Page 17 of 29
OG35.{3,19},OG36.1 | Emergency Recognition and Initial Management — SDL Guide
Learning Objectives
- Recognise clinical situations requiring urgent or emergency treatment at secondary and tertiary centres and make a prompt referral after providing appropriate first-line management
- Diagnose antepartum haemorrhage and distinguish placenta praevia from abruptio placentae on clinical grounds; provide initial emergency management for each
- Diagnose postpartum haemorrhage using the 4 Ts framework, initiate first-line uterotonic treatment with correct drug selection and dosage, and perform uterine massage and bimanual uterine compression in a simulated/guided environment
- Plan and institute a line of treatment in OG emergencies that is need-based, cost-effective, and appropriate for the patient, the disease severity, the socioeconomic context, and the institutional and government guidelines
INSTRUCTIONS
Maternal mortality in India remains a major public health challenge. Two of the three leading direct obstetric causes of maternal death — haemorrhage (postpartum and antepartum) and hypertensive disorders (pre-eclampsia and eclampsia) — are preventable with early recognition and prompt initial management at the first point of contact. This module builds the emergency recognition and first-line management skills you need to act effectively at a primary health centre, district hospital, or tertiary labour ward when these emergencies occur.
References
- Dutta DC. Textbook of Obstetrics. 10th ed. New Central Book Agency; 2023 (textbook)
- Shaw RW et al. Shaw's Textbook of Gynaecology. 17th ed. Elsevier; 2019 (textbook)
- WHO. Recommendations for the Prevention and Treatment of Postpartum Haemorrhage. 2012 (updated evidence 2023) (guideline)
- National Health Mission, India. Facility-Based Newborn Care and Obstetric Emergency Management Protocols. 2020 (guideline)
- FOGSI. Good Clinical Practice Recommendations — Management of Postpartum Haemorrhage. 2020 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 11 PM at a primary health centre in a rural district. The on-call intern, Dr Arjun, receives a 24-year-old primigravida at 38 weeks who was brought in by her mother-in-law. She is pale, sweating, and barely responsive. Her blood pressure is unrecordable. Her pulse is 140 per minute and thready. The mother-in-law says 'she started bleeding one hour after the baby was born at home.' Dr Arjun has never seen a postpartum haemorrhage before. He knows the word 'PPH' from his textbook. But does he know what to do in the next five minutes? Two IV lines, oxytocin, uterine massage, volume resuscitation, and a phone call to the district hospital — in that order, without hesitation. Emergency recognition and first-line management is not theoretical knowledge. It is a practiced skill, and it saves lives.
WHY THIS MATTERS
Haemorrhage (APH and PPH) and hypertensive disorders account for more than 50% of direct maternal deaths in India. Most of these deaths are preventable — not by complex surgery or intensive care, but by early recognition, prompt first-line management, and timely referral. The NMC competencies OG35.3, OG35.19, and OG36.1 address precisely these skills, and they are assessed in DOAP (demonstration, observation, assistance, performance) sessions, skill assessments, OSCE, and clinical assessments in your final examinations. More importantly, as a final-year student and as an intern, you will be the first clinician at the scene of an obstetric emergency in many settings. What you do in the first 15 minutes determines whether the woman survives.
RECALL
Bring to mind what you already know from your obstetrics study. What is the definition of PPH? What is the uterotonic of choice for active management of the third stage of labour? From your pharmacology posting: what is the mechanism of action of oxytocin, and what are its contraindications? What is MgSO₄ used for in obstetrics, and what are the two named regimens — can you recall the Pritchard doses? From your medicine posting: what are the clinical signs of hypovolaemic shock — what happens to the blood pressure, pulse, skin, and mental status as blood loss progresses? And from your surgery posting: what is the ABCDE primary survey? Hold these anchors as we build the OG emergency management framework on them.
Why Emergency Recognition Is the Critical First Step
In obstetrics, the single most important determinant of maternal outcome in an emergency is the time from recognition to first intervention. A woman with a ruptured uterus who arrives at the operating theatre 30 minutes after the diagnosis is made has a survival probability many times higher than one who arrives 90 minutes after the same diagnosis — and the difference is not surgical skill but the speed of recognition, stabilisation, and transfer. Most preventable maternal deaths in India occur not because definitive care was unavailable, but because the emergency was not recognised early enough, or because the decision to refer was delayed.
The barriers to emergency recognition in OG are well-documented. Clinical overconfidence: a 'stable' patient who is compensating haemodynamically may suddenly decompensate when the physiological reserve is exceeded. The normalisation trap: a rapid pulse in late pregnancy can be attributed to physiological changes rather than haemorrhage; a sudden headache in a hypertensive pregnancy can be dismissed as tension headache. The diagnostic delay: the time between first symptoms and clinical action is prolonged when the clinician does not have a structured framework for recognising the emergency constellation.
This module focuses on three emergency presentations that together account for the majority of acute maternal mortality: (1) haemorrhage in pregnancy and the puerperium (APH and PPH); (2) hypertensive emergencies (severe pre-eclampsia and eclampsia); and (3) any obstetric emergency requiring urgent referral. For each, the initial management follows a consistent structure: recognise (identify the emergency constellation), stabilise (ABCDE primary survey and first-line interventions), communicate (call for help and prepare the referral), and transfer (with treatment continuing during transport).
For final-year students and interns, the expected competency level is 'should help' (SH) — performing these skills under supervision — with some elements assessed at DOAP level (demonstration, observation, assistance, performance). The goal is not independent management of these emergencies, but confident first-line action before senior assistance or referral arrives.
ABCDE Primary Survey in Obstetric Emergencies
The ABCDE Framework and Shock Recognition in OG Emergencies
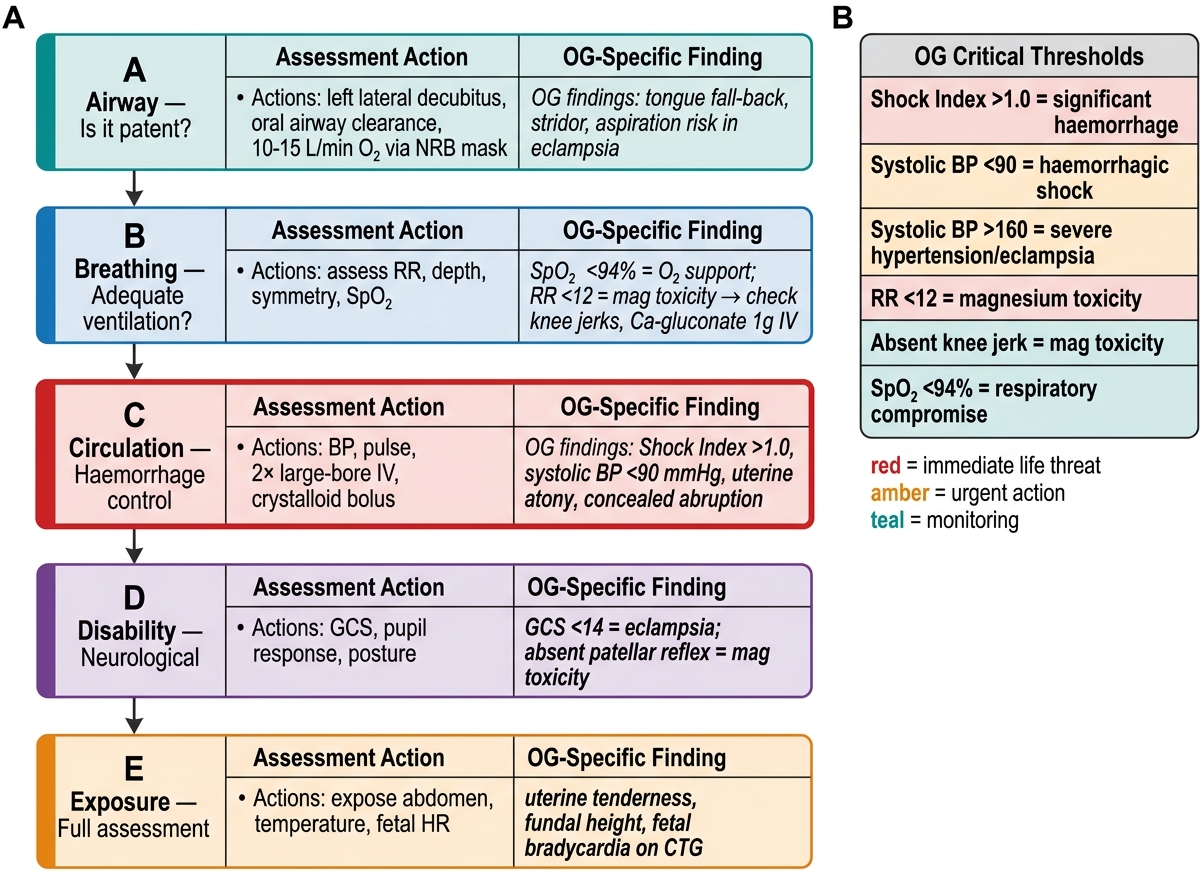
The ABCDE primary survey (Airway, Breathing, Circulation, Disability, Exposure) is the systematic first-response framework for any critically ill patient. In obstetric emergencies, it provides a reproducible structure that prevents the two most common errors: becoming fixated on the obstetric diagnosis before securing the airway and circulation, and missing a concurrent deterioration in a different system.
A — Airway: Is the airway patent? In an eclamptic patient with convulsions, the airway may be compromised by the tongue falling back or by aspiration. Position the patient in the left lateral decubitus (recovery) position; clear the oral airway; apply high-flow oxygen by non-rebreather mask at 10–15 L/min.
B — Breathing: Is the patient breathing adequately? Assess respiratory rate, depth, and symmetry. Oxygen saturation <94% requires supplemental oxygen or airway support. In magnesium toxicity (an important OG-specific cause), respiratory rate <12/min is a pre-arrest warning — check knee jerks and call for calcium gluconate 1 g IV immediately.
C — Circulation: This is the critical step in haemorrhagic emergencies. Assess: blood pressure (systolic <90 mmHg = shock); pulse rate (>100 = tachycardia; >120 = significant haemorrhage); skin (pallor, mottling, cold extremities); capillary refill time (>2 seconds = poor perfusion). The shock index (pulse rate / systolic BP) is a rapid bedside tool: a value >1 indicates significant haemorrhage requiring immediate IV access and volume replacement. Establish two large-bore (14–16 G) IV cannulae; send blood for FBC, cross-match (at least 2 units), coagulation profile, and renal function; initiate IV crystalloid (normal saline or Ringer's lactate) at 1 L over 15–20 minutes while awaiting blood.
D — Disability: Assess the Glasgow Coma Scale (GCS). In pre-eclampsia/eclampsia: check for hyperreflexia (knee jerk), visual disturbance (photophobia, blurred vision), or any altered consciousness. A GCS <14 in a hypertensive patient requires immediate MgSO₄ and urgent referral to a centre with ICU capability.
E — Exposure: Fully expose the patient to assess the extent of bleeding (vaginal, wound, concealed intraperitoneal). In APH: estimate the pad count; palpate the abdomen for uterine tenderness (abruption) vs a painless soft uterus (praevia). In PPH: massage the uterus, assess its tone (atony = boggy, poorly contracted uterus), and inspect the perineum and vagina for lacerations.
Uterotonic agents — key contraindications (MUST be correct):
- Oxytocin 10 IU IM: first-line for all cases; contraindication: rapid IV bolus (causes hypotension and tachycardia — always give as slow IV infusion or IM)
- Misoprostol 800 µg sublingual or rectal: use where oxytocin is unavailable or failed
- Carboprost (PGF2α) 250 µg IM: contraindicated in asthma (causes bronchospasm)
- Ergometrine / methylergometrine 0.2 mg IM or IV slowly: contraindicated in hypertension and pre-eclampsia (causes severe hypertension); also contraindicated in heart disease and Raynaud's
SELF-CHECK
A patient develops PPH following vaginal delivery. She has severe pre-eclampsia with BP 180/110 mmHg. Which uterotonic is contraindicated in this patient?
A. Oxytocin 10 IU IM
B. Misoprostol 800 µg sublingual
C. Carboprost 250 µg IM
D. Ergometrine 0.2 mg IV
Reveal Answer
Answer: D. Ergometrine 0.2 mg IV
Ergometrine (and methylergometrine) is contraindicated in hypertension and pre-eclampsia because it causes severe vasoconstriction, potentially precipitating a hypertensive crisis, stroke, or cardiac arrest. In a patient with PPH and severe pre-eclampsia, the correct uterotonics are oxytocin (first line) and misoprostol (second line). Carboprost is contraindicated in asthma (not hypertension). Oxytocin and misoprostol are safe in hypertensive patients.
Recognising and Initially Managing an Obstetric Emergency
Obstetric emergencies share a fundamental characteristic that distinguishes them from most other medical emergencies: the time window between recognition and irreversible harm is measured in minutes, not hours. A ruptured uterus untreated for 30 extra minutes adds litres of intraperitoneal blood. An eclamptic convulsion that occurs during an unprotected airway aspirates. A PPH that is not attributed to a specific cause — atony, trauma, retained tissue, or coagulopathy — is treated with the wrong intervention. The structured Recognise → Stabilise → Communicate → Transfer sequence applied to every obstetric emergency is therefore not a protocol for convenience; it is a time-critical decision pathway that determines survival. The five emergencies requiring immediate recognition and referral from primary or secondary care settings are: eclampsia, severe antepartum haemorrhage, ruptured uterus, postpartum haemorrhage not responding to initial measures, and severe fetal distress requiring caesarean section. Each is described below with its initial management steps.
Eclampsia: characterised by convulsions (tonic-clonic) in a woman with pre-eclampsia (BP ≥140/90 after 20 weeks, with proteinuria or end-organ dysfunction). Initial management:
1. Call for help immediately; do not leave the patient alone
2. Left lateral position; protect the airway; high-flow oxygen (10–15 L/min, non-rebreather mask)
3. MgSO₄ loading dose — the Pritchard regimen (IM, available at most PHCs): 4 g IV over 10–15 minutes (diluted in 50 mL normal saline) + 10 g IM (5 g deep IM into each buttock); maintenance 5 g deep IM every 4 hours in alternate buttocks. OR the Zuspan regimen (IV): loading 4 g IV over 10–15 min, then 1 g/h IV infusion. The antidote to MgSO₄ toxicity is calcium gluconate 1 g IV (10 mL of 10% solution) — this must be at the bedside at all times.
4. Monitor: knee jerks (loss of patellar reflex = first sign of toxicity — stop MgSO₄), respiratory rate ≥12/min, urine output ≥30 mL/h
5. Antihypertensive for severe-feature BP (≥160/110): labetalol 20 mg IV (repeat 40 mg after 10 min if needed; max 300 mg total), or hydralazine 5 mg IV, or oral nifedipine 10 mg
6. Refer urgently to a centre with ICU and obstetric care capability, with treatment continuing during transfer and a complete referral letter
Ruptured uterus: triad of sudden severe abdominal pain, haemodynamic instability, and loss of fetal heart sounds in a woman with a uterine scar (previous LSCS, myomectomy) or obstructed labour. Initial management: IV access, fluid resuscitation, cross-match blood, Foley catheter, nil by mouth, and immediate referral for emergency laparotomy. Do NOT attempt vaginal examination in suspected complete rupture.
Obstructed labour: failure of descent despite regular uterine contractions; caput, moulding, and a high presenting part that cannot be displaced. Management: IV fluids, Foley catheter, nil by mouth, assess fetal condition, and immediate referral for LSCS.