Page 17 of 37
OG34.2 | Ovarian Cancer — SDL Guide (Part 2)
Investigations and Tumour Markers
The investigation of a suspected ovarian malignancy begins with risk stratification using the Risk of Malignancy Index (RMI), a validated scoring tool that combines three variables to distinguish benign from malignant adnexal masses before surgery. The RMI (Jacobs 1990 formula) = Menopausal status score (M) × Ultrasound score (U) × CA-125 (IU/mL), where M = 1 (premenopausal) or 3 (postmenopausal); U = 1 (one ultrasound feature: multilocular cysts, solid areas, bilateral lesions, ascites, intra-abdominal metastases) or 3 (two or more features). An RMI >200 identifies high-risk patients who should be referred to a gynaecological oncology centre for definitive surgery. An RMI <25 suggests low risk (likely benign); 25–200 is indeterminate and warrants careful further evaluation.
Ultrasound (transvaginal preferred) remains the first-line imaging modality. Features suggesting malignancy include: bilateral masses, solid or mixed echogenicity (solid + cystic), internal papillary projections or septations >3 mm, irregular contour, increased vascularity on Doppler (low-resistance flow), and free fluid (ascites). An entirely unilocular anechoic thin-walled cyst <5 cm in a postmenopausal woman is almost certainly benign.
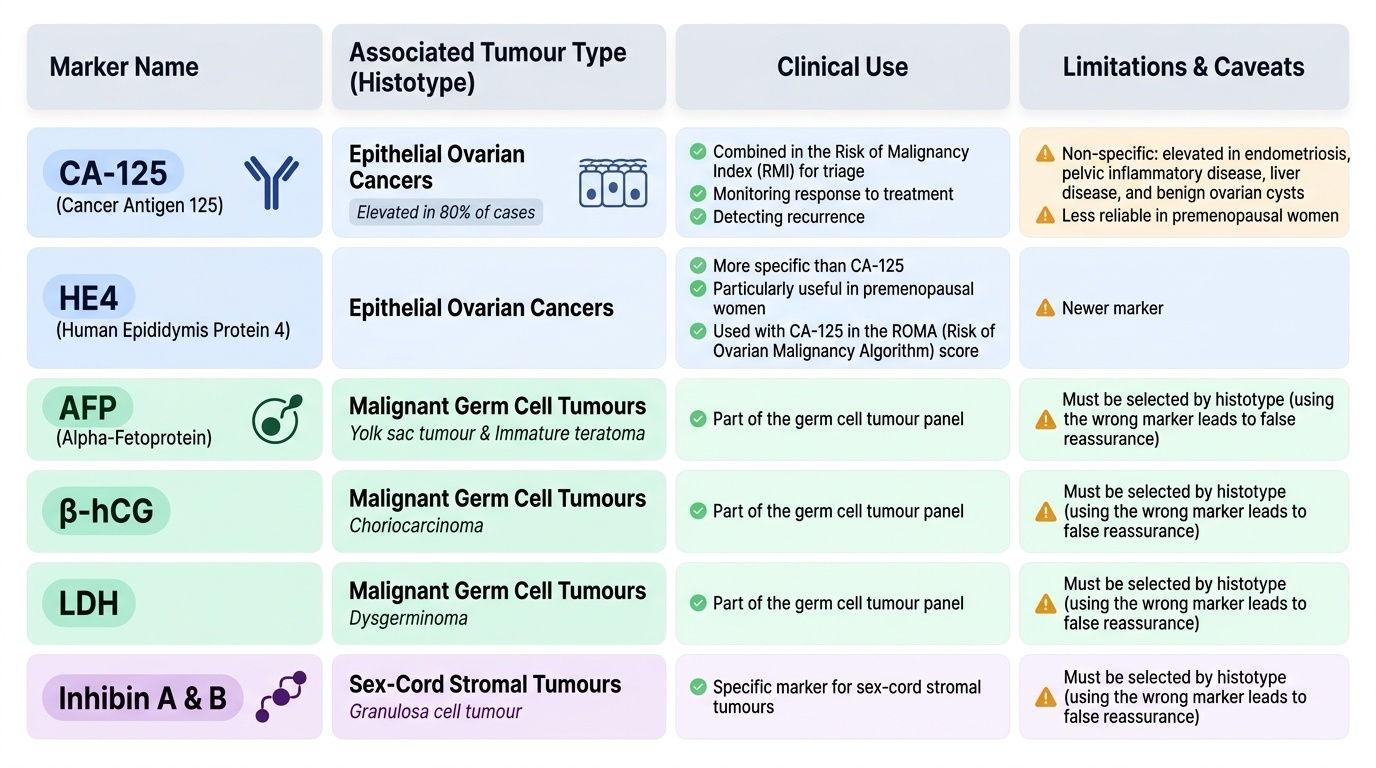
Tumour markers must be selected by histotype — using the wrong marker leads to false reassurance. CA-125 (Cancer Antigen 125): elevated (>35 U/mL) in 80% of epithelial ovarian cancers, but non-specific (also elevated in endometriosis, pelvic inflammatory disease, liver disease, and benign ovarian cysts). It is less reliable in premenopausal women. CA-125 is most useful for monitoring response to treatment and detecting recurrence. AFP (alpha-fetoprotein) + β-hCG + LDH: the germ cell tumour panel. AFP is elevated in yolk sac tumour and immature teratoma; β-hCG in choriocarcinoma; LDH in dysgerminoma. Inhibin A and B: elevated in granulosa cell tumour (sex-cord stromal). HE4 (Human Epididymis protein 4): newer marker, more specific than CA-125, particularly useful in premenopausal women; used with CA-125 in the ROMA (Risk of Ovarian Malignancy Algorithm) score.
For staging and surgical planning, CT abdomen/pelvis with contrast is the standard imaging once malignancy is suspected — it identifies peritoneal deposits, retroperitoneal adenopathy, liver/spleen involvement, and pleural effusions. MRI pelvis better characterises the primary mass (tissue characterisation). Chest X-ray detects pleural effusion. Ascitic fluid cytology (paracentesis) can confirm malignancy in cases with obvious disseminated disease where upfront debulking surgery may not be feasible, guiding the decision for neoadjuvant chemotherapy.
Provided image
Differential Diagnosis
An adnexal mass has a broad differential diagnosis, and the clinical challenge lies in distinguishing malignant from benign causes, especially in premenopausal women where functional ovarian changes are common. The following framework helps systematic differential reasoning, moving from most common benign causes to malignant lesions.
Functional/physiological cysts: Follicular cysts (simple, thin-walled, <8 cm, resolve spontaneously over 4–8 weeks in premenopausal women; do not occur after the menopause — a persistent simple cyst post-menopause must be investigated). Corpus luteum cysts can be haemorrhagic and may mimic malignancy on ultrasound; they also resolve with menstrual cycles.
Benign ovarian neoplasms: Serous cystadenoma (most common benign ovarian tumour), mucinous cystadenoma (may be very large, multilocular), mature cystic teratoma (dermoid cyst — commonest ovarian tumour overall; contains echogenic shadowing fat/teeth on ultrasound; bilateral in 10–15%; risk of torsion), ovarian fibroma (solid, hypoechoic), endometrioma ('chocolate cyst' — ground-glass or low-level homogeneous echoes on ultrasound, associated with endometriosis).
Conditions mimicking ovarian malignancy: Pedunculated fibroid (arises from the uterus; MRI distinguishes), hydrosalpinx (tubular structure with incomplete septa), tubo-ovarian abscess (in context of PID — fever, pelvic tenderness, raised CRP), pelvic kidney (IVU confirms), colorectal or appendiceal mass, retroperitoneal tumour, para-ovarian cyst.
Metastatic disease to the ovary (Krukenberg tumour): Bilateral solid ovarian masses in a patient with anorexia, weight loss, or history of gastrointestinal malignancy should always raise suspicion. Gastric primary is most common; also consider colon, breast, appendix. CA-125 may be elevated. Upper GI endoscopy or CT of the abdomen is essential in this scenario.
| Diagnosis | Age Group | Ultrasound Features | Key Distinguishing Point |
|---|---|---|---|
| Follicular cyst | Reproductive | Simple, thin-walled, <8 cm | Resolves in 4–8 weeks; post-menopausal = never functional |
| Dermoid (mature teratoma) | Young (peak 20s) | Echogenic, shadowing, fat-fluid level | CA-125 normal; bilateral 10–15% |
| Endometrioma | Reproductive | Ground-glass/homogeneous low echo | History of dysmenorrhoea, dyspareunia, infertility |
| Serous carcinoma | Post-menopausal | Bilateral solid-cystic, ascites | High CA-125, RMI >200 |
| Mucinous carcinoma | All ages | Large multilocular, unilateral | Check appendix/colon if bilateral |
| Granulosa cell tumour | Peri/postmenopause, children | Solid-cystic, unilocular | Oestrogen excess symptoms, inhibin elevated |
| Krukenberg tumour | Any age | Bilateral solid, irregular | Gastric/colorectal primary; upper GI symptoms |
SELF-CHECK
A 23-year-old woman has a right adnexal mass with AFP 2,400 ng/mL, normal CA-125, normal β-hCG. CT shows a solid-cystic right ovarian mass with no evidence of peritoneal disease. What is the most likely diagnosis and how does this affect surgical planning?
A. High-grade serous carcinoma; requires immediate bilateral salpingo-oophorectomy
B. Yolk sac tumour (germ cell); fertility-sparing unilateral salpingo-oophorectomy is appropriate
C. Granulosa cell tumour; inhibin level should be checked
D. Mucinous carcinoma; appendicectomy should accompany surgery
Reveal Answer
Answer: B. Yolk sac tumour (germ cell); fertility-sparing unilateral salpingo-oophorectomy is appropriate
Markedly elevated AFP with a solid ovarian mass in a young woman is highly characteristic of a yolk sac tumour (endodermal sinus tumour), a germ cell tumour. Germ cell tumours are usually unilateral, and in young women, fertility-preserving surgery (unilateral salpingo-oophorectomy + surgical staging) is standard — unlike epithelial ovarian cancer where bilateral surgery is routine. Post-operatively, BEP chemotherapy (bleomycin, etoposide, cisplatin) provides excellent outcomes even with stage IC–III disease.
Management — Staging Laparotomy and Cytoreductive Surgery
Surgical management is central to both staging and treatment of ovarian cancer, and the two objectives — accurate staging and maximal cytoreduction — are often achieved in the same operation. Surgery is performed through a midline vertical incision (allowing adequate exposure of the upper abdomen).
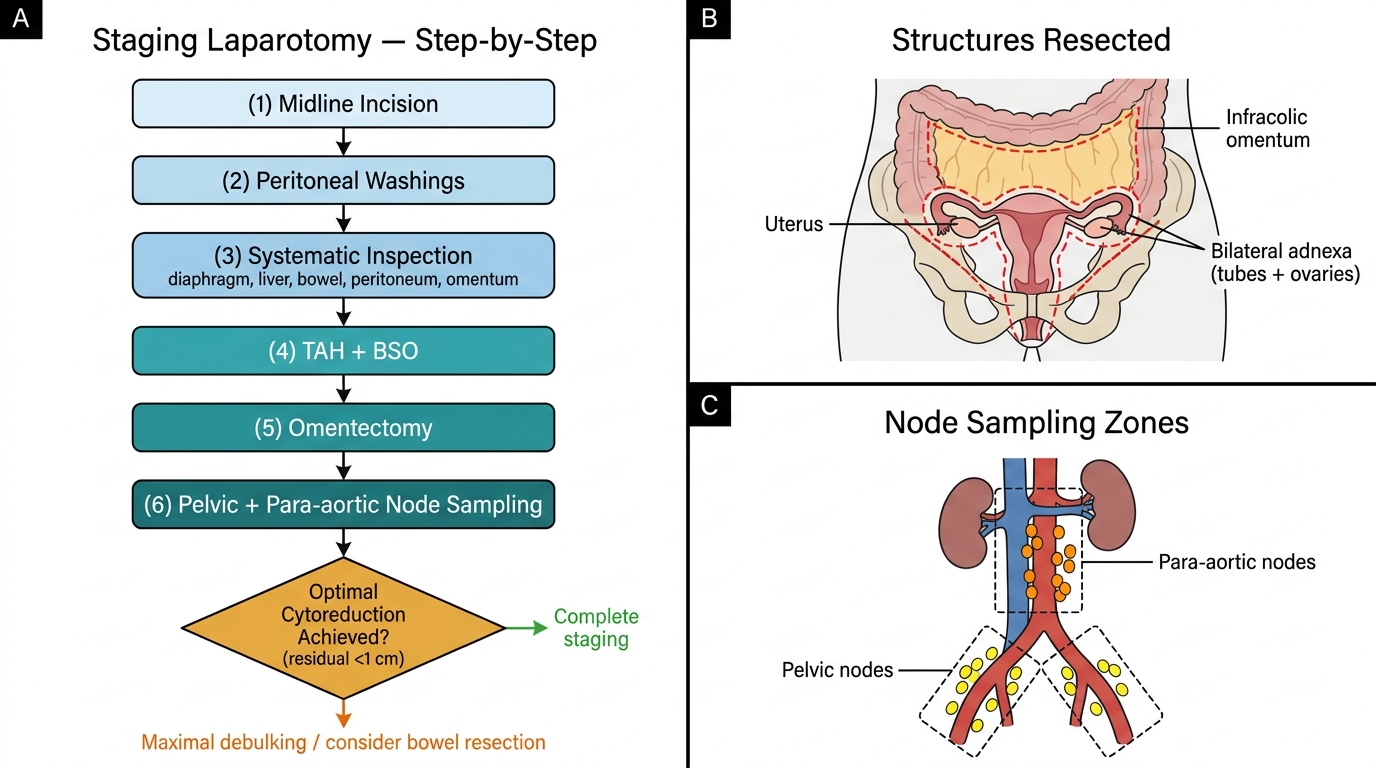
A staging laparotomy for presumed early-stage disease includes a systematic set of steps: (1) obtain peritoneal washings from the pelvis, right and left paracolic gutters, and subdiaphragmatic areas at the time of opening the abdomen; (2) careful inspection of all peritoneal surfaces including diaphragm, omentum, bowel serosa, and paracolic gutters for deposits; (3) total abdominal hysterectomy (TAH) + bilateral salpingo-oophorectomy (BSO) as the cornerstone procedure; (4) infragastric omentectomy (omentum is a common site of microscopic spread and 'omental cake' formation); (5) pelvic and para-aortic lymph node sampling/dissection (para-aortic nodes receive direct drainage from the ovary via ovarian vessels — this is the primary nodal basin, often before pelvic nodes); (6) random peritoneal biopsies from cul-de-sac, both paracolic gutters, pelvic sidewalls, and diaphragm even if visually normal; (7) appendicectomy particularly for mucinous tumours (to exclude an appendiceal primary Krukenberg source).
Cytoreductive surgery (debulking) applies to advanced-stage disease (III–IV). The surgical goal is optimal cytoreduction — residual tumour <1 cm maximum diameter (R1 ≤1 cm is standard; complete cytoreduction R0 is ideal). Survival is directly correlated with residual tumour burden: women with R0 have significantly better progression-free and overall survival than those with R1 >1 cm. Extensive upper abdominal surgery may be required: bowel resection with anastomosis, splenectomy, liver resection, diaphragm stripping or peritonectomy. This is complex surgery requiring a multidisciplinary gynaecological oncology team.
For patients unfit for upfront surgery or with very extensive disease where R0 is unlikely, neoadjuvant chemotherapy (NACT) followed by interval debulking surgery (IDS) after 3 cycles of carboplatin-paclitaxel is an established alternative (EORTC 55971, CHORUS trials showed non-inferiority for overall survival in selected patients). IDS should target R0 when possible.
Fertility-preserving surgery is appropriate in young women with: (1) apparent unilateral early-stage germ cell tumours (unilateral salpingo-oophorectomy + staging); (2) Stage IA, Grade 1 epithelial tumours in carefully selected cases desiring fertility (retain uterus and contralateral ovary with comprehensive staging). Close oncological surveillance is mandatory.
Staging Laparotomy for Gynaecological Malignancy: Operative Sequence and Anatomical Targets