Page 18 of 37
OG34.2 | Ovarian Cancer — SDL Guide (Part 3)
Chemotherapy and Targeted Therapy
Ovarian cancer is one of the more chemosensitive solid tumours, and adjuvant or primary systemic chemotherapy is central to management of all but the earliest-stage disease. The choice of regimen depends on histological type, stage, and molecular profile.
For epithelial ovarian cancer, the current standard first-line regimen is carboplatin (AUC 5–6) + paclitaxel (175 mg/m²) every 3 weeks for 6 cycles (established by GOG 111 and OV10 trials replacing the older cisplatin+cyclophosphamide). Carboplatin is preferred over cisplatin in most settings because of comparable efficacy with a more favourable toxicity profile (less nephrotoxicity, neurotoxicity, nausea). Intraperitoneal (IP) chemotherapy delivers high drug concentrations directly to the peritoneal surface and has shown survival benefit in optimally debulked Stage III disease (GOG 172), but its toxicity and catheter-related complications have limited widespread adoption.
Bevacizumab (anti-VEGF monoclonal antibody) added to first-line carboplatin-paclitaxel and continued as maintenance has demonstrated a modest progression-free survival benefit (ICON7, GOG 218 trials), particularly in Stage IIIB–IV disease. It is not approved universally in resource-limited settings due to cost.
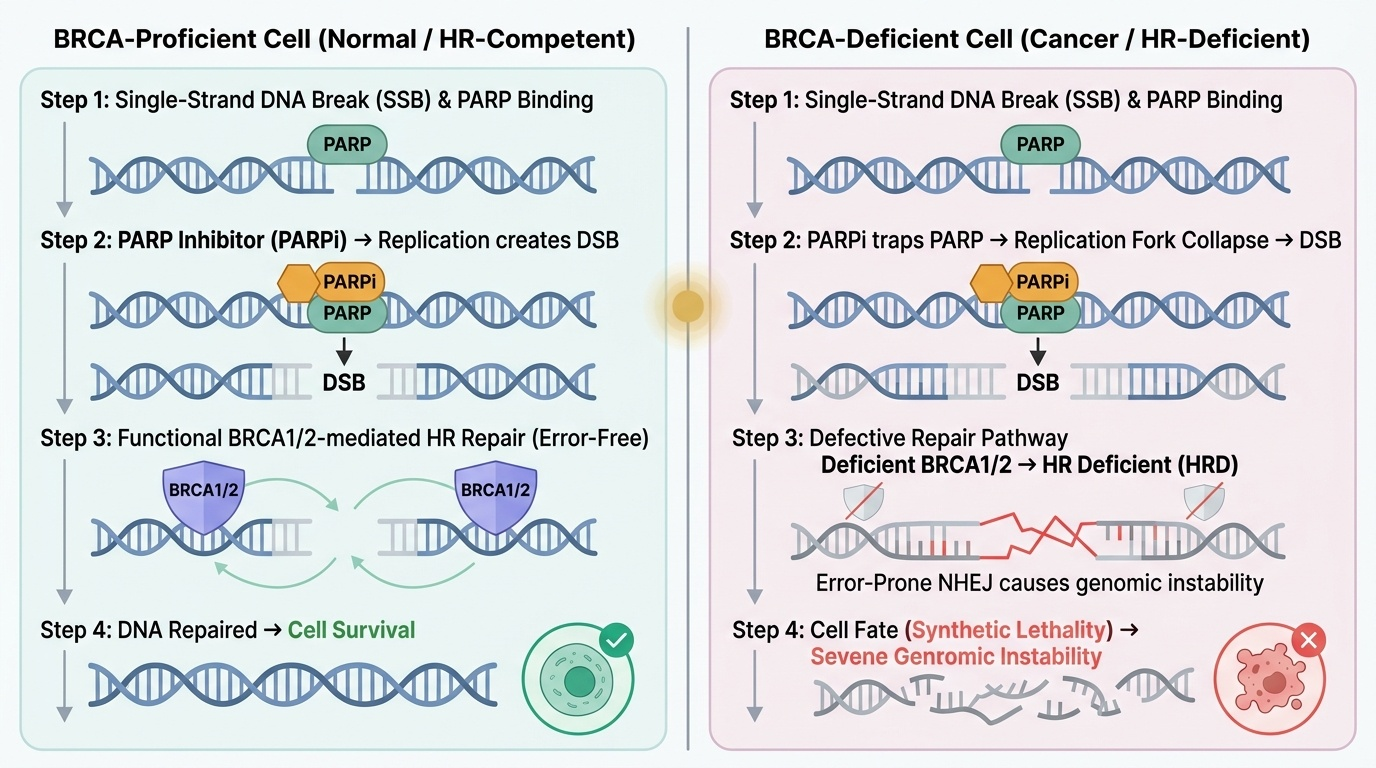
The most significant advance in ovarian cancer treatment is PARP inhibitor maintenance therapy for BRCA1/2-mutated advanced epithelial ovarian cancer. Olaparib (SOLO-1 trial) and niraparib (PRIMA trial) as maintenance after complete or partial response to first-line chemotherapy have markedly prolonged progression-free survival in patients with BRCA mutations or homologous recombination deficiency (HRD). All women with advanced epithelial ovarian cancer should be tested for germline and somatic BRCA mutations.
For germ cell tumours, the standard chemotherapy is BEP (bleomycin + etoposide + cisplatin) for 3–4 cycles, which achieves cure rates >95% even in advanced dysgerminoma and excellent outcomes in other germ cell types. Response is monitored by serial AFP, β-hCG, and LDH normalisation. Dysgerminoma is also radiosensitive, though chemotherapy is preferred to preserve fertility.
For sex-cord stromal tumours such as granulosa cell tumours, adjuvant chemotherapy (carboplatin + paclitaxel or BEP) is reserved for Stage IC and above. Surveillance with serum inhibin is used to detect recurrence, which can occur decades after initial treatment.
For platinum-resistant relapse (progression within 6 months of platinum completion), liposomal doxorubicin, topotecan, or gemcitabine are used. Platinum-sensitive relapse (>6 months after platinum) is re-treated with platinum-based combinations. PARP inhibitors also have a role in BRCA-mutated relapsed disease.
Provided image
CLINICAL PEARL
The ovarian FIGO staging system is surgical and specific to ovarian/fallopian tube/peritoneal cancer — it is completely different from cervical (FIGO 2018) and endometrial staging systems. The critical distinction within Stage III: Stage IIIA1 (retroperitoneal nodes only, no peritoneal metastasis) carries a significantly better prognosis than IIIB/IIIC (peritoneal disease). Additionally, the landmark finding about the cell of origin: high-grade serous carcinoma — the most common and lethal epithelial type — is now believed to originate predominantly from the fimbriated end of the fallopian tube (serous tubal intraepithelial carcinoma, STIC), not the ovarian surface epithelium itself. This has led to BRCA-positive women opting for risk-reducing salpingo-oophorectomy (RRSO) which removes the fallopian tubes along with the ovaries. Opportunistic bilateral salpingectomy at the time of other gynaecological surgery is increasingly recommended for general population risk reduction.
SELF-CHECK
A woman with Stage IIIC high-grade serous ovarian carcinoma undergoes optimal debulking (R0) followed by 6 cycles of carboplatin-paclitaxel. She achieves a complete clinical response. Germline BRCA1 mutation is confirmed. What is the most evidence-based next step?
A. Annual CA-125 surveillance; chemotherapy only at relapse
B. Olaparib maintenance therapy for 2 years
C. Immediate second-look laparotomy to confirm pathological complete response
D. Consolidation whole-abdomen radiotherapy
Reveal Answer
Answer: B. Olaparib maintenance therapy for 2 years
The SOLO-1 trial demonstrated that olaparib maintenance (a PARP inhibitor) for 2 years after complete or partial response to first-line platinum-based chemotherapy in BRCA1/2-mutated advanced ovarian cancer significantly prolonged progression-free survival (median 56 months vs 13.8 months with placebo). Second-look laparotomy has been abandoned as it did not improve survival. Whole-abdomen radiotherapy is no longer used. Surveillance-only is inferior to maintenance olaparib in BRCA-mutated disease.
Prognosis and Surveillance
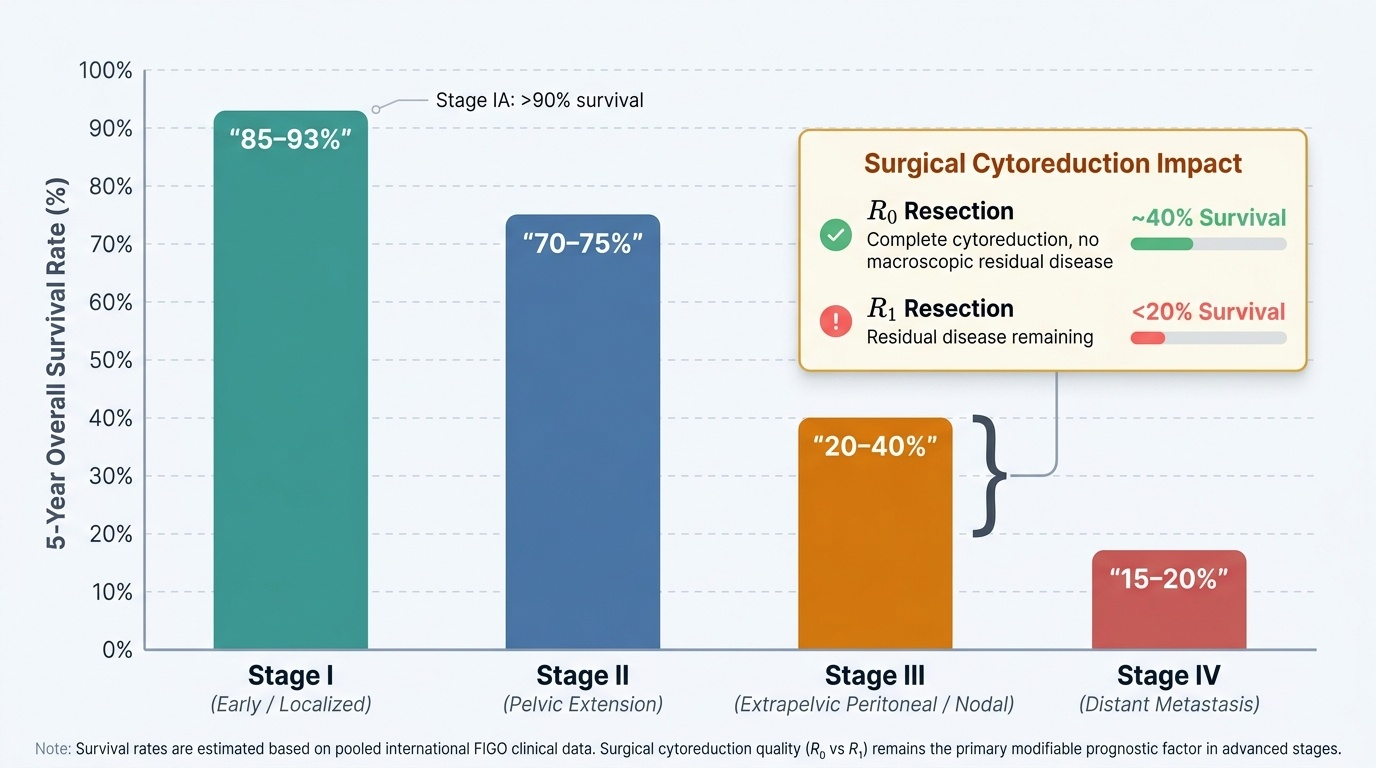
Prognosis in ovarian cancer is predominantly stage-driven, with histological type, grade, and residual tumour burden also contributing significantly. The outcome gap between early and advanced disease is wider for ovarian cancer than for almost any other gynaecological malignancy — a woman diagnosed at Stage IA has a greater than 90% chance of long-term survival, while a woman diagnosed at Stage IIIC has less than a 40% chance even with optimal treatment. This stark disparity explains why the absence of an effective screening programme is such a public health concern: by the time symptoms bring a woman to clinical attention, she is usually already in the advanced-stage group. Within advanced-stage disease, the quality of surgical cytoreduction is itself a prognostic modifier — a woman achieving complete cytoreduction (R0) at staging laparotomy has meaningfully better outcomes than one with residual disease, even within the same FIGO stage. This means that the surgical team's decisions in the operating theatre directly affect long-term survival. The 5-year overall survival rates by FIGO stage (approximate values from pooled international data):
- Stage I: ~85–93% (IA > IB > IC; IC3 somewhat worse)
- Stage II: ~70–75%
- Stage III: ~20–40% (IIIA1 better than IIIC; R0 debulking improves survival within stage)
- Stage IV: ~15–20%
Histological type modifies the prognosis within stage: clear cell carcinoma has worse stage-for-stage prognosis than serous carcinoma; mucinous carcinoma is often chemoresistant at advanced stage. Germ cell tumours (particularly dysgerminoma) have an excellent prognosis even at advanced stage due to chemosensitivity. Granulosa cell tumours have an indolent course but are notable for very late recurrence — surveillance must be lifelong.
Post-treatment surveillance follows a structured protocol. CA-125 is measured every 3 months for the first 2 years, then every 6 months for 3 years, then annually. A rising CA-125 (confirmed on two readings, 2 weeks apart) precedes clinical or radiological relapse by a median of 3–5 months ('lead time'). However, the ICON4 trial found that treating CA-125-only relapse without clinical symptoms did not improve survival over waiting for symptomatic relapse — the current approach is to use a rising CA-125 to prompt CT scanning and clinical review, not automatic chemotherapy re-initiation. CT abdomen/pelvis is the standard imaging at suspected relapse.
Second-look laparotomy (surgical re-exploration after completing chemotherapy to assess pathological complete response in clinically responding patients) was practiced in the 1980s–1990s but has been abandoned — it did not improve overall survival in randomised trials.
Genetic counselling and cascade testing: All women diagnosed with epithelial ovarian cancer (especially serous and endometrioid types under age 70, and all clear-cell and mucinous at any age) should be offered germline BRCA1/2 and mismatch repair gene (Lynch syndrome) testing. Positive results enable cascade genetic testing of first-degree relatives, allowing risk-reducing interventions including RRSO and enhanced breast surveillance in BRCA carriers.
Provided image
SELF-CHECK
A postmenopausal woman completes primary surgery (optimal debulking, FIGO Stage IIIC high-grade serous carcinoma) and 6 cycles of carboplatin-paclitaxel. She is clinically in remission with CA-125 14 U/mL. Germline BRCA testing is negative. At her 18-month follow-up, CA-125 rises from 14 to 28 to 52 U/mL on three serial measurements. She is asymptomatic. What is the most appropriate next action?
A. Immediately commence salvage chemotherapy with liposomal doxorubicin
B. Arrange CT abdomen/pelvis and clinical review; delay chemotherapy until symptomatic or imaging-confirmed relapse
C. Repeat CA-125 in 3 months and observe
D. Proceed to second-look laparotomy to confirm relapse
Reveal Answer
Answer: B. Arrange CT abdomen/pelvis and clinical review; delay chemotherapy until symptomatic or imaging-confirmed relapse
The ICON4 evidence showed no survival benefit from treating CA-125-only relapse before clinical symptoms manifest. The appropriate response to a rising CA-125 is to perform CT abdomen/pelvis to look for radiological evidence of relapse and to manage the patient in an informed, multidisciplinary way — but not to immediately start chemotherapy based on CA-125 alone in an asymptomatic patient. Second-look laparotomy is no longer performed.