Page 24 of 37
OG34.4 | Minor Operative Gynaecology — SDL Guide
Learning Objectives
- State the clinical indications for Dilatation and Curettage (D&C), endometrial aspiration (EA), endocervical curettage (ECC), and cervical biopsy
- Describe the anatomical principles that govern safe instrument passage through the cervical canal into the uterine cavity
- Outline the step-by-step technique of D&C including anaesthesia, cervical dilatation, and curettage
- Describe outpatient endometrial aspiration (Pipelle/Vabra) and colposcopy-directed cervical punch biopsy techniques
- Explain the principle of fractional curettage (ECC first, then endometrial) for distinguishing cervical from endometrial disease
- Identify the immediate, early, and late complications of these procedures and their management
- Describe what to observe in theatre during supervised practice of minor gynaecological procedures
INSTRUCTIONS
Minor operative gynaecological procedures — D&C, endometrial aspiration, endocervical curettage, and cervical biopsy — are foundational diagnostic and therapeutic tools in gynaecology. They provide tissue diagnosis for abnormal uterine bleeding, postmenopausal bleeding, suspected endometrial or cervical pathology, and are essential steps in the management of gynaecological cancers and gestational trophoblastic disease. This module builds the knowledge and observational framework needed to assist at, understand, and eventually perform these procedures under supervision.
References
- DC Dutta's Textbook of Gynecology, 7th ed., Ch 34 — Operative Gynaecology: Minor Procedures (textbook)
- Shaw's Textbook of Gynaecology, 17th ed., Ch 34 — Gynaecological Procedures (textbook)
- RCOG Green-top Guideline No. 59 — Best Practice in Outpatient Hysteroscopy (2011) (guideline)
- TeLinde's Operative Gynecology, 12th ed., Ch 26 — D&C and Endometrial Sampling (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 52-year-old postmenopausal woman presents with a single episode of vaginal bleeding that occurred six weeks ago. Pelvic ultrasound shows an endometrial thickness of 9 mm (upper limit for postmenopausal endometrium without HRT is 4–5 mm). Her GP referred her to the gynaecology outpatient clinic under the two-week wait pathway. The gynaecologist performs a transvaginal ultrasound-guided Pipelle endometrial biopsy in the clinic — she tolerates it well and the result shows complex endometrial hyperplasia with atypia. She is booked for a formal D&C under general anaesthesia with hysteroscopy to further characterise the lesion. What is the D&C going to involve, what are the anatomical principles that make it safe, and what complications must the consenting doctor discuss with this patient?
WHY THIS MATTERS
Minor operative gynaecological procedures are among the most commonly performed surgical procedures in gynaecology worldwide. D&C remains a cornerstone diagnostic and therapeutic tool for a wide range of conditions — from abnormal uterine bleeding and postmenopausal bleeding to incomplete abortion, molar pregnancy, and endometrial polyp removal. As a final-year student on clinical rotations, you will witness these procedures in outpatient clinics and operating theatres, assist in theatre, and be expected to counsel patients about what to expect. Understanding the anatomical basis of safe instrument passage, the specific indications for each procedure variant, the expected findings on histopathology, and the complications to monitor post-operatively is essential both for clinical competence and for OSCE/viva assessments. Endometrial aspiration (Pipelle) is now increasingly performed as an outpatient procedure without anaesthesia, making it a skill you may perform relatively early in your career.
RECALL
Activate prior anatomical knowledge before proceeding. From your anatomy studies, recall the position of the non-pregnant uterus: typically anteverted and anteflexed in approximately 80% of women, retroverted in 20% — this determines the direction in which instruments are advanced through the cervical canal. Recall the layers of the uterine wall (endometrium, myometrium, perimetrium/serosa) and the endocervical canal lined by columnar epithelium, transitioning to the transformation zone at the squamocolumnar junction. Recall the internal os — the narrowest point of the cervical canal separating the cervical canal from the uterine cavity — which must be negotiated during cervical dilatation. From your understanding of cervical cancer management, recall that the transformation zone (TZ) is the target for colposcopic examination and directed biopsy, as most cervical intraepithelial neoplasia (CIN) arises here. From your knowledge of GTD (OG9.5), recall that suction evacuation — a variant of D&C technique — is the treatment of choice for molar pregnancy.
Clinical Indications and Relevance of Minor Gynaecological Procedures
The minor operative gynaecological procedures covered in this module — D&C, endometrial aspiration (EA), endocervical curettage (ECC), and cervical biopsy — each occupy a specific diagnostic or therapeutic role in a tiered system of uterine and cervical tissue diagnosis. The key clinical skill is choosing the right procedure for the right indication: an outpatient Pipelle biopsy is appropriate as the first-line investigation for postmenopausal bleeding in most women, while a formal D&C under general anaesthesia is reserved for cases where the outpatient procedure yields insufficient material, where a focal lesion (polyp, submucosal fibroid) needs direct visualisation with hysteroscopy, or where the patient cannot tolerate an outpatient procedure. Similarly, a cervical punch biopsy (performed at colposcopy without anaesthesia) serves a different purpose than an endocervical curettage (sampling the endocervical canal for staging purposes). Understanding these distinctions prevents both under-investigation — missing an endometrial carcinoma by accepting an inadequate Pipelle sample — and over-investigation — subjecting a patient to general anaesthesia when a 2-minute outpatient procedure would have answered the clinical question.
Dilatation and Curettage (D&C) is indicated for:
- Diagnostic: abnormal uterine bleeding (AUB) unresponsive to medical treatment, postmenopausal bleeding with thickened endometrium (>4 mm on TVUS), suspected endometrial polyp or fibroid, investigation for pyometra, staging prior to hysterectomy
- Therapeutic: incomplete or missed abortion (evacuation of retained products of conception — suction curettage preferred), hydatidiform mole (suction evacuation, also OG9.5), removal of endometrial polyp, haemostasis in dysfunctional uterine bleeding (temporary)
- Fractional curettage: when the relative contribution of endocervical vs endometrial disease needs to be distinguished (e.g. suspected stage II endometrial cancer with cervical extension, or combined CIN + AUB)
Endometrial Aspiration (EA) — using the Pipelle de Cornier, Vabra aspirator, or similar devices — is the outpatient, usually anaesthesia-free alternative to D&C for endometrial sampling. It is indicated for: postmenopausal bleeding, investigation of abnormal endometrium on ultrasound, follow-up of treated endometrial hyperplasia, and as a first-line investigation before committing to a D&C under anaesthesia. Its key advantage is that it can be performed in the outpatient or clinic setting without anaesthesia in most women. Its limitation is an inadequate sample rate of ~10–15% (particularly in post-menopausal women with atrophic endometrium or cervical stenosis) — an inadequate sample in a symptomatic woman mandates D&C.
Endocervical Curettage (ECC) is performed to sample the endocervical canal and is indicated: alongside colposcopy when the transformation zone is not fully visible (type 2 or 3 transformation zone), when there is discordance between cytology and colposcopy, or as part of fractional curettage for endometrial staging.
Cervical Biopsy is indicated for: colposcopic abnormalities (directed biopsy of the worst area of the TZ), punch biopsy of a visible cervical lesion, and large loop excision of the TZ (LLETZ, also called LEEP) as a combined diagnostic and therapeutic excision for CIN 2–3.
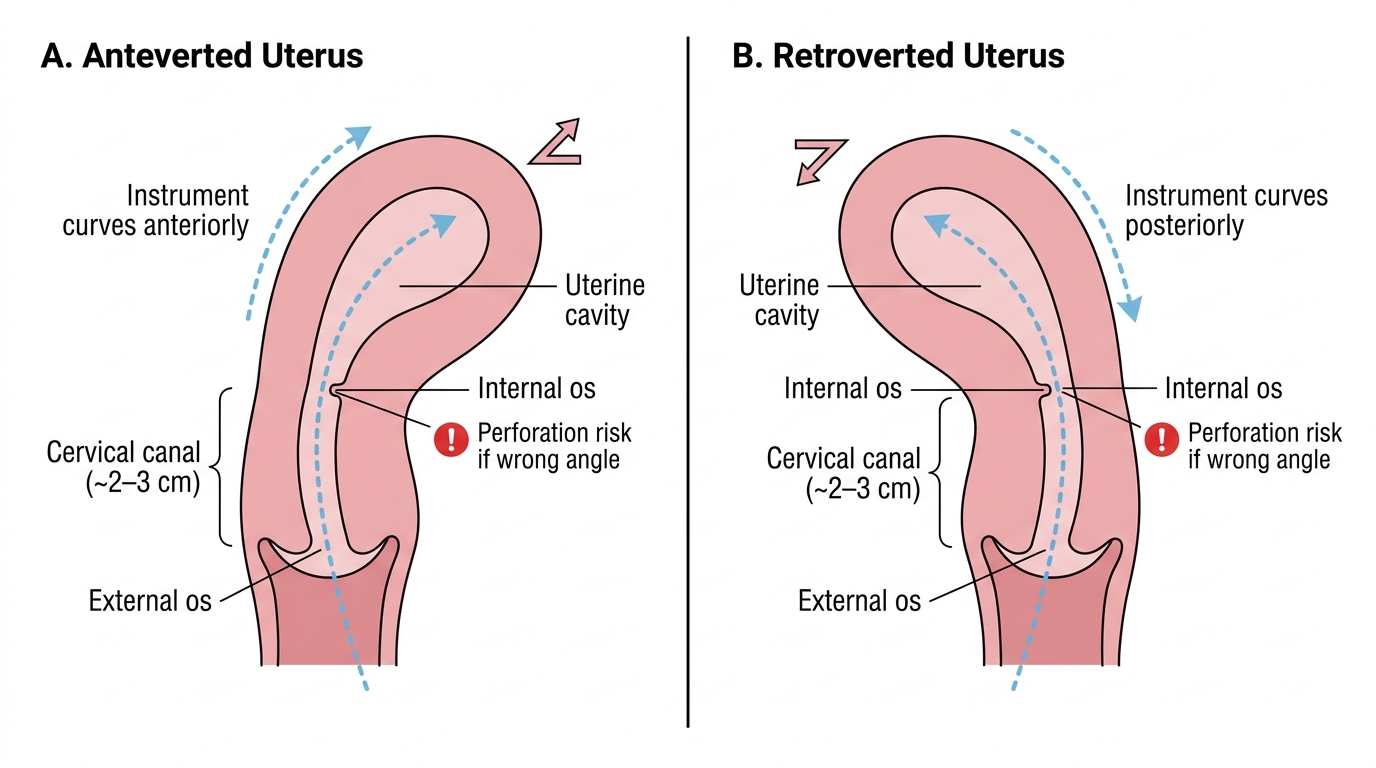
Uterine Position and Instrument Path in Anteverted vs Retroverted Uterus
Anatomy and Governing Principles
Safe passage of instruments through the cervix and into the uterine cavity depends on a precise understanding of the uterocervical anatomy and on a careful pre-operative bimanual examination to determine uterine size, position, and mobility. This pre-operative assessment is not a formality — it is the step that prevents uterine perforation, which is the most serious immediate complication of D&C.
The uterine position determines the angle of instrument entry. In an anteverted uterus (the majority), the uterine body is flexed anteriorly relative to the cervix, meaning instruments advanced through the cervical canal must curve anteriorly (upward) once the internal os is passed. In a retroverted uterus, the body lies posteriorly, and instruments must curve posteriorly. Using the wrong direction of approach creates a false passage and risks perforation at the internal os or lower uterine segment. Bimanual examination under anaesthesia (EUA) immediately before the procedure establishes the position definitively.
The cervical canal is approximately 2–3 cm long in the non-pregnant uterus, running from the external os (at the ectocervix) to the internal os (at the junction with the uterine cavity). The internal os is the anatomical narrowing that must be progressively dilated using Hegar dilators to allow passage of a curette. The canal is angled relative to the vagina, which is why the cervix is first steadied with a tenaculum (vulsellum forceps) applied to the anterior lip, straightening the cervicouterine junction and providing traction.
The uterine sound is the first instrument passed into the cavity, after securing the cervix with a tenaculum. The sound is a slender graduated probe that measures the length of the uterine cavity from the internal os to the fundus — typically 6–8 cm in a normal nulliparous uterus, up to 10 cm in a multiparous uterus. Confirming the direction, angle, and depth before inserting dilators is a fundamental safety step — resistance at the internal os guides the size of the first dilator to use. Sounding must be gentle; forcing the sound can perforate the fundus (thin and relatively avascular, the commonest perforation site).
Hegar dilators are graduated metal dilators (sizes 1–20, where the number approximately equals the diameter in mm). Cervical dilatation is performed sequentially, beginning with the smallest dilator that meets resistance and advancing by single sizes — never skipping sizes, which risks cervical laceration. For a D&C in a nulliparous woman, dilatation to Hegar 8–10 is usually sufficient to pass a medium curette.
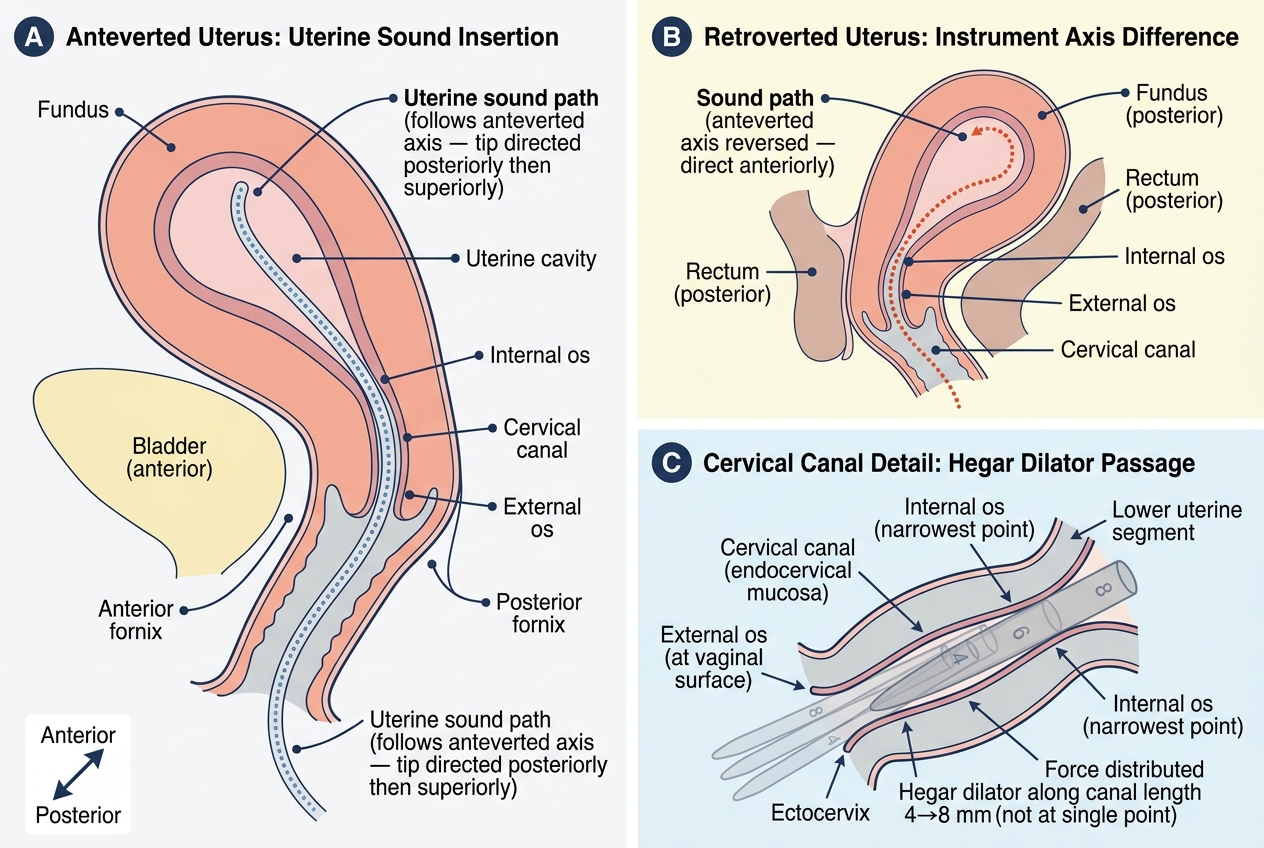
Uterine Axis, Cervical Landmarks, and Instrument Path in D&C
Dilatation and Curettage — Technique
The D&C procedure follows a logical, sequential technique that protects the patient from the procedure's main risks (perforation, haemorrhage, infection) while ensuring an adequate diagnostic or therapeutic result. It is performed in a theatre setting under general anaesthesia (or spinal/paracervical block), with the patient in the lithotomy position. Each step in the sequence has a specific safety rationale — the bimanual examination establishes uterine axis before any instrument is introduced; the tenaculum stabilises the cervix and straightens the cervicouterine angle; the sound confirms axis and depth before the wider dilators are advanced; and the sequential dilatation distributes force along the cervical canal rather than concentrating it at a single point. Learning the technique means learning not just the motor sequence but the reason why each step comes before the next. A doctor who skips the sound and dilates immediately has removed the primary safety check against perforation; a doctor who performs ECC after endometrial curettage has invalidated the localisation value of fractional curettage. These are not arbitrary rules — they are steps whose omission directly leads to preventable harm or missed diagnosis.
Pre-operative steps: (1) Informed consent including discussion of complications (see complications section); (2) Pelvic ultrasound to confirm uterine position and identify any structural pathology; (3) Antibiotic prophylaxis as indicated (especially post-abortion or if PID risk exists); (4) Misoprostol 400 µg vaginally 2–4 hours pre-operatively can be used to soften the cervix (particularly in nulliparous or postmenopausal women), reducing the force required for dilatation.
Procedure steps in sequence:
1. Lithotomy position; catheterise the bladder (or ask patient to void pre-operatively)
2. Bimanual examination under anaesthesia (EUA): confirm uterine size, position (ante vs retroverted), consistency, and mobility
3. Speculum insertion (Sims/bivalve); visualise the cervix; clean with antiseptic
4. Tenaculum (vulsellum) application: single-tooth or double-tooth forceps applied to the anterior cervical lip at 12 o'clock, providing downward traction to straighten the cervicouterine angle
5. Uterine sounding: the sound is gently introduced through the external os, negotiated through the internal os (following the uterine axis established by EUA), and advanced to the fundus. Record the cavity depth in cm.
6. Sequential cervical dilatation with Hegar dilators: starting at the size that meets gentle resistance; each dilator held for 10–15 seconds; advance by single sizes to the desired width (typically Hegar 8–10 for a diagnostic D&C)
7. Curettage: using a sharp curette (medium or large), systematic strokes are made from the fundus towards the internal os in all four quadrants (anterior, posterior, right, left walls). The curette should feel firm contact with the uterine wall; a grating sensation indicates the endometrium is being sampled. A soft, spongy sensation suggests completed curettage. Fractional curettage: if staged, perform ECC (endocervical) FIRST before dilatation — any subsequent material from dilatation would contaminate the endocervical sample.
8. Specimen collection: curettings collected in a labelled fixative container; submit for histopathology
9. Haemostasis check: inspect cavity (with hysteroscope if combined); uterine contraction reduces bleeding
10. Remove tenaculum; inspect cervix for lacerations; remove speculum
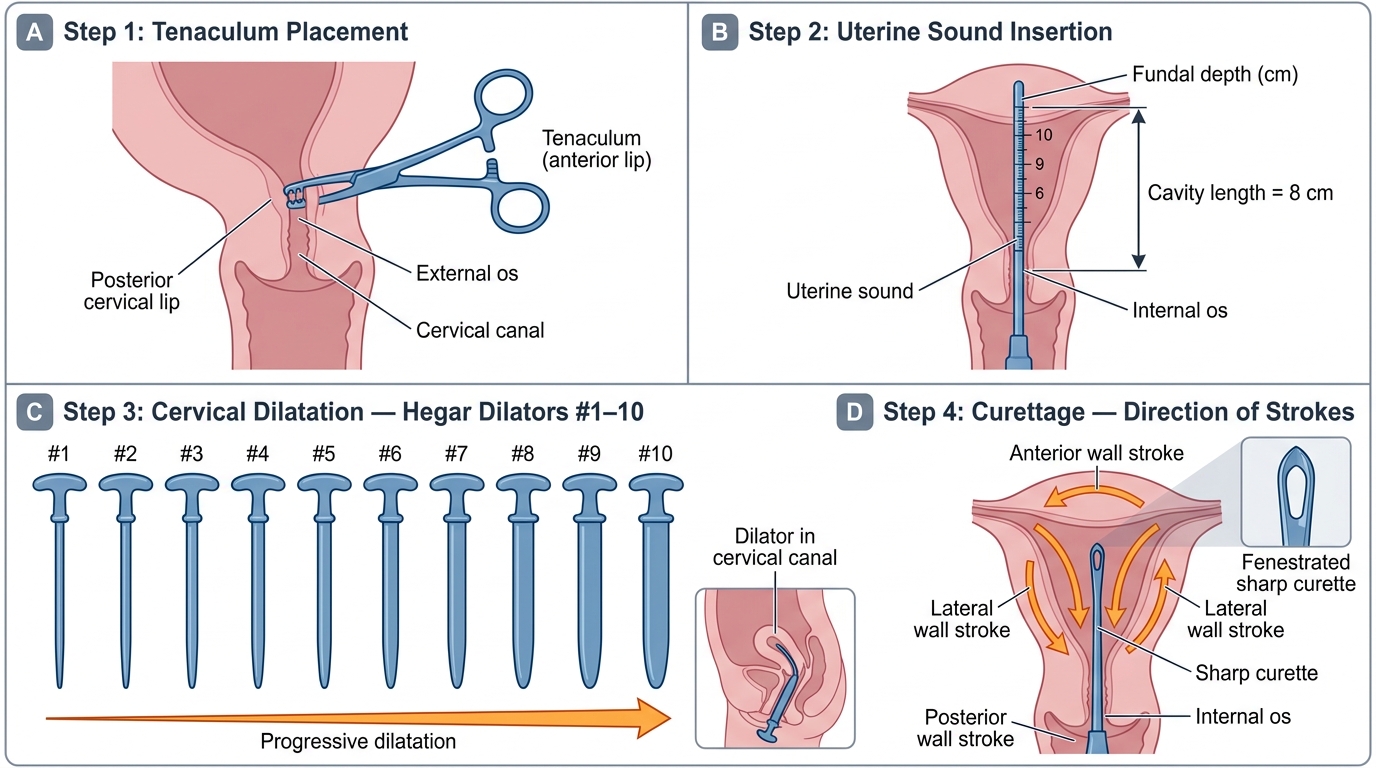
Steps of Dilatation and Curettage (D&C): Instrument Sequence and Technique