Page 10 of 29
OG35.{7,9-10,14} | Communication, Ethics, Consent and Universal Precautions — SDL Guide (Part 2)
Ethical Behaviour in Clinical OG Practice
Ethical behaviour in obstetrics and gynaecology is not simply about following rules — it is about applying a consistent moral framework to every clinical decision, especially when values conflict. The most common ethical tensions in OG practice arise at the intersection of patient autonomy, clinical beneficence, legal obligation, and family pressure.
Reproductive autonomy is a foundational ethical principle in OG. A woman has the right to make decisions about her own reproductive life — including contraception, pregnancy continuation, and sterilisation — free from coercion by her family, healthcare provider, or state. The NMC AETCOM framework specifically identifies reproductive coercion as an ethical violation. Practically, this means: never performing a sterilisation procedure without the patient's independent, written, informed consent (even if the husband requests it); never discouraging a patient from requesting MTP on personal moral grounds; and never allowing family pressure to override the patient's documented wishes.
Confidentiality in OG is particularly complex because multiple parties have interests in the patient's information. Key rules: results of investigations (HIV status, STI results, pregnancy terminations) may not be disclosed to family members without the patient's explicit consent. Police enquiries require a specific legal instrument (court order or FIR documentation) before disclosure. In cases of domestic violence, the clinician may encourage the patient to seek help but cannot make a report without the patient's consent except in specific circumstances (threat to life of a minor, mandatory reporting under POCSO Act for patients under 18).
PCPNDT compliance: the Pre-Conception and Pre-Natal Diagnostic Techniques Act 1994 prohibits the use of any diagnostic technique for the purpose of sex determination. This includes not merely stating the fetal sex, but also communicating it indirectly (e.g. a raised eyebrow, a cryptic comment, 'the baby is very active'). Every person who performs, assists, or referres a patient for ultrasonography must be registered under PCPNDT. The penalty for violation includes imprisonment and removal from the medical register.
Ethical complexity at the end of life in OG: when a pregnant woman is critically ill (e.g. in irreversible shock after a ruptured ectopic), decisions about withdrawing treatment and the interests of the fetus must be made within a framework of shared decision-making that includes the family, the treating team, and in some cases a clinical ethics committee. The principle of double effect (an action intended to relieve suffering may have a foreseen but unintended harmful effect) has specific OG applications.
SELF-CHECK
A pregnant woman is HIV-positive. Her husband does not know. She asks you not to disclose. Under the principles governing confidentiality in OG practice, which response is most appropriate?
A. Disclose to the husband immediately, because he has a right to know about risk to himself
B. Maintain confidentiality; counsel the patient about partner notification and the benefits of disclosure; document your counselling
C. Report to the district health officer, as HIV is a notifiable disease
D. Withhold antenatal care until the patient consents to disclosure
Reveal Answer
Answer: B. Maintain confidentiality; counsel the patient about partner notification and the benefits of disclosure; document your counselling
Confidentiality is a fundamental ethical and legal obligation. HIV status is sensitive personal information and may not be disclosed to the husband without the patient's consent. The correct approach is to maintain confidentiality, counsel the patient about the importance of partner notification and the availability of support, offer to assist with disclosure if she is willing, and document the counselling given. Coercive disclosure or withholding care are unethical and illegal. HIV is reportable in an aggregate, anonymised form but not in a way that identifies the individual patient to family members.
Obtaining Informed Consent for OG Procedures
Provided image
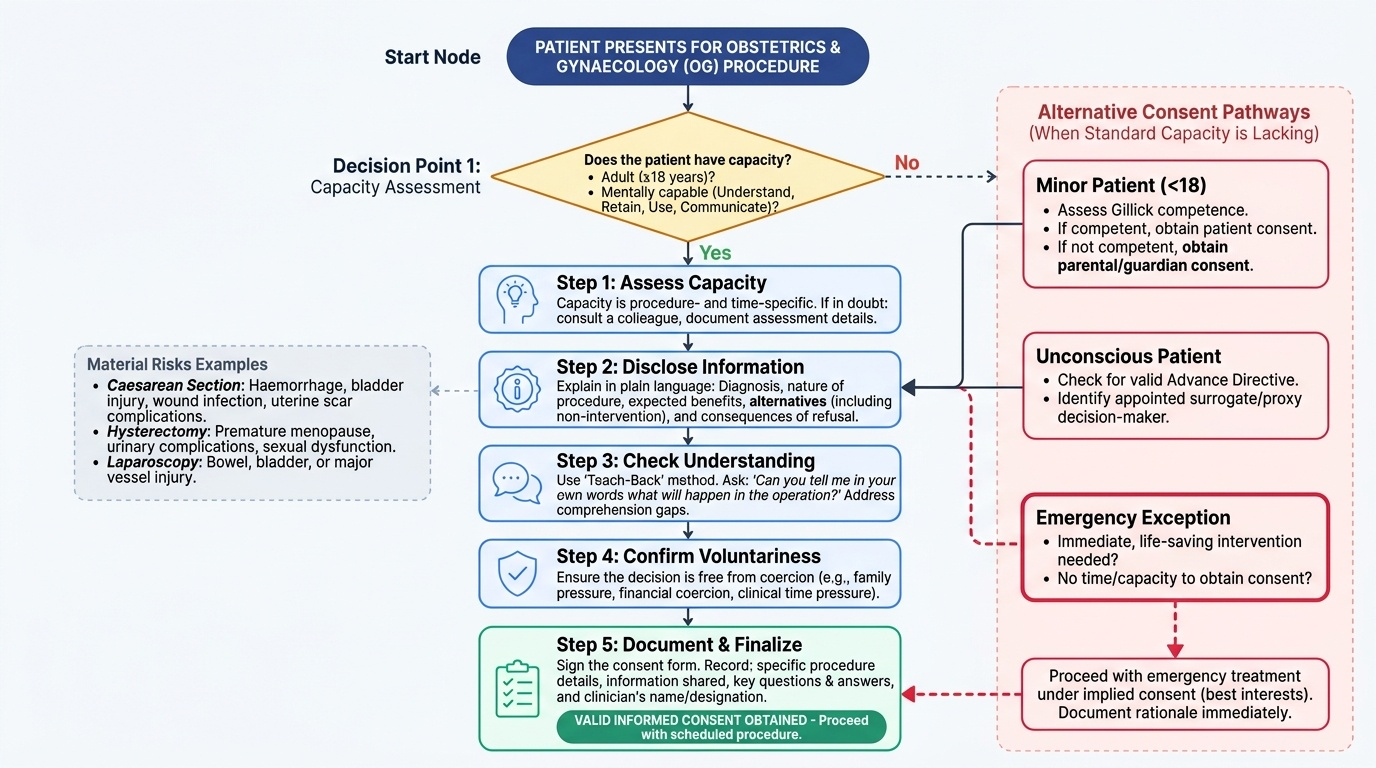
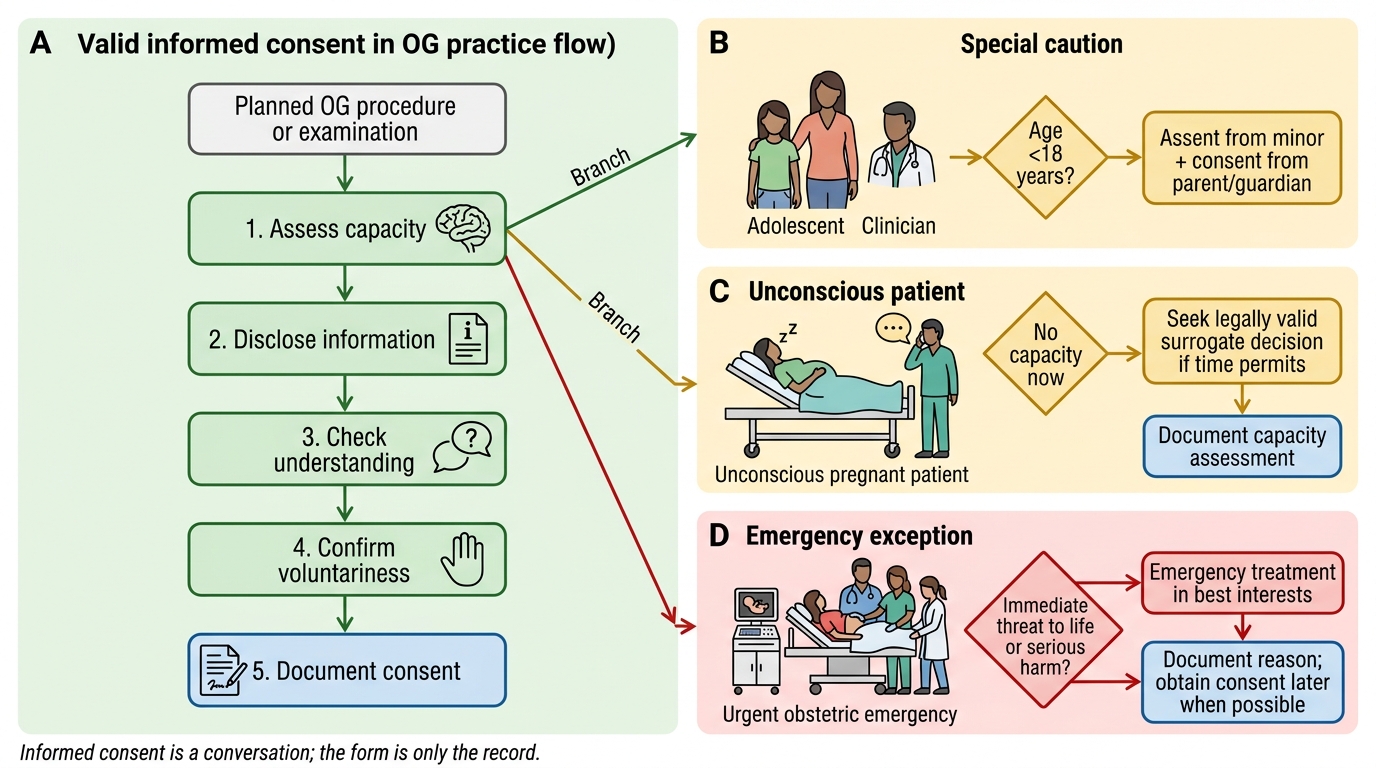
Informed consent in obstetrics and gynaecology is a process, not a form. The consent form is the written record of a conversation — it is not a substitute for that conversation. A signature on a consent form obtained under duress, without comprehension, or from a patient who lacked capacity is legally invalid regardless of the clinical need for the procedure.
The process of obtaining valid informed consent involves five sequential steps:
Step 1 — Assess capacity: the patient must be an adult (≥18 years) with the mental capacity to understand information, retain it, use it in decision-making, and communicate a decision. Capacity is procedure-specific and time-specific — a patient may lack capacity today (due to acute illness or drug effect) but regain it tomorrow. If capacity is in doubt, consult a colleague and document your assessment.
Step 2 — Disclose: explain in plain language: (a) the diagnosis or reason for the procedure; (b) the nature of the proposed procedure and what it involves; (c) the expected benefits; (d) the material risks — those which are common, or which are rare but serious; (e) the available alternatives including non-intervention; and (f) the consequences of refusal. In OG, 'material risks' for common procedures include: for caesarean section — haemorrhage, bladder injury, wound infection, future uterine scar complications; for hysterectomy — premature menopause, urinary complications, sexual function; for laparoscopy — injury to bowel, bladder, or major vessels.
Step 3 — Check understanding: ask the patient to explain back what she has understood, not just whether she has any questions. 'Can you tell me in your own words what will happen in the operation?' This reveals comprehension gaps that simple question-asking does not.
Step 4 — Confirm voluntariness: consent obtained under coercion is invalid. This includes family pressure ('my husband says I must agree'), financial coercion ('we will not treat you if you don't sign'), and time pressure ('sign now or it will be too late'). The clinician must ensure the patient is making a free decision.
Step 5 — Document: the signed consent form records: the procedure, the information given, the patient's questions and answers, and the name and designation of the clinician who obtained consent. Consent is not obtained by the person performing the procedure — it can be obtained by any appropriately trained clinician who is competent to answer questions about the procedure.
Special consent situations in OG:
- Sterilisation: requires written informed consent from the woman alone (not the husband). The MTP Act and Family Welfare Programme guidelines additionally require a minimum waiting period and repeat counselling to ensure no coercion.
- MTP: written opinion of the registered medical practitioner(s) required (see documentation module). The woman's consent is mandatory; no third party can consent on her behalf.
- Minor (under 18 years): guardian consent is required, plus the patient's own assent where she has sufficient maturity. In emergencies where a guardian is unavailable and life is at risk, the treating clinician may proceed without consent and document the emergency exception.
- Unconscious patient: a next-of-kin (spouse, adult child, parent in that order) may provide proxy consent. If no kin is available and delay would cause death or serious harm, the clinician may proceed in the patient's best interest and document fully.
- Refusal of consent: a competent adult has the absolute right to refuse treatment, including in life-threatening situations. The clinician must ensure the refusal is informed, document it (ideally with the patient's signature on a 'refusal of consent' form), and offer continued care and monitoring.
Informed Consent Decision Flow in OG
Universal Precautions in Obstetric and Gynaecological Settings
Standard precautions (commonly called universal precautions) are the minimum infection-prevention measures applied to every patient contact involving potential exposure to blood, body fluids, non-intact skin, or mucous membranes — regardless of whether the patient is known to carry a blood-borne pathogen. In obstetrics and gynaecology, blood and amniotic fluid exposure is routine during every vaginal examination, delivery, and operative procedure; standard precautions are therefore not optional additions but baseline professional conduct.
The principal components of standard precautions in OG settings are:
Hand hygiene is the single most effective infection-prevention measure and must be performed at the WHO five moments: before patient contact, before an aseptic task, after body fluid exposure, after patient contact, and after contact with the patient's surroundings. In OG ward and labour room settings, alcohol-based hand rub is effective for routine decontamination; soap and water is required when hands are visibly soiled or after contact with spores (Clostridioides).
Personal protective equipment (PPE) in OG must be selected based on the anticipated level of exposure:
- Gloves (non-sterile) for vaginal examination, venepuncture, handling blood-stained linen
- Sterile gloves for delivery, operative procedures, catheterisation
- Apron or gown (impermeable) for deliveries and any procedure with splash risk
- Eye protection (goggles or face shield) for deliveries, assisted vaginal delivery, LSCS
- Surgical mask for procedures involving splash or aerosol risk
The donning and doffing sequence must be learned and practised precisely. PPE is put on in the order: hand hygiene → gown → mask/respirator → eye protection → gloves. It is removed in the reverse order, with the most contaminated items (gloves, gown) removed first and hand hygiene performed between each step, ensuring that clean surfaces of PPE contact clean skin.
Safe sharps handling is critical in OG. Key rules: never resheath a used needle by hand (use the single-hand scoop technique or a mechanical resheathing device); immediately place all sharps in a designated sharps container (rigid, puncture-proof, colour-coded yellow); announce 'sharp passing' when handing a sharp instrument; use a neutral zone (kidney tray) for instrument transfer in the operative field.
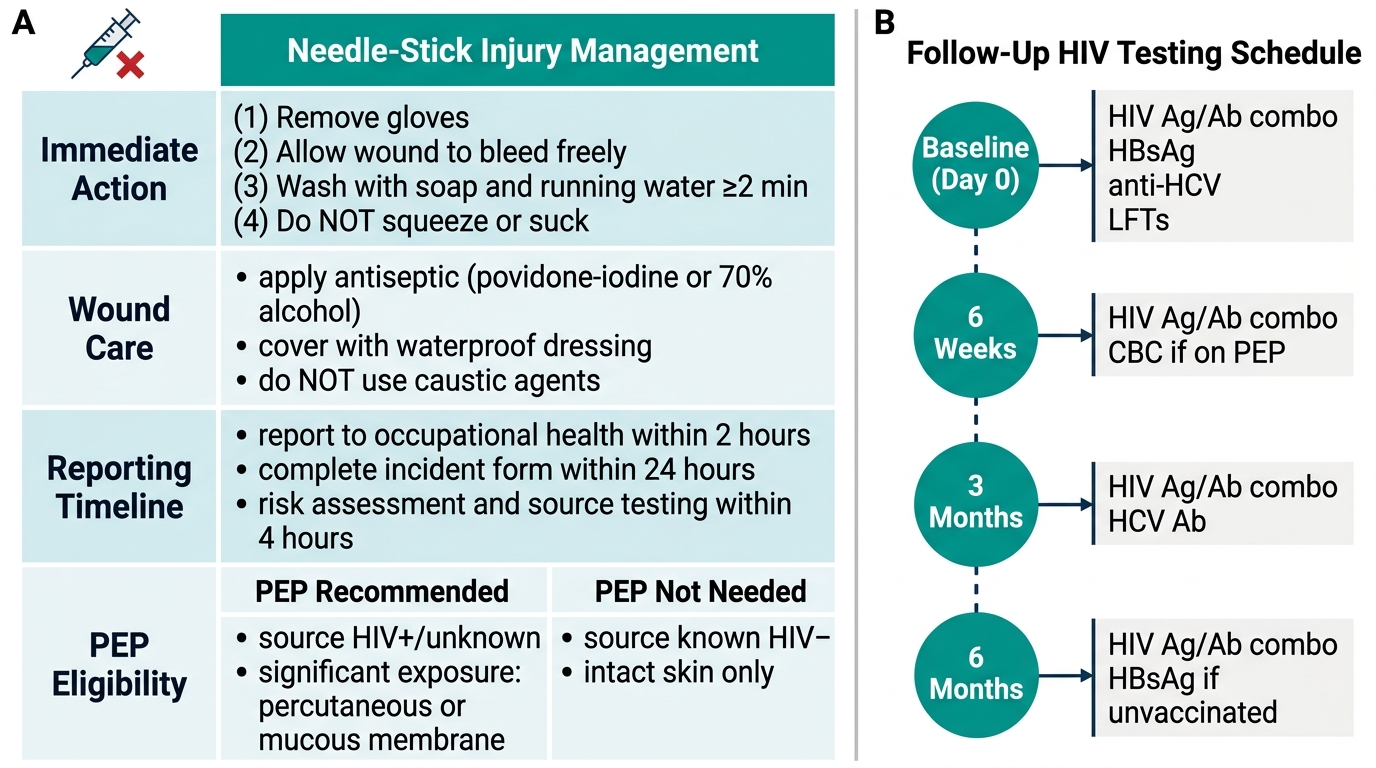
Management of needle-stick or sharps injury:
1. Do not panic; do not suck the wound
2. Immediately squeeze the wound to bleed it freely
3. Wash thoroughly with soap and water for 5 minutes; do not scrub
4. Flush mucous membrane splash with copious water
5. Report to the occupational health officer or duty medical officer within 1 hour
6. The source patient's HIV and hepatitis B/C status must be assessed (with consent)
7. PEP (post-exposure prophylaxis) for HIV must be initiated within 72 hours of exposure (ideally within 2 hours). The standard 28-day regimen per NACO 2014 guidelines: tenofovir 300 mg + lamivudine 300 mg + lopinavir/ritonavir 400/100 mg twice daily. PEP is not indicated if the source is confirmed HIV-negative.
8. For hepatitis B exposure in a non-immune HCW: HBIG (hepatitis B immunoglobulin) within 24 hours + accelerated hepatitis B vaccination.
9. Follow-up HIV testing at baseline, 6 weeks, 3 months, and 6 months after exposure.

Provided image
Needle-Stick Injury: Management Protocol and Follow-Up Schedule
SELF-CHECK
A senior resident sustains a needle-stick injury with a hollow-bore needle while taking blood from an HIV-positive patient. She has been vaccinated against hepatitis B and her anti-HBs titre is >10 mIU/mL. It is currently 11:30 PM. What is the most urgent action she should take?
A. Wait until morning to report to the occupational health officer during business hours
B. Immediately wash the wound, bleed it freely, and report to the duty medical officer within 1 hour for PEP assessment
C. Start hepatitis B immunoglobulin immediately as she is not protected against hepatitis B
D. Complete the incident report form and self-administer the antiviral of her choice
Reveal Answer
Answer: B. Immediately wash the wound, bleed it freely, and report to the duty medical officer within 1 hour for PEP assessment
PEP for HIV must be started within 72 hours of exposure, ideally within 2 hours, to maximise effectiveness. Waiting until morning could exceed the optimal window. The correct first steps are: bleed the wound and wash with soap and water for 5 minutes, then immediately report to the duty medical officer for PEP assessment. She does not need HBIG because her anti-HBs titre of >10 mIU/mL indicates protective immunity from prior vaccination. Self-administration of antivirals without clinical assessment is not appropriate.