Fibroids are identifiable as white whorled nodules within the myometrium. Endometriosis on the serosal surface appears as blue-black haemorrhagic deposits or white fibrotic plaques. In cancer surgery, the surgeon checks that the resection margins are macroscopically clear (no visible tumour at the vaginal cuff or parametrial margin). A bulky, irregular endometrial cavity (seen on sectioning the specimen) raises the possibility of endometrial carcinoma in a hysterectomy performed for presumed benign disease.
Ureteric identification: A key indicator of safe completion is visually confirming the ureter's course before closing the abdomen. If there is any doubt about ureteric integrity — an unusual dissection plane, a clamped pedicle that was difficult to separate from surrounding tissue — intraoperative cystoscopy with ureteric catheterisation or indigo carmine injection (confirming bilateral ureteral jets in the bladder) should be performed before closure.
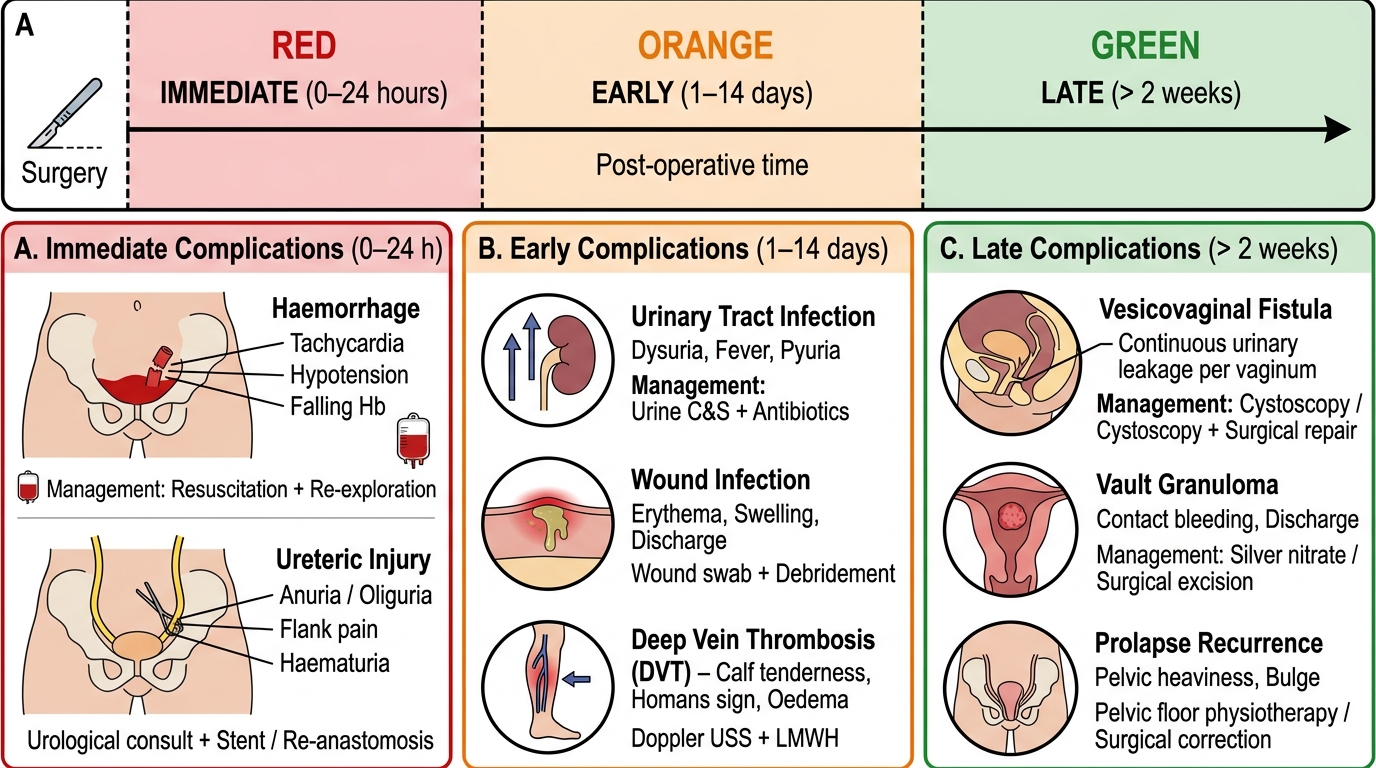
Post-Operative Complications Timeline: Major Gynaecological Surgery
Post-Operative Complications and Management
Post-operative complications after major gynaecological surgery span three time domains — immediate (intraoperative to 24 hours), early (days 1–14), and late (weeks to months) — and recognising the clinical features of each complication at the bedside allows timely escalation.
Immediate complications:
Haemorrhage: Primary haemorrhage from a slipped ligature or pedicle — presents with falling haemoglobin, tachycardia, hypotension, and pelvic pain. Management: early return to theatre for re-exploration if haemodynamically unstable. Reactive (secondary) haemorrhage at 7–10 days is usually from infection at the vault or a pedicle.
Ureteric injury: The most common serious complication of hysterectomy. Ligation presents post-operatively (day 1–5) with loin pain, fever, and raised creatinine. Transection may manifest as urinary leakage from the vault (ureterovaginal fistula) — watery vaginal discharge starting day 5–14. Diagnosis: CT urogram; management by urology (stenting vs surgical repair). Prevention: always identify the ureter before clamping pedicles; use intraoperative cystoscopy in difficult cases.
Bladder injury (cystotomy): Usually recognised intraoperatively (urine in the operative field, bladder catheter visible in wound). If recognised, immediate repair in two layers; catheterisation for 7–14 days. Missed cystotomy presents as vesicovaginal fistula (constant urinary dribbling from the vagina) 7–14 days post-operatively.
Bowel injury: Most commonly from adhesiolysis or trocar entry at laparoscopy. May not be recognised intraoperatively. Presents with peritonitis, fever, and distension 2–5 days post-operatively. Requires urgent laparotomy.
Early complications:
Urinary tract infection (UTI): Most common early complication after hysterectomy (catheter-related); presents with dysuria, frequency, fever; treated with antibiotics per sensitivity. Early catheter removal reduces risk.
Wound infection: Subcutaneous wound infection presents days 4–7 with wound redness, swelling, purulent discharge; managed with wound opening, debridement, and antibiotics.
Vault haematoma/abscess: Collection in the vaginal vault post-hysterectomy; presents with fever, pelvic pain, and vault tenderness on examination. Small haematoma: conservative (antibiotics, NSAIDs). Large or infected collection: vault drainage per vaginam.
Deep vein thrombosis (DVT) / pulmonary embolism (PE): Life-threatening complication, especially after prolonged pelvic surgery (cancer). Prevention: LMWH + TED stockings (started 12 hours post-operatively); early mobilisation. DVT presents with calf swelling and pain; PE with dyspnoea, pleuritic chest pain, tachycardia. Confirmed by duplex ultrasound (DVT) or CTPA (PE); treated with anticoagulation.
Late complications:
Vesicovaginal fistula: Abnormal communication between the bladder and vaginal vault, usually from a missed bladder injury or ischaemic necrosis. Presents with continuous urinary dribbling from the vagina. Diagnosis: dye test (methylene blue in bladder, appears vaginally); cystoscopy. Treatment: surgical repair (delayed 6–12 weeks to allow inflammation to resolve).
Ureterovaginal fistula: From ureteric injury; presents with flank pain and urinary leakage per vaginum; managed by ureteroscopic stenting or surgical reimplantation.
Vault granuloma: Granulation tissue at the vaginal vault suture line — common benign complication presenting with post-coital bleeding or discharge weeks after hysterectomy; treated with silver nitrate cautery or suture removal in the outpatient clinic.
Pelvic organ prolapse recurrence: After pelvic floor repair, symptomatic recurrence of cystocoele or rectocoele occurs in 10–30% at 5 years; managed with repeat surgery or pessary.
CLINICAL PEARL
The ureter is the great danger in all pelvic surgery — 'if in doubt, cut out the doubt' means: when uncertain about a structure, trace it from an unambiguous landmark (e.g., identify the ureter at the pelvic brim where it is clearly visible crossing the iliac vessels) before clamping anything near it. The three surgical aphorisms for safe hysterectomy are: (1) 'Always identify the ureter before clamping the infundibulopelvic ligament' — the ureter lies immediately beneath it; (2) 'Hug the uterus' — keeping clamps close to the uterus keeps the ureter out of pedicles; (3) 'Open the bladder space first' — mobilise the bladder fully before approaching the vaginal cuff, or the bladder will be included in the vault pedicle. The most preventable post-operative complication of major gynaecological surgery is DVT/PE: all patients undergoing major pelvic surgery must receive pharmacological prophylaxis (LMWH) and mechanical compression — omitting this in a post-operative cancer patient represents a standard of care failure.
Applied and Supervised Practice
The transition from student observer to surgical assistant is driven by structured observation — knowing what to look for at each stage of the operation, asking targeted questions, and building a mental model of the operative field that will guide future hands-on practice. The following observation frameworks are designed for use in theatre during major gynaecological procedures.
At TAH (abdominal hysterectomy): Before the case begins, ask to see the preoperative TVUS or MRI — identify the uterine size, fibroid locations, and adnexal findings that will influence the operative plan. In theatre, watch the EUA (examination under anaesthesia) — confirm whether the uterus is anteverted or retroverted and how this changes the operative approach. When the surgeon reflects the bladder, note the tissue plane — ask why they are using blunt versus sharp dissection in different areas. Watch the uterine artery pedicle being secured — identify the ureter crossing beneath (if visible) and note the clamp placement close to the uterus. After removal, look at the specimen on the back table: identify the fundus, the fallopian tubes, the round ligaments, and the endocervix.
At vaginal hysterectomy + pelvic floor repair: Note the difference in patient positioning (lithotomy vs supine). Observe the anterior vaginal dissection — ask the surgeon how they know when they are in the correct plane between the bladder and cervix. Watch the delivery of the uterus through the vaginal vault. During the colporrhaphy, watch the fascial plication technique and ask how much tissue tension is appropriate — too tight causes urinary obstruction; too loose fails to correct the prolapse.
At laparoscopy: Watch the Veress needle insertion and the drop test. Note the insufflation pressure (12–15 mmHg); ask what happens if it exceeds 20 mmHg. Observe the systematic peritoneal inspection — confirm that the surgeon checks the appendix and upper abdomen. If an unexpected finding (adhesion, endometrioma) is encountered, ask the surgeon what options were discussed in the consent process.
Post-operative ward round: When reviewing post-hysterectomy patients, specifically assess: (1) urine output (oliguria = ureteric injury or haemorrhage); (2) haemoglobin (if low or falling = haemorrhage); (3) temperature curve (early fever = atelectasis; day 5–7 = wound or vault infection); (4) calf tenderness and leg swelling (DVT screen); (5) vaginal discharge character (fresh blood = reactive haemorrhage; watery = possible fistula).