Page 1 of 29
OG35.{1-2,8,11} | History, Examination and Provisional Diagnosis — SDL Guide
Learning Objectives
- Obtain a logical, humane, and thorough obstetric and gynaecological history, including obstetric formula (GPAL/TPAL), menstrual, marital and contraceptive histories.
- Perform a systematic general, systemic, and obstetric abdominal examination — including fundal height measurement, Leopold's manoeuvres, and fetal heart auscultation — excluding per-rectal and per-vaginal examinations.
- Synthesise history and examination findings to arrive at a logical provisional diagnosis.
- Determine gestational age, EDD (by Naegele's rule), and obstetric formula from available data.
- Write a complete, well-structured case record with all necessary details.
INSTRUCTIONS
This module prepares you for supervised bedside practice in obstetrics and gynaecology. Clinical communication, consent, and humane examination are as important as technique. Work through each section before your clinic posting; return to the Leopold's manoeuvres and EDD calculation sections for hands-on reinforcement.
References
- DC Dutta's Textbook of Obstetrics, 9th edition — Ch. 3 (Diagnosis of Pregnancy), Ch. 4 (Antenatal Care), Ch. 7 (Obstetrical Examination) (textbook)
- Shaw's Textbook of Gynaecology, 17th edition — Ch. 1 (History and Examination in Gynaecology) (textbook)
- NMC 2024 CBME Competency Framework — OG35 (Clinical and Procedural Skills) (reference)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 26-year-old woman, gravida 2 para 1, presents to the antenatal clinic at 34 weeks of gestation complaining of reduced fetal movements over the past 24 hours. The on-call intern approaches her bed, introduces herself, draws the curtain — and then is uncertain where to begin. Should she start with the fetal heart, the fundal height, or the history? Does the last menstrual period match the current fundal height? Is the obstetric formula correctly determined? Without a systematic approach, vital information is missed, errors cascade, and a potentially compromised fetus may not be identified in time. The structured obstetric clinical encounter — history first, examination second, synthesis third — is not a bureaucratic formality. It is the clinical reasoning scaffold that turns a ward encounter into a safe clinical decision.
WHY THIS MATTERS
Competency OG35 spans the full clinical encounter: history (OG35.1), provisional diagnosis (OG35.2), gestational-age and EDD determination (OG35.8), and case-record writing (OG35.11). These are SH (should perform under supervision) competencies — meaning you are expected to actually do them at the bedside, not merely describe them. In the NMC 2024 Miller's Pyramid framework, SH sits at 'shows how': you perform the skill under a supervisor's observation and receive formative feedback. Errors in history-taking translate directly to missed diagnoses (placenta praevia mistaken for labour, ectopic pregnancy missed because LMP was not verified) and to documentation failures that compromise patient safety and medico-legal defence. Every clinical encounter you lead in this posting is an opportunity to practise and be assessed on these competencies.
RECALL
Before proceeding, bring to mind what you already know:
- Pelvic anatomy (AN): the bony pelvis (sacrum, coccyx, iliac bones, pubic symphysis), the uterus and its relations, the round ligament, and the position of the bladder and rectum.
- Reproductive physiology (PY): the menstrual cycle (follicular and luteal phases, average 28 days), ovulation on day 14 of a 28-day cycle, fertilisation, and implantation.
- Clinical reasoning: the general structure of a medical history — presenting complaint, history of presenting illness, past medical/surgical history, family history, social history. OG adds layers: menstrual, obstetric, marital, and contraceptive histories.
- Vital signs interpretation: normal ranges for blood pressure, pulse, temperature, and respiratory rate in a non-pregnant adult; recall that pregnancy modifies these norms (BP falls in mid-trimester; heart rate increases ~10–15 bpm).
Why Systematic History and Examination Matter in OG
The obstetric and gynaecological clinical encounter is fundamentally different from a general medicine clerking, and understanding why it differs is the first step toward performing it competently. In obstetrics, you are simultaneously caring for two patients — the mother and the fetus — whose wellbeing may at times be in tension. A missed pregnancy complication (antepartum haemorrhage, pre-eclampsia, fetal growth restriction) can result in maternal or perinatal death; the clinical encounter is the front-line safety net. In gynaecology, the history uncovers conditions that range from benign but distressing (uterine fibroids, dysfunctional uterine bleeding) to immediately life-threatening (ectopic pregnancy rupture, cervical cancer). A systematic approach — the same sequence every time — prevents cognitive shortcuts that skip important questions.
The obstetric encounter centres on the current pregnancy: gestational age, fetal wellbeing, maternal complications, and the trajectory toward delivery. The gynaecological encounter centres on symptoms relating to the female reproductive tract: abnormal bleeding, pelvic pain, vaginal discharge, prolapse, or infertility. While both require a full general medical history, the disease-specific extensions — menstrual history, obstetric history, marital and contraceptive history — are unique to this specialty and must never be abbreviated.
There are also ethical and legal dimensions to every OG encounter that do not apply with the same urgency elsewhere. The patient's right to privacy and dignity demands a curtained or private space, a chaperone (a nurse or female staff member present whenever a male clinician examines a female patient — and considered good practice regardless of gender), and explicit, informed consent before any examination. Failure to obtain consent, or to arrange a chaperone, is not merely impolite — it is a clinical governance failure and a source of formal complaints and litigation. These principles are taught as governing principles in Step 2, but their clinical motivation — why they are not optional — is established here.
Finally, the provisional diagnosis that emerges from this encounter drives every subsequent decision: investigations ordered, speciality referrals made, treatment initiated. An incomplete or inaccurate history yields an incorrect provisional diagnosis; an incorrect provisional diagnosis drives unnecessary or harmful investigations and delayed treatment. The investment of 10–15 minutes in a thorough, structured history and examination pays dividends in patient safety and clinical efficiency that far outweigh the time spent.
SELF-CHECK
A 22-year-old patient presents to the gynaecology OPD with pelvic pain. The intern begins the examination without introducing herself or seeking the patient's consent. Which principle of the OG clinical encounter has been violated?
A. Obstetric formula documentation
B. Informed consent and humane examination
C. Calculation of EDD by Naegele's rule
D. Fundal height measurement technique
Reveal Answer
Answer: B. Informed consent and humane examination
Informed consent and the principle of humane examination (including introduction, consent, chaperone, and privacy) must precede any clinical examination in obstetrics and gynaecology. This is both an ethical obligation and a clinical governance requirement. The other options describe procedural skills relevant to obstetric examination and documentation, but none is the principle violated here.
Anatomy Review and Principles of the OG Encounter
A confident examination begins with a confident grasp of surface anatomy. The non-pregnant uterus is a pear-shaped, anteverted, anteflexed organ lying in the lesser pelvis, with its fundus pointing upward and forward, its body lying on the superior surface of the bladder, and its cervix projecting into the vagina. In pregnancy, as the uterus enlarges from within the pelvis, its fundus rises progressively above the symphysis pubis — a predictable anatomical relationship that underpins the clinical method of fundal height measurement.
Key surface landmarks used in obstetric abdominal examination include the symphysis pubis (the bony anterior midline junction of the pubic bones, palpable just above the mons pubis), the umbilicus (at approximately the level of the fourth lumbar vertebra in a non-pregnant adult), and the xiphisternum (the inferior tip of the sternum). The fundus of the pregnant uterus rises approximately one finger-breadth per week from the symphysis pubis toward the umbilicus during the first half of pregnancy, and continues to the xiphisternum at approximately 36 weeks, descending slightly at term as engagement occurs.
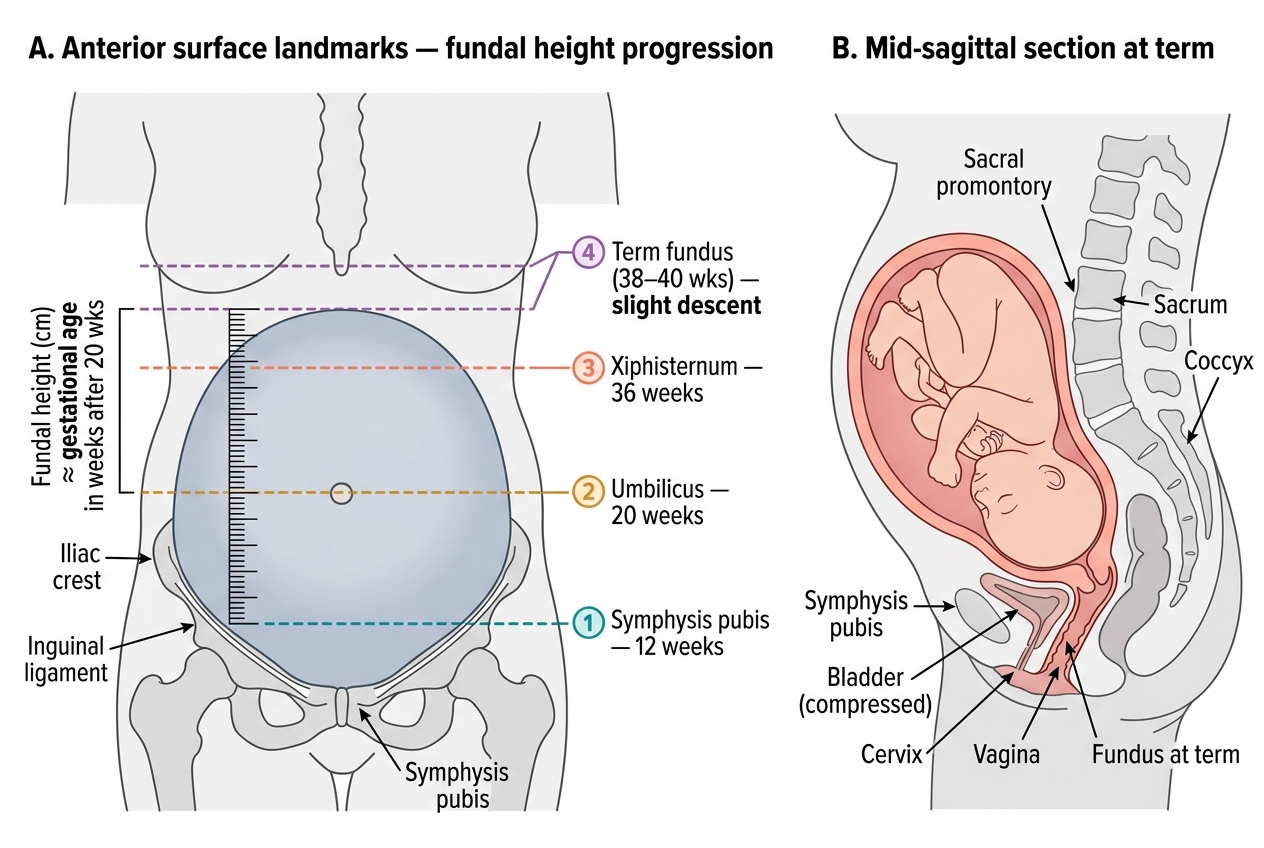
Surface Landmarks for Fundal Height Assessment and Sagittal Pelvic Anatomy at Term
The structure of the obstetric history maps onto these anatomical and physiological realities. It begins with the chief complaint and history of presenting illness, then extends through:
- Menstrual history: last menstrual period (LMP) — date, certainty, regularity of cycle; usual cycle length and duration of flow; abnormal features (dysmenorrhoea, intermenstrual bleeding).
- Obstetric history (GPAL formula): G = Gravida (total number of pregnancies including the present one); P = Para (number of deliveries at or beyond 28 weeks of gestation, regardless of fetal outcome); A = Abortus (number of pregnancy losses before 28 weeks, including spontaneous and induced); L = Living (number of children currently alive). A variant — TPAL — subdivides Para into Term (≥37 weeks), Preterm (28–<37 weeks), Abortus (<28 weeks), Living.
- Marital history: marital status, duration of marriage; relevant for understanding social support and certain disease risk factors.
- Contraceptive history: current or recent method, duration of use, compliance — critical for assessing risk of unintended pregnancy or contraceptive failure complications.
The principles of a humane OG encounter are not optional refinements — they are the baseline standard of care. Consent must be sought before every examination: explain what you will do, why it is necessary, and ask the patient's permission. A chaperone (a trained female staff member) must be present for all intimate examinations, regardless of the examining clinician's gender — this protects both patient and clinician. Universal precautions (gloves, hand hygiene) apply to every physical contact. The patient should be positioned, draped, and examined in a private space with dignity maintained throughout.
Taking a Complete Obstetric and Gynaecological History
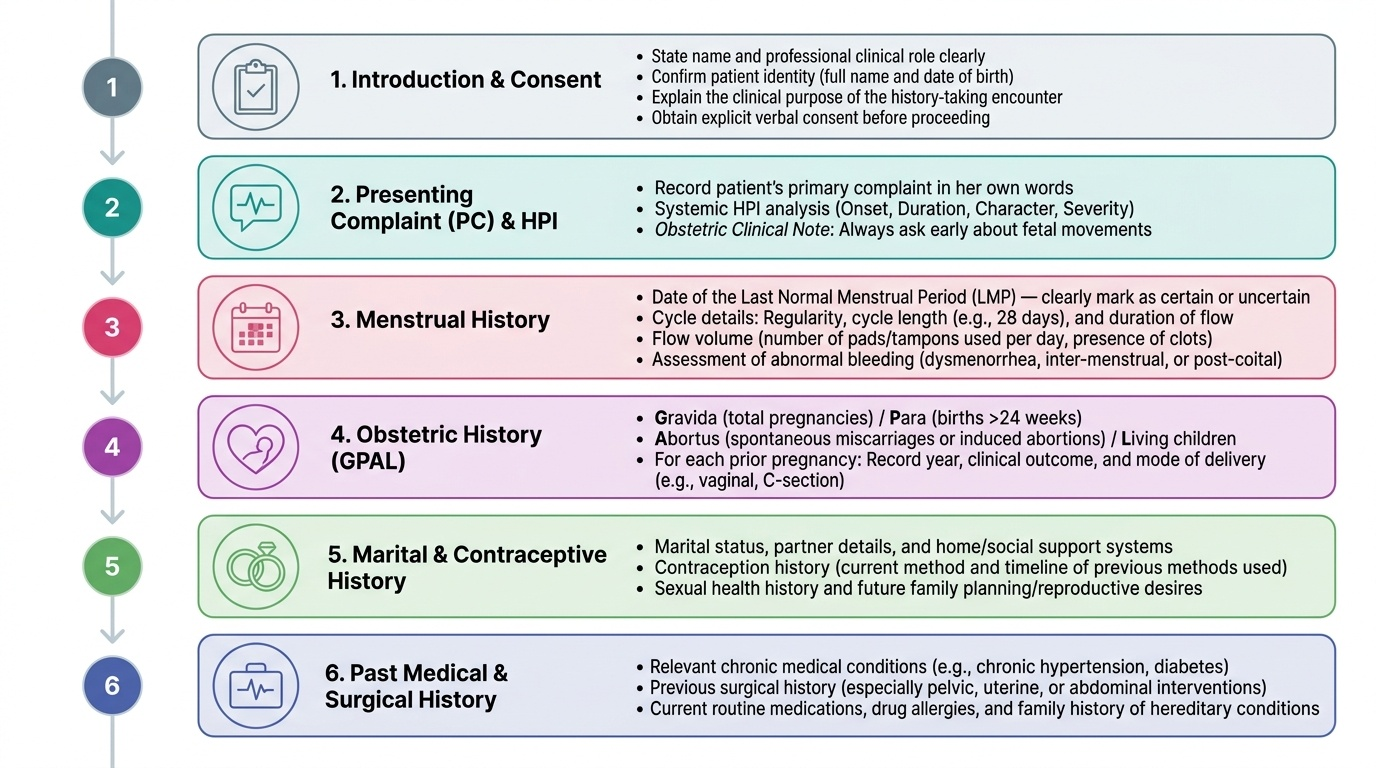
Provided image
History-taking in obstetrics and gynaecology follows a logical sequence that has been refined over a century of clinical practice into a structure that minimises omissions and maximises diagnostic yield. The sequence is not arbitrary — it mirrors the clinical reasoning process, moving from the patient's current concern, to the reproductive context, to general health background.
Begin with a structured introduction: state your name and role, confirm the patient's identity, explain the purpose of the encounter, and obtain verbal consent to proceed. This is not merely social courtesy — it establishes the therapeutic relationship and the patient's willingness to disclose sensitive reproductive history.
1. Presenting complaint (PC) and history of presenting illness (HPI): Ask the patient in her own words what has brought her in. Explore the HPI systematically: onset, duration, character, severity, radiation (for pain), aggravating/relieving factors, associated symptoms, and functional impact. In obstetric patients, always ask about fetal movements early.
2. Menstrual history: Record the date of the LMP (the first day of the last normal menstrual period), cycle regularity (regular/irregular), cycle length (e.g. 28 days, 35 days), duration of flow, flow volume (pads per day, clots), and any abnormal features (dysmenorrhoea, inter-menstrual or post-coital bleeding). The LMP is the cornerstone of gestational-age dating and must be recorded with certainty or flagged as uncertain.
3. Obstetric history (GPAL): For each previous pregnancy, record the year, outcome (term normal delivery, preterm, abortion — spontaneous or induced, ectopic), mode of delivery (SVD, instrumental, caesarean section), birthweight, neonatal outcome, and any complications. The obstetric formula is then written as: G_P_A_L_ (e.g. G3 P2 A0 L2 for a woman with 3 pregnancies, 2 deliveries, 0 abortions, 2 living children — including the current pregnancy in G).
4. Marital history: Duration of marriage, current marital status, partner's health (relevant to STI risk and fertility).
5. Contraceptive history: Current or previous method (IUCD, OCP, barrier, sterilisation), duration of use, any problems or complications.
6. Past medical, surgical, and obstetric history: Chronic conditions (hypertension, diabetes mellitus, thyroid disease, anaemia), prior abdominal or pelvic surgeries, previous gynaecological procedures (LEEP, D&C).
7. Family history: Hypertensive disorders of pregnancy, gestational diabetes, multiple pregnancies, chromosomal disorders.
8. Personal and social history: Occupation, living conditions, smoking, alcohol, substance use, dietary habits, travel.
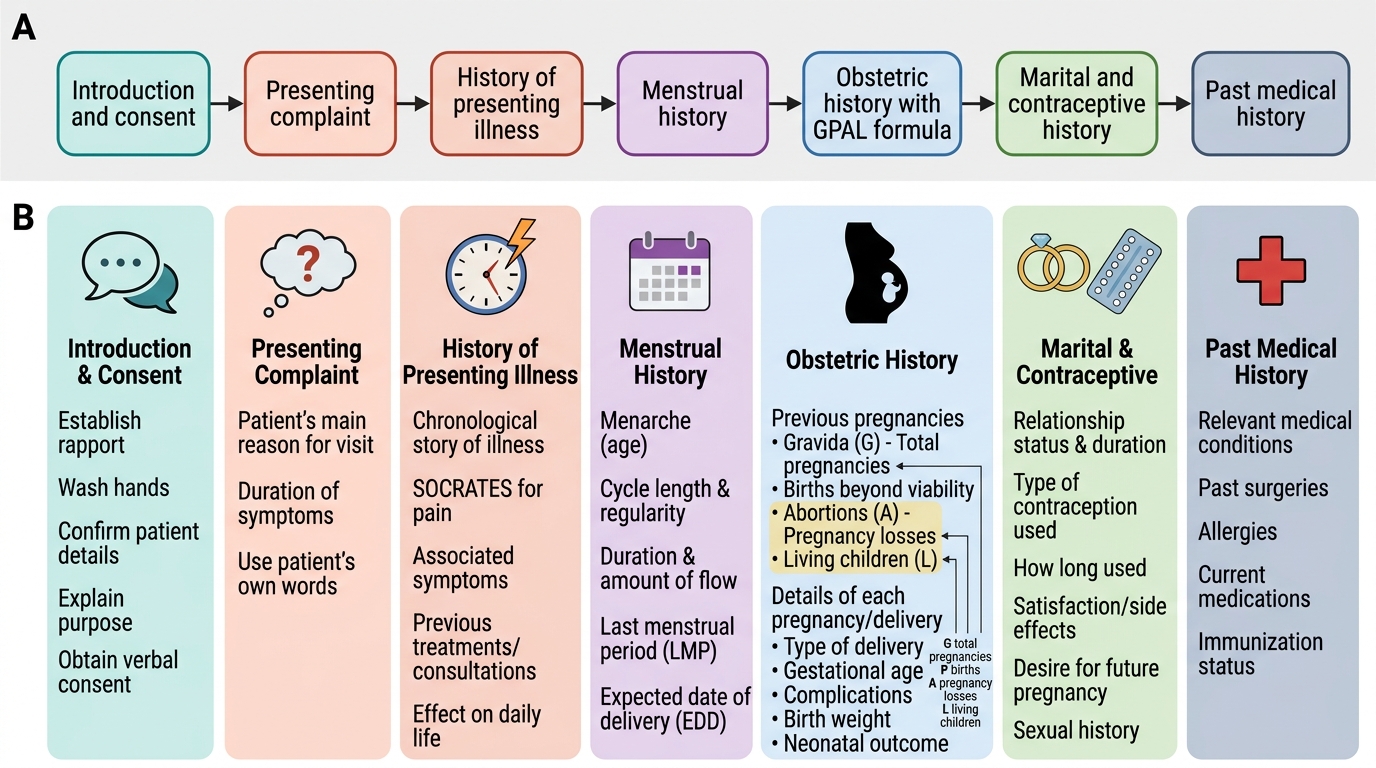
Structured Obstetric History-Taking Flow
| Letter | Meaning | What to record | Example |
|---|---|---|---|
| G | Gravida | Total pregnancies (including present) | G3 |
| P | Para | Deliveries ≥28 weeks (alive or stillborn) | P1 |
| A | Abortus | Losses <28 weeks (spontaneous + induced) | A1 |
| L | Living | Children currently alive | L1 |
TPAL variant: T = Term deliveries (≥37 weeks), P = Preterm deliveries (28–<37 weeks), A = Abortus, L = Living. Both notations are in common use; know the convention of your institution.
A practical note: the obstetric formula includes the current pregnancy in the gravida count but NOT in para (she is not yet para until this delivery is complete). A primigravida in her first pregnancy is G1 P0 A0 L0.
SELF-CHECK
A woman presents at 32 weeks of gestation. She has had 3 previous pregnancies: one term normal delivery (baby alive), one caesarean section at 38 weeks (baby died on day 3), and one spontaneous abortion at 10 weeks. Including the current pregnancy, what is her correct obstetric formula?
A. G3 P2 A1 L1
B. G4 P2 A1 L1
C. G4 P3 A1 L1
D. G3 P2 A1 L2
Reveal Answer
Answer: B. G4 P2 A1 L1
Gravida includes ALL pregnancies including the current one, so G = 4 (3 previous + current). Para = deliveries at or beyond 28 weeks = 2 (term SVD + caesarean at 38 weeks; the spontaneous abortion at 10 weeks does not count as a para). Abortus = 1 (spontaneous abortion at 10 weeks). Living = 1 (only the first baby survived; the caesarean baby died). Therefore G4 P2 A1 L1.