Page 25 of 37
OG34.4 | Minor Operative Gynaecology — SDL Guide (Part 2)
Endometrial Aspiration, ECC, and Cervical Biopsy — Technique
These procedures share the goal of obtaining tissue from the uterine cavity or cervix for histological diagnosis, but differ in setting (outpatient vs theatre), anaesthesia requirement, specimen adequacy, and diagnostic sensitivity. Understanding the technical nuances of each improves diagnostic yield and patient experience.
Endometrial aspiration (Pipelle technique): The Pipelle de Cornier is a flexible 3.1 mm outer diameter polypropylene sheath with a piston that creates suction when the inner rod is withdrawn. The technique is as follows: (1) visualise the cervix with a speculum; (2) no cervical dilatation is usually needed (the Pipelle is narrow enough to pass through the internal os in most women); (3) introduce the Pipelle gently through the external os and advance to the uterine fundus; (4) withdraw the inner piston to create negative pressure (suction); (5) rotate the Pipelle and move it in and out with strokes covering all four walls; (6) remove and expel contents into fixative. The entire procedure takes 1–2 minutes. Sensitivity for endometrial carcinoma: approximately 91% in studies (comparable to D&C for carcinoma detection; lower for polyps and focal hyperplasia). An inadequate sample (insufficient material for histology) in a symptomatic postmenopausal woman mandates hysteroscopy + directed biopsy.
Endocervical curettage (ECC): A small (Kevorkian or similar) curette is introduced into the endocervical canal without dilating the cervix (to avoid contamination from the uterine cavity). Systematic scraping of the canal walls yields an endocervical specimen. In fractional curettage, ECC is performed first and specimen labelled separately, THEN the endometrial curettage proceeds — preserving the integrity of endocervical sampling before dilatation.
Colposcopy-directed cervical punch biopsy: (1) Apply 3–5% acetic acid to the cervix; identify the transformation zone (TZ) and acetowhite areas; (2) Apply Lugol's iodine if needed (iodine-negative = Schiller positive = abnormal glycogen-poor epithelium); (3) Use a Kevorkian or similar punch biopsy forceps to take 3–5 mm tissue cylinder from the most abnormal area of the TZ; (4) Haemostasis with Monsel's solution (ferric subsulphate), silver nitrate, or pressure; (5) Label specimens separately if multiple sites biopsied. No anaesthesia is typically needed; the patient experiences brief sharp discomfort. The procedure is performed at colposcopy after an abnormal cervical smear.
| Sampling Method | Setting | Anaesthesia | Sensitivity for Carcinoma | Key Limitation |
|---|---|---|---|---|
| Pipelle aspiration | Outpatient | Usually none | ~91% | Inadequate rate ~10–15%; misses focal lesions |
| Vabra aspirator | Outpatient | Paracervical block | ~95% | More uncomfortable than Pipelle |
| D&C (blind) | Theatre | GA/spinal | ~80–85% | Misses focal lesions (polyps, focal Ca) |
| Hysteroscopy + biopsy | Theatre/OPD | Variable | >95% | Equipment-dependent; most accurate |
SELF-CHECK
A 58-year-old postmenopausal woman has postmenopausal bleeding. Outpatient Pipelle biopsy yields insufficient material. Transvaginal ultrasound shows endometrial thickness 7 mm. What is the most appropriate next step?
A. Reassure — Pipelle was negative so endometrial cancer is excluded
B. Repeat Pipelle biopsy in 3 months
C. Hysteroscopy with directed biopsy and/or D&C under anaesthesia
D. Start progestogen therapy empirically
Reveal Answer
Answer: C. Hysteroscopy with directed biopsy and/or D&C under anaesthesia
An insufficient Pipelle sample in a symptomatic postmenopausal woman with thickened endometrium does NOT exclude endometrial pathology — it simply means no diagnosis was possible. The standard next step is hysteroscopy (with direct visualisation and targeted biopsy) and/or D&C under anaesthesia to obtain an adequate sample. Reassuring the patient on the basis of an inadequate sample is a recognised cause of missed endometrial cancer. Empirical progestogen without diagnosis is inappropriate.
Interpretation of Findings
The clinical value of D&C, endometrial aspiration, ECC, and cervical biopsy lies in the histopathological findings they yield. The clinician ordering these procedures must understand the range of expected findings and their clinical implications, both to counsel patients pre-operatively and to action the results appropriately.
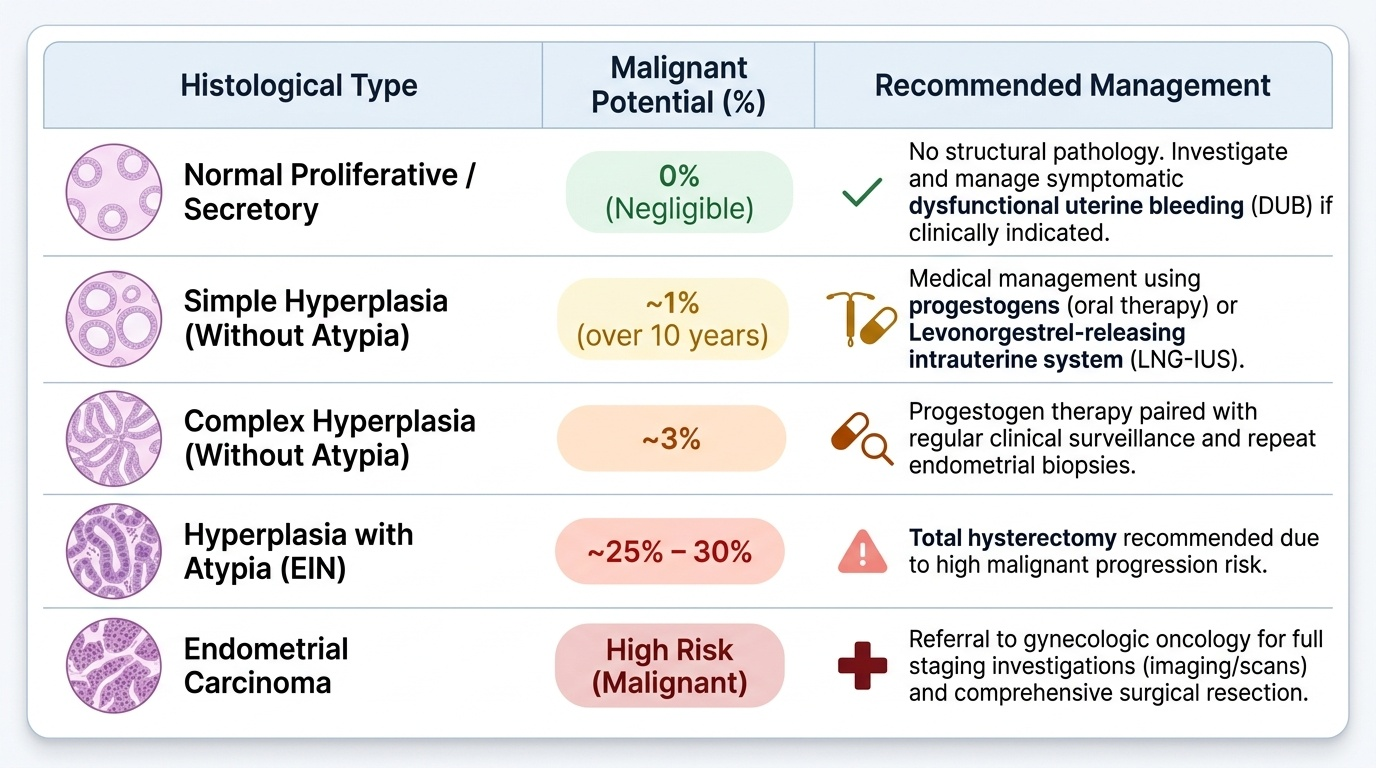
Endometrial histology (from D&C or EA): Normal proliferative or secretory endometrium indicates no structural pathology (though dysfunctional uterine bleeding can still occur). Endometrial polyp (irregular glandular overgrowth on a fibrovascular stalk): benign in most, but ~0.5% harbour carcinoma; usually requires hysteroscopic polypectomy. Simple hyperplasia without atypia: low malignant potential (~1% cancer risk over 10 years); managed with progestogens or LNG-IUS. Complex hyperplasia without atypia: ~3% cancer risk; progestogen treatment and surveillance. Simple/Complex hyperplasia WITH atypia (endometrial intraepithelial neoplasia): ~25–30% cancer risk; hysterectomy recommended. Endometrial carcinoma: requires full staging investigations and surgical management. Inadequate sample: cannot exclude pathology; proceed to hysteroscopy if clinically indicated. Atrophic endometrium: common in postmenopausal women; reassuring when the clinical presentation is low-risk, but does not exclude focal cancer.
Endocervical histology (from ECC): Normal endocervical epithelium. Endocervical glandular dysplasia (adenocarcinoma in situ, AIS): requires excision (cone biopsy/LLETZ) as it may extend into the canal beyond colposcopy's view. Cervical adenocarcinoma: less common than squamous but increasing in incidence; HPV-18 associated.
Cervical biopsy histology: Normal ectocervix or metaplastic TZ. CIN 1 (low-grade squamous intraepithelial lesion, LSIL): usually regresses spontaneously; surveillance colposcopy. CIN 2/3 (high-grade squamous intraepithelial lesion, HSIL): requires treatment (LLETZ excision). Squamous cell carcinoma: invasive cancer requiring staging and oncological management (OG34.1).
Inadequate cervical biopsy occurs when the biopsy misses the lesion (targeting error), samples too superficially (no stroma), or is too small. It requires repeat colposcopy and biopsy.
Provided image
Complications and Their Management
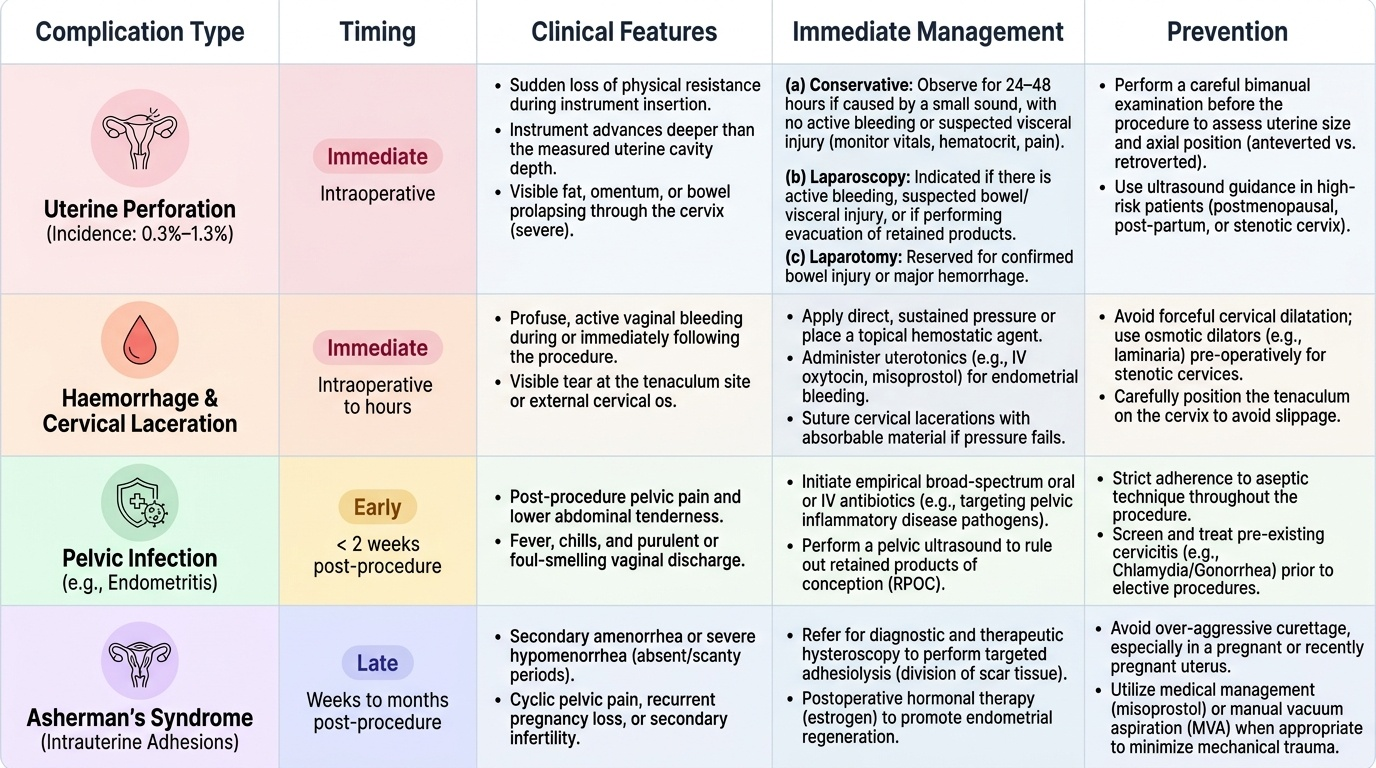
Complications of minor gynaecological procedures are uncommon but clinically important — the consenting doctor must discuss each with the patient before the procedure. Complications are classified as immediate (intraoperative or within hours), early (within 2 weeks), and late (weeks to months after the procedure).
Immediate complications:
Uterine perforation is the most serious immediate complication. Incidence: approximately 0.3–1.3% for D&C (higher in postmenopausal uterus, post-partum uterus, and when performed by inexperienced operators). The perforation is typically fundal (thin myometrium at the fundus) and often results from the uterine sound or the first dilator. Recognition: sudden loss of resistance with instrument advancing further than the measured cavity depth; instrument passes beyond the expected fundal limit. Management: (a) if the perforation is recognised with a small sound only, and there is no bleeding or suspicion of bowel injury — observe for 24–48 hours conservatively (vital signs, haematocrit, pain); (b) if there is bleeding, visceral injury suspected (bowel smell, omentum prolapsing through the perforation), or if the procedure was being done for evacuation of retained products — proceed to diagnostic laparoscopy to inspect the perforation and exclude bowel injury; (c) laparotomy is rarely needed but necessary for bowel injury or significant intraperitoneal haemorrhage.
Cervical laceration: from tenaculum slipping or forceful dilatation, especially in a stenotic cervix. Usually managed with direct pressure or a suture.
Haemorrhage: intraoperative bleeding from the endometrium or cervix; managed with uterotonics (oxytocin IV), gauze packing, or Foley balloon tamponade.
Anaesthetic complications: standard risks of GA/spinal.
Early complications:
Endometritis/pelvic infection: fever, uterine tenderness, purulent discharge within days to 2 weeks. Risk is higher in women with pre-existing PID, STI, or immunosuppression. Treated with broad-spectrum antibiotics (doxycycline + metronidazole, or cephalosporin + metronidazole). Antibiotic prophylaxis pre-D&C is recommended in high-risk patients.
Late complications:
Asherman syndrome (intrauterine adhesions/synechiae): the most clinically significant long-term complication. Results from overzealous curettage that strips the stratum basalis (regenerative layer) of the endometrium, especially when done in the post-partum or post-abortal period when the endometrium is soft and adherent. Clinical features: secondary amenorrhoea or hypomenorrhoea, cyclical pelvic pain (haematometra), and infertility. Risk is highest after postpartum D&C for retained placenta or missed/incomplete abortion (incidence up to 30% in some series). Diagnosed by hysteroscopy. Treatment: hysteroscopic adhesiolysis followed by oestrogen therapy and an intrauterine splint to prevent re-adhesion.
Cervical stenosis: a late complication of repeated D&Cs or traumatic dilatation, causing obstruction at the internal os; may result in haematometra (blood accumulating in the uterine cavity).
Provided image
SELF-CHECK
During a D&C for retained products of conception 10 days post-partum, the uterine sound advances to 12 cm (pre-procedure fundal height suggested the uterus was at 8 cm). There is a sudden loss of resistance. What has most likely occurred and what is the immediate next step?
A. The cavity is larger than expected; continue curettage
B. Uterine perforation has occurred; stop the procedure and arrange diagnostic laparoscopy
C. Uterine perforation has occurred; proceed immediately to laparotomy
D. The sound has passed through the fallopian tube; withdraw and try again
Reveal Answer
Answer: B. Uterine perforation has occurred; stop the procedure and arrange diagnostic laparoscopy
Sudden loss of resistance with the instrument advancing beyond the expected fundal depth is the classic sign of uterine perforation. The post-partum uterus is particularly at risk — soft, large, and with thin myometrium. The correct initial response is to stop the procedure immediately. Diagnostic laparoscopy is needed to inspect the perforation and exclude bowel injury (not immediate laparotomy, unless there is evidence of haemorrhage or visceral injury). The sound cannot pass through the fallopian tube — the tubal ostia are much too narrow.