Page 16 of 37
OG34.2 | Ovarian Cancer — SDL Guide
Learning Objectives
- Describe the aetiology and risk factors for ovarian cancer including genetic predisposition (BRCA1/2)
- Classify ovarian tumours by histological origin: epithelial, germ cell, and sex-cord stromal types
- Apply the FIGO 2014 staging system accurately to ovarian cancer (distinguishing it from cervical and endometrial staging)
- Select appropriate investigations and interpret tumour markers (CA-125, AFP, β-hCG, LDH) for specific histotypes
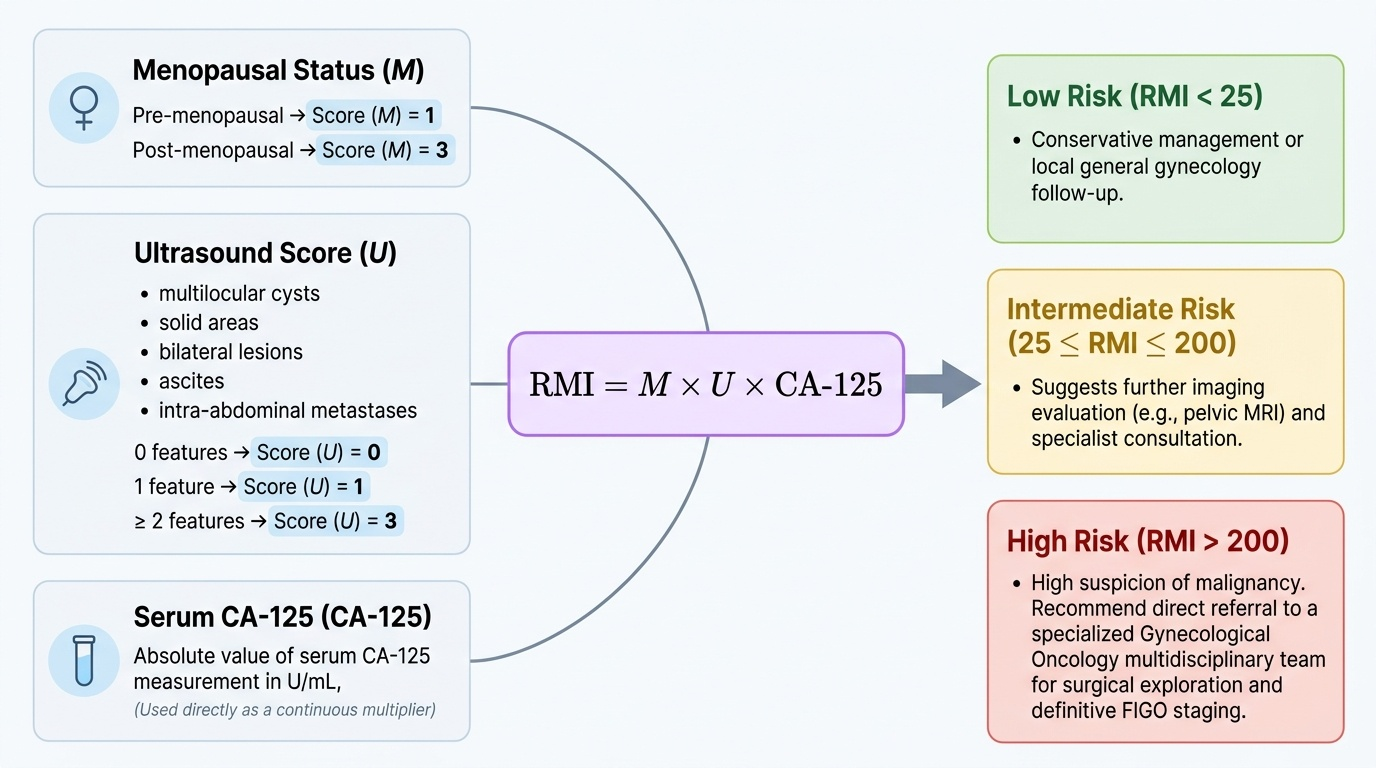
- Calculate and apply the Risk of Malignancy Index (RMI) for triaging adnexal masses
- Outline the principles of staging laparotomy and cytoreductive surgery for ovarian cancer
- Describe first-line chemotherapy regimens and maintenance therapy (including PARP inhibitors for BRCA-mutated disease)
- Discuss prognosis by stage and surveillance strategies post-treatment
INSTRUCTIONS
Ovarian cancer is the most lethal gynaecological malignancy — its insidious onset, nonspecific symptoms, and lack of effective screening mean that over 70% of cases are diagnosed at advanced stage. This module will take you from the biology of the 'silent killer' through classification, staging, investigation, and management, building your ability to think systematically about an adnexal mass and manage a patient with ovarian cancer from diagnosis through treatment.
References
- DC Dutta's Textbook of Gynecology, 7th ed., Ch 30 — Malignant Tumours of the Ovary (textbook)
- Shaw's Textbook of Gynaecology, 17th ed., Ch 29 — Ovarian Tumours (textbook)
- FIGO Staging Classification for Cancer of the Ovary, Fallopian Tube, and Peritoneum, 2014 (guideline)
- FOGSI Good Clinical Practice Recommendation — Ovarian Cancer Management (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 54-year-old postmenopausal woman presents to the gynaecology outpatient clinic with a 3-month history of gradually increasing abdominal girth, early satiety, and vague lower abdominal discomfort. She initially attributed the bloating to weight gain. On examination, there is a large irregular mass arising from the pelvis, shifting dullness on percussion, and mild bilateral leg oedema. Ultrasound shows a complex bilateral adnexal mass with solid components, internal septations, and a moderate volume of free fluid. Her CA-125 is 890 U/mL. Her sister was diagnosed with breast cancer at age 42. The surgical team discusses proceeding to staging laparotomy. What has happened inside this woman's abdomen over the past several months — and what should guide the surgical plan?
WHY THIS MATTERS
Ovarian cancer accounts for approximately 3–4% of all female cancers globally, yet it is the most lethal gynaecological malignancy because early disease is almost entirely asymptomatic and no effective population-based screening programme exists. In India, ovarian cancer is the second most common gynaecological malignancy after cervical cancer (ICMR data). The five-year survival rate for Stage I disease exceeds 90% — but only about 20–30% of cases are detected at this early stage. The vast majority present at Stage III or IV, where five-year survival drops to 20–30%. As a final-year student you will encounter adnexal masses in outpatient clinics, emergency presentations with torsion or rupture, and post-operative surveillance patients. Understanding the biology, staging, and management framework is essential — surgical staging determines both prognosis and whether adjuvant chemotherapy is needed.
RECALL
Before proceeding, connect this topic to prior learning. From your anatomy studies, recall the blood supply of the ovary (ovarian artery from the aorta, with anastomosis from the uterine artery) and the lymphatic drainage to para-aortic nodes — critical for understanding staging and surgical nodal dissection. From physiology, recall the hormonal functions of granulosa and theca cells, which become relevant when considering sex-cord stromal tumours that may cause hormonal symptoms. From pathology, recall the distinction between benign, borderline (low malignant potential), and frankly malignant tumours, and how surface epithelial cells of the ovary undergo metaplastic change under repeated ovulation trauma. From biochemistry, recall AFP (alpha-fetoprotein) as a yolk-sac marker and β-hCG as a trophoblastic marker — these become the tumour markers for germ cell tumours. Finally, recall how the peritoneal cavity provides a contiguous space for transcoeliomic spread from ovary to omentum, bowel serosa, and diaphragm.
Clinical Presentation and Risk Factors
Ovarian cancer has earned the sobriquet 'the silent killer' because it produces symptoms only when the disease has already spread beyond the ovary — and even those symptoms are distressingly non-specific. The classic triad of presenting symptoms is abdominal bloating, early satiety, and pelvic or abdominal discomfort. Urinary frequency or urgency from pressure on the bladder, altered bowel habit, dyspepsia, and unexplained weight loss or anorexia are also reported. By the time ascites is clinically detectable, disease is almost invariably Stage III or beyond. A retrospective study found that over 70% of women had symptoms for 3–6 months before presentation — the issue is not absence of symptoms but their attribution to benign conditions. Vaginal bleeding is relatively uncommon in epithelial ovarian cancer but may occur in endometrioid subtypes or when there is uterine involvement.
On examination, the typical late-stage patient has a palpable pelvic-abdominal mass (often bilateral and irregular), ascites (shifting dullness, fluid thrill), and sometimes pleural effusion detected by decreased breath sounds. Early-stage disease may present only as an incidental adnexal finding on ultrasound.
Risk factors for epithelial ovarian cancer (the predominant type) fall into genetic, reproductive, and environmental categories. Genetic risk is dominated by BRCA1 mutations (lifetime ovarian cancer risk ~44%) and BRCA2 mutations (lifetime risk ~17%), compared with a 1.3% background risk. Lynch syndrome (hereditary non-polyposis colorectal cancer, due to mismatch repair gene mutations) carries a 6–10% lifetime ovarian cancer risk and is also associated with endometrial cancer — making family history of colorectal and endometrial cancer relevant. Reproductive factors that increase risk include nulliparity, early menarche, late menopause, and use of postmenopausal hormone replacement therapy (oestrogen-only or combined). Conversely, oral contraceptive pill use (even for 3–5 years) reduces ovarian cancer risk by 30–50%, as does multiparity, breastfeeding, and tubal ligation — all sharing the mechanism of suppressing ovulation ('incessant ovulation hypothesis': each ovulation creates a wound at the ovarian surface that must repair, and accumulated repair errors drive malignant transformation). Endometriosis is associated with a modestly increased risk of clear-cell and endometrioid subtypes. Talc exposure to the perineum has been debated but evidence remains weak.
Provided image
Pathology and Classification of Ovarian Tumours
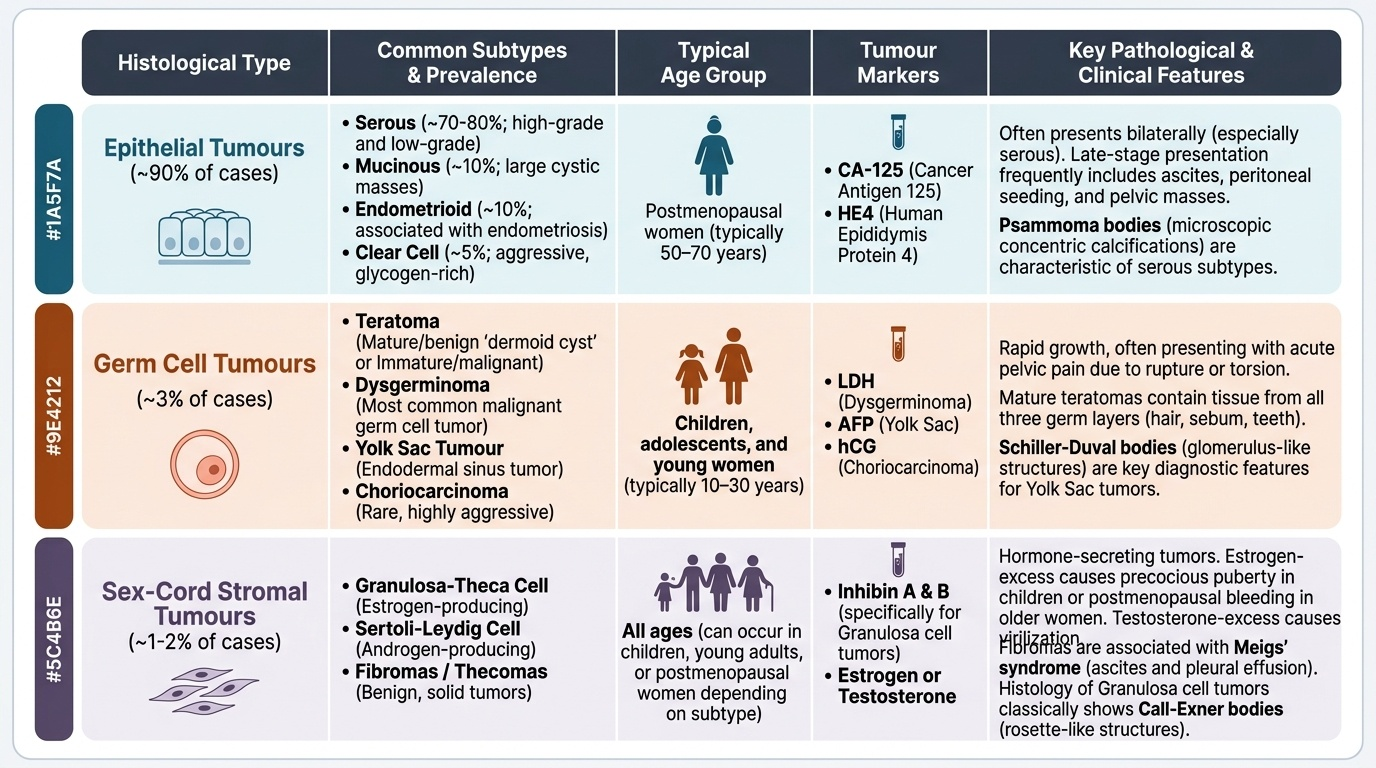
Ovarian tumours are classified by their cell of origin into three broad histological groups, each with distinct biology, age distribution, clinical behaviour, and therapeutic implications. Understanding this classification is non-negotiable because the management of a dysgerminoma in a 19-year-old differs fundamentally from that of a high-grade serous carcinoma in a 60-year-old.
Epithelial tumours arise from the surface epithelium (celomic epithelium) of the ovary or, increasingly recognised, from the fimbriated end of the fallopian tube (serous carcinomas). They constitute approximately 90% of all ovarian malignancies. Within this group, serous carcinoma is the most common (~70% of epithelial), subdivided into high-grade (aggressive, TP53 and BRCA mutations, late stage at diagnosis) and low-grade (indolent, KRAS/BRAF mutations). Mucinous carcinoma is often unilateral and large; when bilateral, consider metastasis from colon or stomach (Krukenberg tumour). Endometrioid carcinoma is associated with endometriosis and may co-exist with endometrial carcinoma. Clear cell carcinoma has the worst prognosis among epithelial types, is associated with endometriosis, and is relatively chemoresistant. Brenner tumour is mostly benign (transitional cell type). Borderline tumours (tumours of low malignant potential) have atypical epithelial proliferation without stromal invasion — they have an excellent prognosis and may be managed conservatively in young women.
Germ cell tumours arise from the primordial germ cells and constitute approximately 5% of ovarian malignancies overall, but are the predominant malignant type in children and young women (under 30). Dysgerminoma is the most common malignant germ cell tumour (counterpart of testicular seminoma); it is highly radiosensitive and chemosensitive, often cured even at advanced stage. Yolk sac tumour (endodermal sinus tumour) secretes AFP and is highly aggressive but responsive to BEP chemotherapy. Immature teratoma contains embryonic-type tissue and is graded 1–3 by the amount of immature neuroepithelium. Mixed germ cell tumours contain more than one germ cell element. Germ cell tumours are often unilateral and allow fertility-preserving surgery (unilateral salpingo-oophorectomy + staging).
Sex-cord stromal tumours arise from the supporting cells of the ovary and account for ~5–8% of ovarian malignancies. Granulosa cell tumour is the most common malignant type and secretes oestrogen (causing post-menopausal bleeding or precocious puberty in children) and inhibin (a useful tumour marker). It has a slow clinical course but can recur decades later (late recurrence is a hallmark). Sertoli-Leydig cell tumour secretes androgens and may cause virilisation. Fibrothecoma is usually benign. A special association: Meigs syndrome = benign ovarian fibroma + ascites + right pleural effusion (resolves after tumour removal).
A clinically important secondary ovarian tumour is the Krukenberg tumour — bilateral metastatic deposits from a primary gastric carcinoma (signet-ring cell type), less commonly from colorectal, breast, or appendix primaries. Always suspect bilaterality and a primary elsewhere.
FIGO 2014 Staging of Ovarian Cancer (Stages I–IV)
FIGO Staging of Ovarian Cancer
Ovarian cancer is staged surgically according to the FIGO 2014 classification — this is emphatically its OWN system and must not be confused with the FIGO 2018 cervical cancer staging or the FIGO endometrial cancer staging, both of which have entirely different stage definitions and sub-stage criteria. The stage is assigned in the operating theatre based on the extent of disease found during staging laparotomy and systematic exploration, not on preoperative imaging alone. This is a fundamental principle: imaging may suggest advanced disease but the definitive FIGO stage must be assigned surgically, which means that a patient who proceeds directly to neoadjuvant chemotherapy without surgery must still have a histological confirmation of malignancy (via laparoscopic biopsy or ascitic cytology) before chemotherapy begins, and the full surgical stage is assigned only at the time of interval debulking surgery. The system runs from Stage I (disease confined to the ovary or fallopian tube) through Stage IV (distant metastasis beyond the peritoneum), with meaningful sub-stages that influence both prognosis and the extent of surgical and chemotherapeutic management.
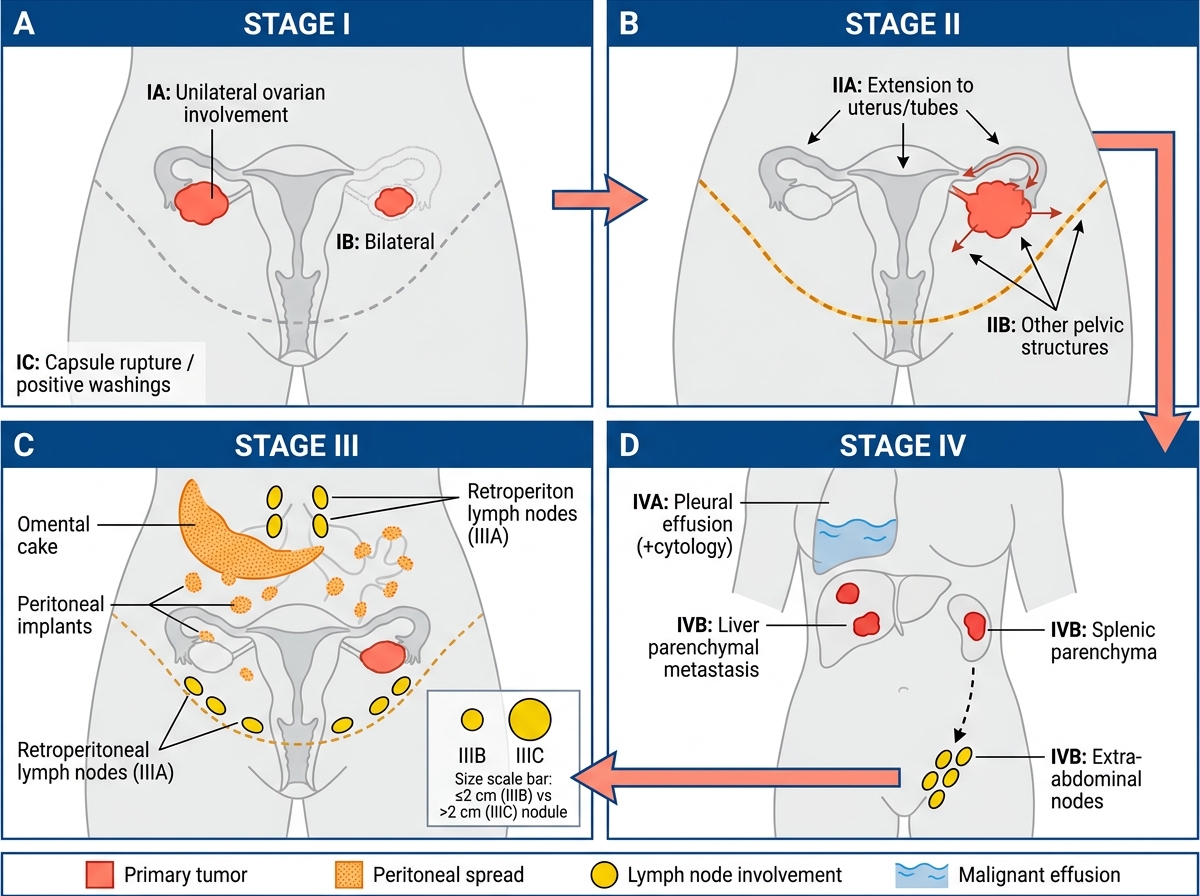
Stage I — confined to ovary(ies) or fallopian tube(s):
- IA: one ovary, capsule intact, no surface tumour, negative washings
- IB: both ovaries, capsule intact, no surface tumour, negative washings
- IC: IC1 = surgical spill; IC2 = pre-operative capsule rupture or surface tumour; IC3 = positive ascites or peritoneal washings
Stage II — pelvic extension or primary peritoneal cancer:
- IIA: extension/implants on uterus or fallopian tubes
- IIB: extension to other pelvic intraperitoneal structures
Stage III — spread to peritoneum outside pelvis and/or retroperitoneal lymph nodes:
- IIIA1: retroperitoneal lymph nodes only (IIIA1i ≤10 mm; IIIA1ii >10 mm)
- IIIA2: microscopic peritoneal metastasis beyond pelvis with or without retroperitoneal nodes
- IIIB: peritoneal metastasis >2 cm or more beyond pelvis, with or without retroperitoneal nodes
- IIIC: peritoneal metastasis >2 cm beyond pelvis, including spread to liver and spleen surfaces, with or without retroperitoneal nodes
Stage IV — distant metastasis beyond peritoneum:
- IVA: pleural effusion with positive cytology
- IVB: hepatic or splenic parenchymal metastases; extra-abdominal organs (including inguinal nodes)
The most important clinical fact: most patients (60–70%) present at Stage III–IV when the peritoneal surface is already seeded. The omentum is a particularly common site of spread ('omental cake') and is always removed at surgery (omentectomy). Diaphragmatic and bowel serosal implants drive the sub-staging within Stage III. Because staging is surgical, women undergoing neoadjuvant chemotherapy followed by interval debulking must have a biopsy-confirmed diagnosis before chemotherapy commences — surgery alone assigns the definitive FIGO stage.
Provided image
SELF-CHECK
A 67-year-old woman has ovarian cancer with peritoneal deposits in the omentum (>2 cm) and positive para-aortic lymph nodes. Liver MRI shows no parenchymal deposits; pleural effusion cytology is negative. What is her FIGO stage?
A. Stage IIIB
B. Stage IIIC
C. Stage IVA
D. Stage IVB
Reveal Answer
Answer: B. Stage IIIC
Stage IIIC requires peritoneal metastasis >2 cm beyond the pelvis (which omental deposits >2 cm satisfy) AND/OR retroperitoneal node involvement. Both criteria are met. Stage IV requires distant metastasis: IVA = positive pleural effusion cytology (negative here), IVB = hepatic parenchymal deposits (absent here). Surface liver deposits are Stage III, not IV.