Page 26 of 37
OG34.4 | Minor Operative Gynaecology — SDL Guide (Part 3)
Applied and Supervised Practice
As a final-year student observing and assisting at minor gynaecological procedures in theatre and outpatient clinics, there are specific items to look for at each stage of the procedure that will consolidate your theoretical understanding into clinical knowledge. Active observation — knowing what to look for and asking structured questions — is far more valuable than passive watching, and prepares you for the point at which you will perform these procedures under supervision.
In the outpatient clinic (Pipelle biopsy): Observe how the gynaecologist counsels the patient before the procedure — what information is provided about discomfort, duration, and what happens next. Watch the speculum insertion and tenaculum application (or whether a tenaculum is needed — in many post-menopausal women with a straightened cervix, it is not). Note whether misoprostol pre-treatment was given. Observe the Pipelle insertion and the patient's response; ask the clinician how they judged when they had reached the fundus. After the procedure, observe the specimen and how it is labelled.
In the operating theatre (D&C): Confirm you can identify the instruments laid out before the procedure: tenaculum, uterine sounds (and their graduation markings), Hegar dilators (ask the scrub nurse to show you sizes 1 through 10 in order), curettes (sharp vs blunt, different sizes), Sims and bivalve specula, Vabra or other suction devices. During the procedure: listen to the surgeon announce the uterine position from EUA and watch how this affects instrument direction. Observe the sound insertion — ask the surgeon what depth they measured. Count the dilators as they are used sequentially. Watch the curette technique and note the systematic approach (four walls, fundus to os). After curettage: look at the specimen — note its volume and colour (proliferative endometrium = scanty pale curetting; hyperplastic = bulky; carcinoma may have necrotic yellow/tan tissue). Ask the surgeon what they plan to do with the result.
Pre- and post-operative patient communication: Pre-operatively, the patient needs to understand: the purpose of the procedure, what anaesthesia will be used, that she will need someone to accompany her home if GA is used, and the possible complications (perforation 0.3–1.3%, infection, Asherman syndrome rare but important if she wishes future fertility). Post-operatively: she will experience mild cramping and light spotting for 1–2 days; she should report fever, heavy bleeding, or worsening pain; she will receive the histology result within 1–2 weeks and should have a follow-up appointment booked.
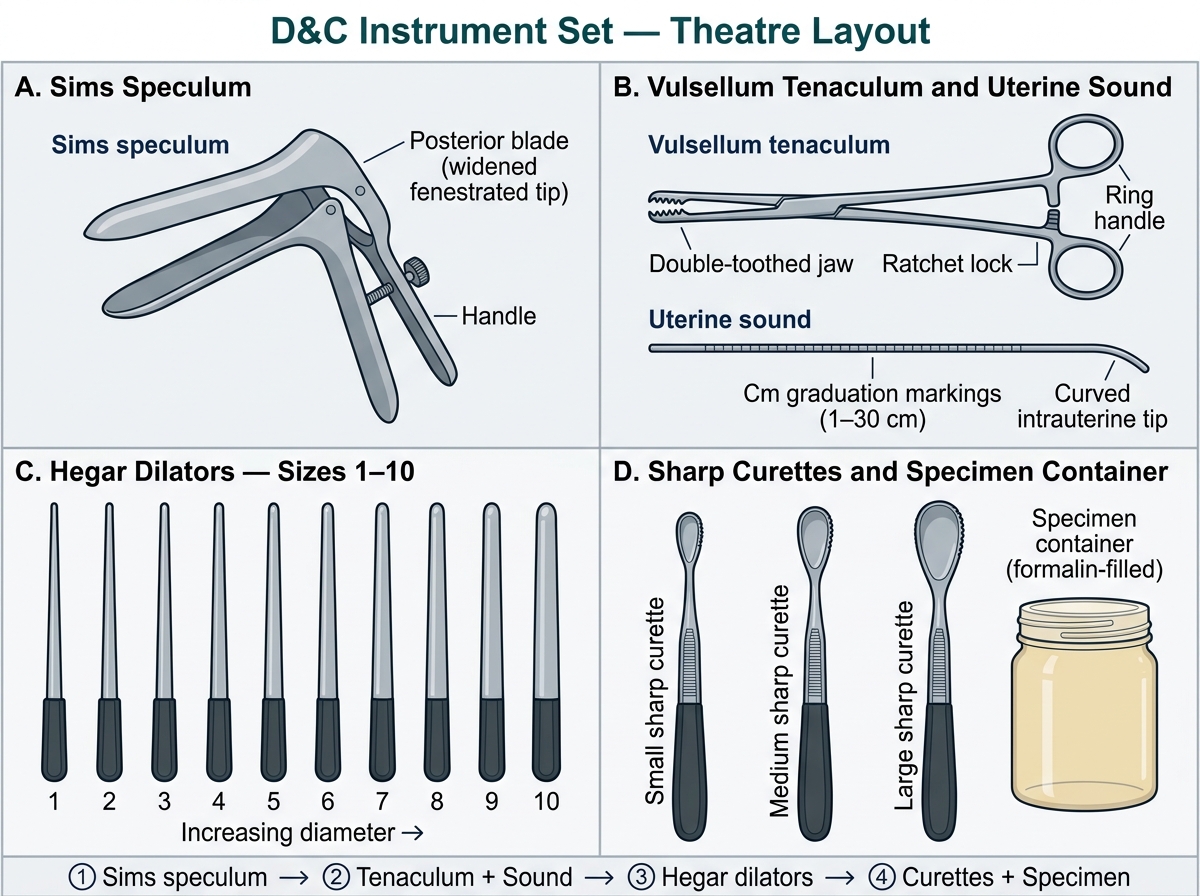
D&C Instrument Set — Standard Theatre Layout
Self-Assessment
Use the following prompts to test your understanding before reviewing the summary. Work through each question independently before checking the summary.
Indication matching: For each clinical scenario, identify the most appropriate procedure — (a) 45-year-old with menorrhagia, TVUS showing 12 mm endometrium, previous failed Pipelle (insufficient sample); (b) 30-year-old with abnormal smear (high-grade dyskaryosis), colposcopy showing dense acetowhite area at the TZ; (c) 28-year-old with 10-week missed abortion; (d) 50-year-old with postmenopausal bleeding, 5 mm endometrium, no previous investigations.
Answers: (a) D&C with hysteroscopy under GA (prior insufficient Pipelle + thickened endometrium); (b) colposcopy-directed punch biopsy ± LLETZ; (c) suction curettage (surgical management of missed abortion — D&C variant); (d) outpatient Pipelle endometrial aspiration is appropriate first step (thin endometrium in a symptomatic woman — still requires histological exclusion of carcinoma, but outpatient sampling is appropriate first-line).
Complication scenario: A woman calls the clinic 5 days after D&C for abnormal uterine bleeding, reporting fever of 38.5°C and worsening pelvic pain. What is the diagnosis and management? — Diagnosis: post-operative endometritis. Management: examination to exclude pelvic abscess; broad-spectrum antibiotics (doxycycline + metronidazole or cephalosporin + metronidazole); if unresponsive, USS to exclude haematometra or abscess; hospital admission if systemically unwell.
Consent point: Why must a patient who wishes future fertility be specifically counselled about Asherman syndrome before a post-partum D&C? Because postpartum D&C (for retained products) carries the highest risk of Asherman syndrome (up to 30% in some series), since the post-partum endometrium is soft and adherent — curettage strips the basalis layer and leads to intrauterine adhesions causing infertility and secondary amenorrhoea. The patient must understand this risk and discuss whether alternatives (expectant or medical management of retained products) are appropriate.
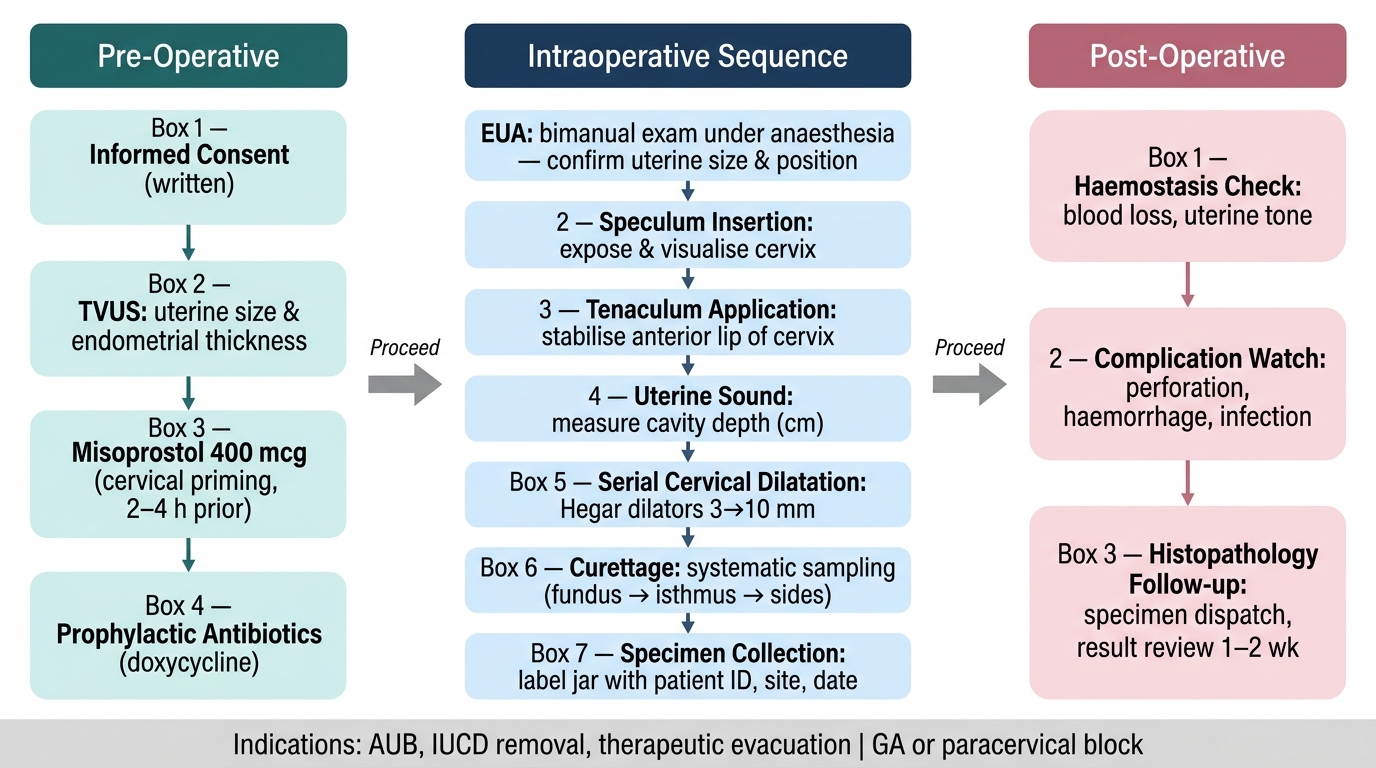
D&C Procedure Checklist: Pre-operative, Intraoperative, and Post-operative Steps
CLINICAL PEARL
Two safety rules that prevent the most serious complications of D&C: (1) Always sound the uterus before dilating — the sound confirms uterine axis, direction, and depth; attempting to dilate a retroverted uterus as if it were anteverted is the most common mechanism of perforation at the internal os. (2) Perform ECC before dilatation in fractional curettage — once the cervix is dilated, endometrial curettings inevitably contaminate the endocervical canal, invalidating the ECC specimen. The order (ECC → dilatation → endometrial curettage) must be strict. Additionally: Asherman syndrome is largely a preventable iatrogenic complication — it results from curettage of a postpartum or post-abortal uterus beyond what is clinically necessary. When evacuation of retained products is the indication, suction curettage (gentler on the endometrium) is preferred over sharp curettage, and the procedure should stop as soon as gritty resistance confirms complete evacuation — not continued until the cavity 'feels empty'.
SELF-CHECK
During a fractional curettage for a patient with postmenopausal bleeding and suspected endometrial carcinoma, the surgeon performs endometrial curettage first and then plans to do ECC. What is the consequence of this order, and why does it matter?
A. No consequence — the cervical and uterine specimens will still be useful
B. The ECC specimen will be contaminated by endometrial cells from the dilated canal, invalidating localisation of disease to the cervix
C. The uterine specimen will be contaminated by endocervical cells
D. The procedure order does not matter as long as both specimens are sent
Reveal Answer
Answer: B. The ECC specimen will be contaminated by endometrial cells from the dilated canal, invalidating localisation of disease to the cervix
Fractional curettage is performed specifically to determine whether disease (e.g. carcinoma) is localised to the endometrium (Stage I) or extends to the endocervix (Stage II endometrial cancer). If the cervix is dilated before ECC, endometrial curettings wash into the cervical canal, making ECC histology uninterpretable — you cannot tell whether endometrial cells in the canal are from true endocervical disease or from contamination. The correct order is: ECC first (before any dilatation), then dilatation, then endometrial curettage.