Page 18 of 29
OG35.{3,19},OG36.1 | Emergency Recognition and Initial Management — SDL Guide (Part 2)
Initial Emergency Management of APH and PPH
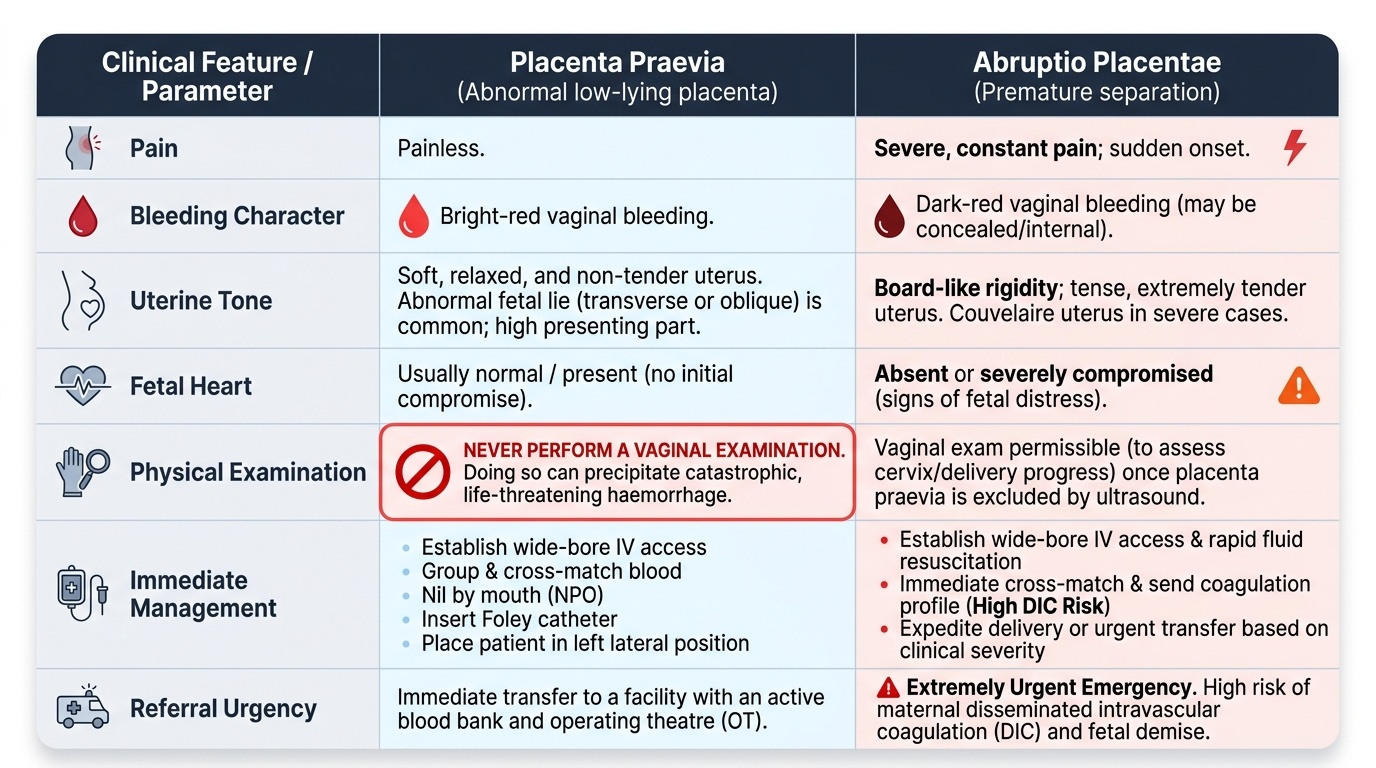
Antepartum haemorrhage (APH) is defined as vaginal bleeding after 20 weeks of gestation (some texts specify 24 weeks as the threshold; state both in your answers). Haemorrhage in pregnancy and the puerperium is the single leading cause of maternal death in India and globally, and rapid clinical differentiation between the two major causes — placenta praevia and abruptio placentae — is critical because the immediate management of each is not only different but in one case (suspected praevia) includes an absolute prohibition on vaginal examination. Getting this distinction right at the first point of contact — primary health centre, emergency OPD, or labour ward — can prevent catastrophic haemorrhage from an inadvertent vaginal examination in a patient with low-lying placenta. The two most important causes requiring immediate recognition and differentiation are placenta praevia (abnormal low-lying placenta) and abruptio placentae (premature separation of a normally situated placenta). The clinical distinction matters not only for immediate management but for the referral decision, the resuscitation approach, and the risk of disseminated intravascular coagulation — which is high in abruption and rare in praevia.
The clinical features and management of each are:
- Placenta praevia: painless, bright-red vaginal bleeding; soft, non-tender uterus; no fetal compromise initially; the fetal lie may be abnormal (transverse, oblique); the presenting part is high. Management: IV access, cross-match, nil by mouth, Foley catheter, left lateral position; never perform a vaginal examination (can precipitate catastrophic haemorrhage); immediate referral to a centre with blood bank and OT facility.
- Abruptio placentae: painful (often board-like uterine rigidity); dark-red bleeding (may be concealed); fetal heart may be absent or severely compromised; pre-eclampsia is often present; Couvelaire uterus in severe cases. Management: IV access, cross-match (DIC is a risk — send coagulation profile), fluid resuscitation, immediate delivery or referral depending on severity.
Postpartum haemorrhage (PPH) is defined as blood loss ≥500 mL after vaginal delivery or ≥1000 mL after caesarean section, or any blood loss causing haemodynamic change. The 4 Ts mnemonic covers all causes:
- Tone (uterine atony): responsible for approximately 80% of PPH; the uterus is boggy, poorly contracted, and large. First-line management: uterine massage; oxytocin 10 IU IM (or 20 IU in 500 mL IV at 60 drops/min); if atony persists add misoprostol 800 µg sublingual; if available and not contraindicated, add carboprost 250 µg IM (avoid in asthma) or ergometrine (avoid in hypertension). Bimanual uterine compression (one hand vaginally, one abdominally): compress the uterus between both hands until it contracts and bleeding stops.
- Trauma: lacerations of the cervix, vagina, or perineum; uterine rupture. Inspect under good light; apply pressure to bleeding points; suture lacerations; refer for uterine rupture.
- Tissue: retained placenta or placental fragments. Inspect the placenta (completeness of membranes and placental disc); if incomplete, manual removal of placenta under anaesthesia.
- Thrombin: coagulopathy (DIC — disseminated intravascular coagulation, most common after abruption, IUFD, amniotic fluid embolism). Manage with fresh frozen plasma, cryoprecipitate, packed red cells, and platelet transfusion; treat the underlying cause.
Simultaneous resuscitation must occur alongside management of the cause: two large-bore IV lines, aggressive IV fluid replacement, early blood transfusion (O-negative in emergency), Foley catheter to monitor urine output, and frequent vital sign monitoring.
Provided image
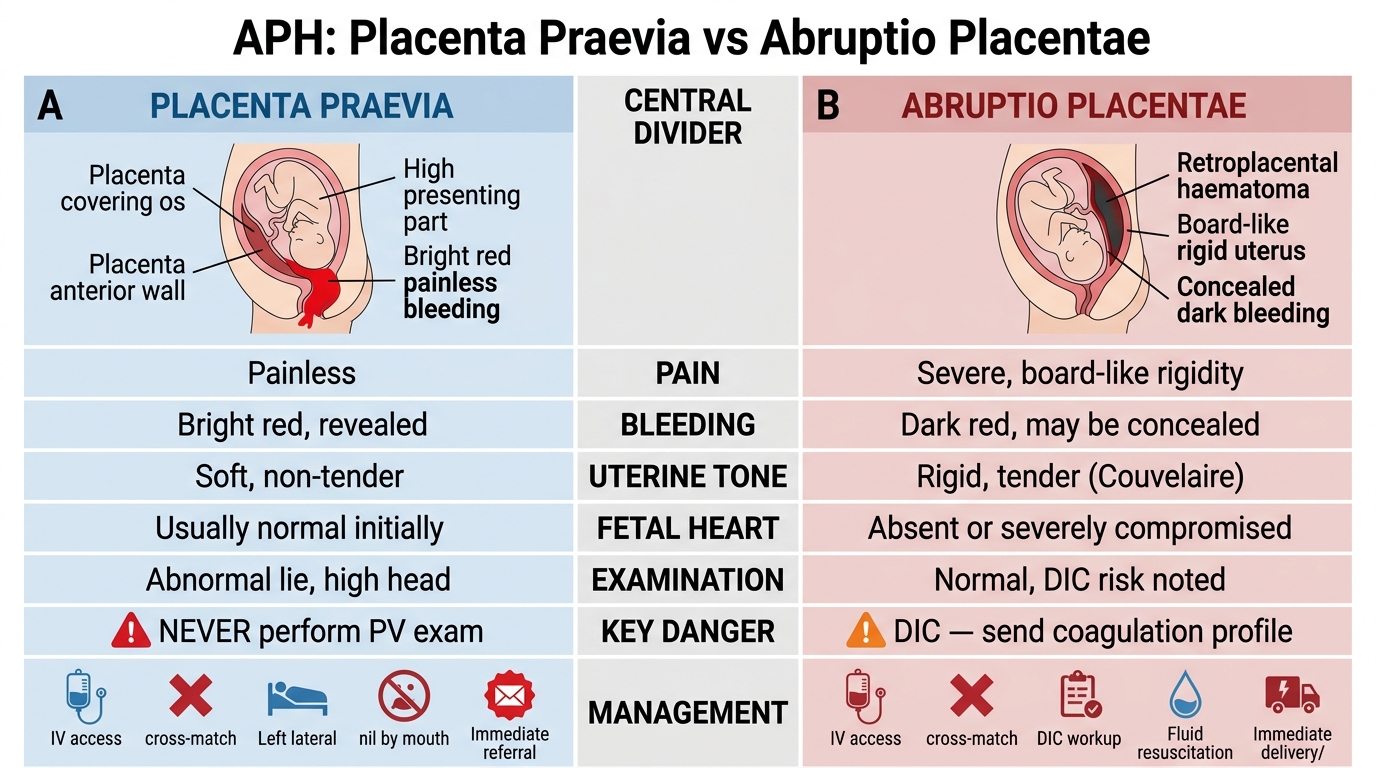
APH: Placenta Praevia vs Abruptio Placentae — Clinical Comparison
SELF-CHECK
A woman delivers vaginally at a PHC and has estimated blood loss of 800 mL with a soft, boggy uterus. The uterus is not contracting with fundal massage alone. What is the next most appropriate step?
A. Immediate blood transfusion and referral without any uterotonic
B. Carboprost 250 µg IM as the first-line uterotonic
C. Oxytocin 10 IU IM (or 20 IU in 500 mL IV) as the first-line uterotonic, with resuscitation and referral preparation
D. Wait for spontaneous contraction before giving any drug
Reveal Answer
Answer: C. Oxytocin 10 IU IM (or 20 IU in 500 mL IV) as the first-line uterotonic, with resuscitation and referral preparation
This is PPH secondary to uterine atony (the 'Tone' T). The first-line uterotonic is oxytocin 10 IU IM (or 20 IU in 500 mL IV at 60 drops/min). Carboprost is a second-line agent and is the first-line choice only if oxytocin and misoprostol have failed, and it is contraindicated in asthma. Blood transfusion is important for resuscitation but does not address the cause (atony). Waiting without uterotonics when there is ongoing haemorrhage is dangerous.
Interpreting Response to Initial Treatment
Interpreting the patient's response to initial emergency management is a critical skill that guides the decision to continue at the current level of care or to escalate immediately. In OG emergencies, an adequate response to first-line treatment provides a window of haemodynamic stability that allows safe transfer; an inadequate response demands immediate escalation.
For PPH, the signs of an adequate response to first-line treatment are: the uterus becomes firm on palpation after massage and uterotonic administration; bleeding reduces to a trickle; haemodynamic parameters improve (pulse rate <100, systolic BP >90, capillary refill <2 seconds). If these signs are not present within 15–20 minutes of correct first-line management, the patient is not responding — escalate the uterotonic regimen, initiate bimanual uterine compression, prepare for transfer, and consider whether DIC is complicating the picture.
For eclampsia, an adequate response to MgSO₄ is defined as no further convulsions after loading dose administration and maintenance of the monitoring parameters (knee jerks present, respiratory rate ≥12/min, urine output ≥30 mL/h). A patient who has a second convulsion after receiving the correct loading dose of MgSO₄ should receive an additional 2–4 g MgSO₄ IV slowly over 5–10 minutes. If convulsions continue despite correct MgSO₄ dosing, consider a differential diagnosis (intracranial bleed, metabolic encephalopathy) and refer to a centre with neurology and imaging capability.
Monitoring during treatment: vital signs (BP, pulse, SpO₂) every 15 minutes; urine output hourly via Foley catheter; GCS every 30 minutes in eclampsia; patellar reflex check before every MgSO₄ maintenance dose. Document everything on a running chart — time, drug given, dose, route, vital signs, urine output — because the receiving tertiary team will use this chart to continue management without interruption.
The documentation principle during an emergency: it feels counterintuitive to stop and write when a patient is crashing. The rule is: one person manages the patient; one person documents in real time. A complete record of the time of events, drugs given and doses, vital signs trend, and the patient's response is not an administrative task — it is part of the patient's management, because it prevents re-dosing errors (especially MgSO₄), guides the receiving team, and is a medicolegal record.
Need-Based, Cost-Effective Treatment Planning in OG Emergencies
OG36.1 requires that you plan and institute treatment that is simultaneously need-based (matched to the severity of the disease), cost-effective (achieves the best outcome within resource constraints), and appropriate (aligned with the patient's values, socioeconomic context, and government guidelines). In OG emergency management, this framework shapes every decision from the first intervention to the referral choice.
Need-based matching: treatment intensity must match the clinical severity. A patient with mild PPH (500–700 mL blood loss, haemodynamically stable, uterus contracting with massage) needs oxytocin and observation — she does not need blood transfusion or immediate theatre. A patient with severe PPH (>1000 mL, haemodynamic instability, failed oxytocin and misoprostol) needs second-line uterotonics, bimanual compression, blood transfusion, and urgent surgical referral. Applying the same protocol regardless of severity wastes resources in mild cases and undertreat severe ones.
Cost-effective sequencing: India's public health system provides a defined package of obstetric emergency drugs and equipment under the National Health Mission (NHM). First-line management should always use the NHM-available drugs (oxytocin, misoprostol, MgSO₄, calcium gluconate, IV fluids) before escalating to more expensive or unavailable second-line options. This is not resource-rationing — it is evidence-based practice, because WHO evidence ranks oxytocin above carboprost for first-line PPH management anyway.
Socioeconomic considerations: in a setting where the patient or family cannot afford cross-matching, rapid initial fluid resuscitation, early transfer to a facility with blood bank capability, and the referral letter documenting the clinical indication for transfusion are the most important actions. Never withhold available first-line treatment pending discussion of cost; document clearly what was given and what was not available.
Government and institutional protocols: national and state NHM obstetric emergency protocols define the treatment algorithm for each PHC and district hospital level. Knowledge of which drugs, which equipment, and which procedures are available at each level — and at what level of care each intervention requires — is the foundation of safe referral practice. A clinician who knows that the district hospital has blood bank, OT, and anaesthesia capability but the sub-centre does not will make a different and more appropriate referral decision than one who assumes capability uniformly.
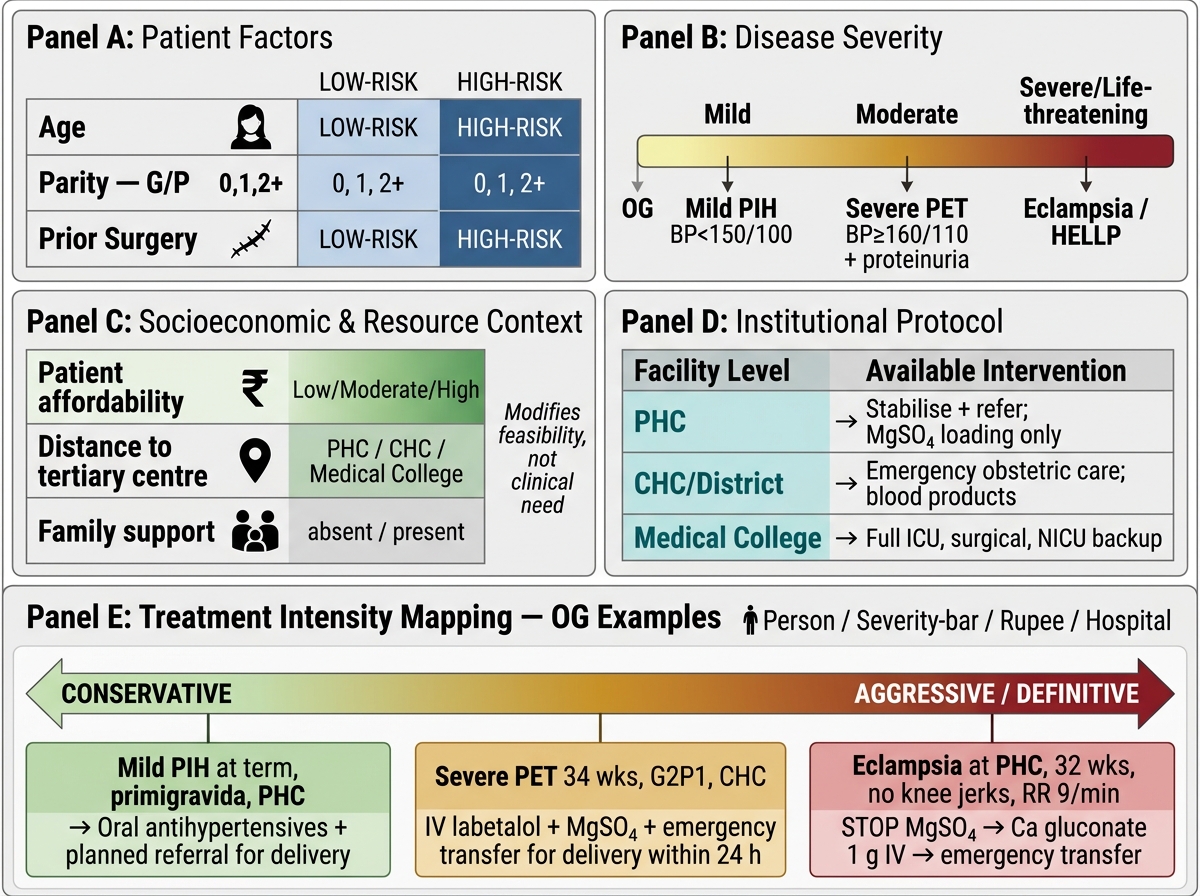
Four-Axis Framework for Need-Based Treatment Intensity in OG Emergencies
SELF-CHECK
At a PHC, a primigravida at 32 weeks presents with an acute convulsion. Her BP is 170/110. She has no knee jerks. A nurse has already given MgSO₄ 4 g IV loading and 10 g IM. Current respiratory rate is 9/min. What is the immediate action?
A. Give the next maintenance dose of MgSO₄ 5 g IM as scheduled
B. Stop MgSO₄ and administer calcium gluconate 1 g IV immediately; monitor closely
C. Increase the MgSO₄ infusion rate to control the convulsions
D. Give diazepam 10 mg IV as an alternative anticonvulsant
Reveal Answer
Answer: B. Stop MgSO₄ and administer calcium gluconate 1 g IV immediately; monitor closely
A respiratory rate of 9/min (below the threshold of 12/min) is a sign of MgSO₄ toxicity. Loss of patellar reflex (knee jerk) is typically the first sign; respiratory depression follows. The immediate action is to stop the MgSO₄ infusion and give calcium gluconate 1 g IV (10 mL of 10% solution) slowly over 10 minutes — this is the specific antidote for MgSO₄ toxicity. Giving more MgSO₄ in the context of toxicity will cause respiratory arrest. Diazepam is not the correct anticonvulsant for eclampsia in this context.
CLINICAL PEARL
Three rules that prevent the most common emergency management errors in OG: (1) Ergometrine is contraindicated in hypertension/pre-eclampsia; carboprost is contraindicated in asthma — know these two contraindications before you pick up a uterotonic. (2) In MgSO₄ management, the three monitoring parameters are non-negotiable: knee jerks present, respiratory rate ≥12/min, urine output ≥30 mL/h; if any one is absent, check for toxicity before the next dose. (3) Placenta praevia = never perform a vaginal examination — the examination can trigger catastrophic haemorrhage from a low-lying placenta.