Page 2 of 29
OG35.{1-2,8,11} | History, Examination and Provisional Diagnosis — SDL Guide (Part 2)
General, Systemic and Abdominal Examination
The physical examination in obstetrics and gynaecology follows the classic medical hierarchy — general examination → systemic examination → special (obstetric or gynaecological) examination — but with discipline-specific elaborations that require separate training and practice.
General examination assesses the patient at first glance and by initial contact. Record: build and nutrition (thin/average/obese), pallor (mucous membranes, conjunctivae — to detect anaemia), icterus, cyanosis, clubbing, koilonychia (iron deficiency anaemia commonly accompanies obstetric complications), lymphadenopathy, oedema (pedal, sacral — physiological ankle oedema is common after 28 weeks; severe generalised oedema suggests pre-eclampsia). Vital signs: blood pressure (position and timing standardised), pulse rate and rhythm, respiratory rate, and temperature.
Systemic examination briefly covers cardiovascular (heart sounds, murmurs — common in pregnancy due to high-flow state), respiratory, and central nervous systems. Note any findings relevant to pregnancy complications (hypertensive retinopathy, hepatosplenomegaly in liver disease).
Obstetric abdominal examination — the centrepiece of the encounter — follows a strict sequence: Inspect → Palpate → Auscultate.
Inspection: Expose the abdomen from xiphisternum to symphysis pubis with appropriate draping. Note the size and shape of the uterus, the linea nigra, striae gravidarum, fetal movements, surgical scars, and signs of multiple pregnancy.
Fundal height measurement: With the patient supine, place the zero end of a non-elastic tape at the upper border of the symphysis pubis and measure to the fundus (uppermost palpable edge of the uterus) in centimetres. After 20 weeks, fundal height in centimetres ≈ gestational age in weeks (±2 cm). Discordance >4 cm warrants investigation.
Leopold's manoeuvres are four sequential abdominal palpation grips that determine the lie, presentation, position, attitude, and degree of engagement of the fetus. The examiner stands on the patient's right side (for manoeuvres 1–3) and faces her feet (for manoeuvre 4). Warm hands, gentle pressure.
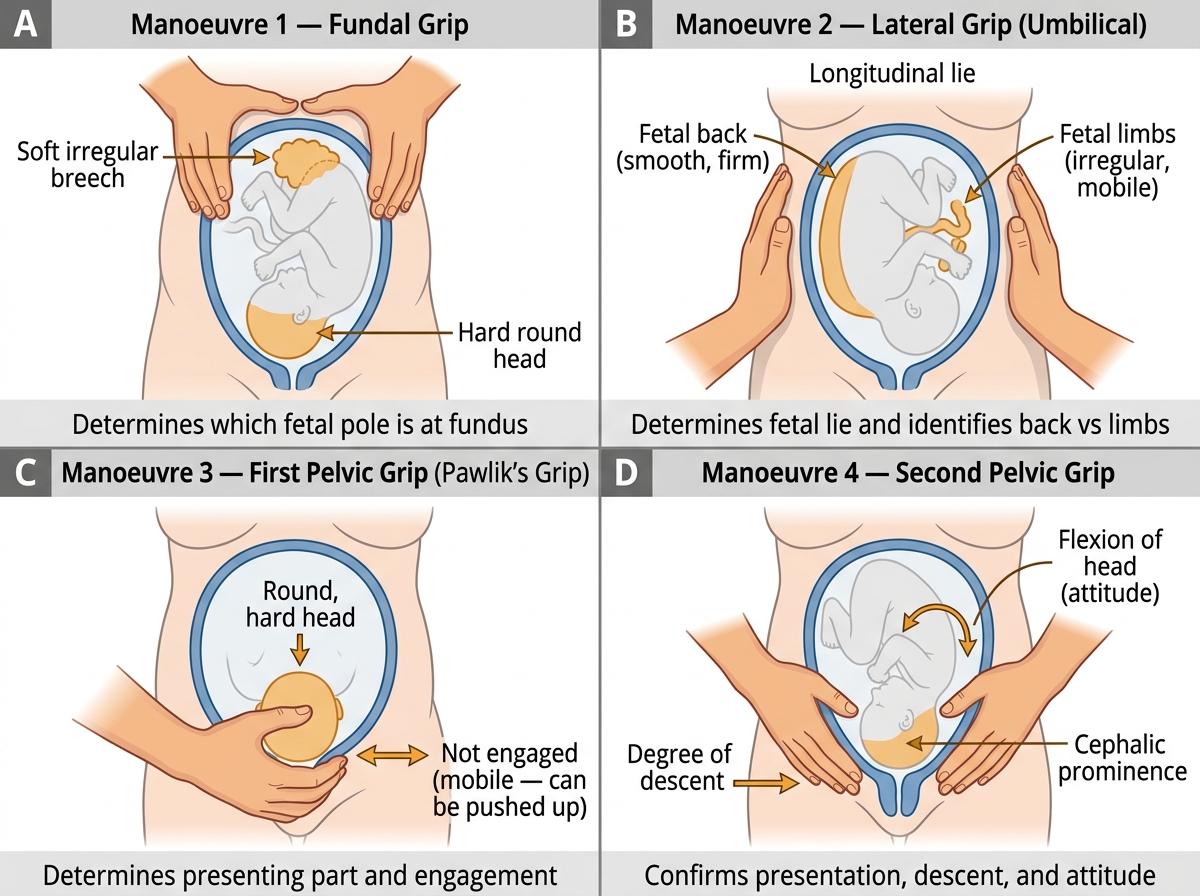
Leopold's Four Manoeuvres of Obstetric Abdominal Examination
| Manoeuvre | Position | Technique | Information obtained |
|---|---|---|---|
| 1. Fundal grip | Examiner faces patient's head | Both hands cup the fundus | Determines which fetal pole occupies the fundus (soft irregular breech vs hard round head) |
| 2. Lateral grip (Umbilical) | Examiner faces patient's head | Palms placed on each side of the uterus, one steady while the other ballots | Determines fetal lie (longitudinal/transverse/oblique); identifies the fetal back (smooth, firm) vs limbs (irregular, mobile) |
| 3. First pelvic grip (Pawlik's grip) | Examiner faces patient's head | Thumb and fingers grasp the lower pole just above symphysis | Determines the presenting part (head vs breech) and its mobility — can it be pushed up (not engaged)? |
| 4. Second pelvic grip | Examiner faces patient's FEET | Both hands applied to the sides of the lower uterus, fingers pointing downward toward the pelvis | Determines the degree of descent/engagement of the presenting part; fingers meet below the presenting part if engaged |
Fetal heart auscultation: The fetal heart is best heard over the fetal back (located by the lateral grip). Use a Pinard's stethoscope (direct placement on maternal abdomen) or a Doppler sonicaid. Normal fetal heart rate: 110–160 bpm. Count for 60 seconds after a fetal movement. Document rate and rhythm.
Liquor volume assessment: Clinically estimated by palpation — uterus feels tense and the fetus is difficult to palpate in polyhydramnios; the uterus is small for dates and the fetus is easily palpable in oligohydramnios. Accurate quantification requires ultrasound.
Gynaecological abdominal examination in non-pregnant patients follows the same general sequence. Uterine size and mobility, adnexal masses, and peritoneal tenderness are assessed by palpation. Percussion may reveal ascites.
Per-rectal (PR) and per-vaginal (PV) examinations are explicitly EXCLUDED from OG35.1 — they are addressed in separate competencies. Students should be aware these examinations exist and are standard components of the full OG examination, but should not attempt them without specific training and direct supervision.
SELF-CHECK
During Leopold's manoeuvres, the third manoeuvre (Pawlik's grip) is performed. The examiner grasps the lower pole and finds a firm, hard, round, ballotable mass that can be pushed upward. What do these findings indicate?
A. Breech presentation with the buttocks not yet engaged
B. Cephalic presentation with the head not yet engaged
C. Transverse lie with the shoulder as presenting part
D. Cephalic presentation with the head engaged
Reveal Answer
Answer: B. Cephalic presentation with the head not yet engaged
Pawlik's grip (first pelvic grip) grasps the presenting part just above the symphysis pubis. A firm, hard, round, ballotable (movable) mass that can be displaced upward indicates the head (vertex) as the presenting part, and the ability to push it upward means it has NOT yet entered (descended into) the pelvis — i.e. it is not engaged. If engaged, the head would be fixed and could not be moved. A breech would feel soft and irregular. A transverse lie would show no clear presenting part at the lower pole.
Interpreting Findings: Provisional Diagnosis, Gestational Age, EDD and Obstetric Formula
The synthesis phase of the clinical encounter — transforming raw history and examination findings into a provisional diagnosis and a coherent clinical impression — is the cognitive skill that distinguishes a trained clinician from a data-recorder. It requires you to integrate information across multiple domains simultaneously: the patient's story, the physical signs, and the gestational-age calculations.
The provisional diagnosis (OG35.2) is formulated as: patient identity + obstetric formula + gestational age + presentation + fetal status + primary clinical problem. For example: G2 P1 A0 L1 at 34 weeks of gestation with a vertex presentation, engaged head, good fetal heart rate, presenting with reduced fetal movements — provisional diagnosis: fetal movement reduction at 34 weeks; rule out fetal growth restriction and cord compromise. The provisional diagnosis is called 'provisional' precisely because it is a working hypothesis that will be tested by investigations; it must be honest about uncertainty and guide the next step rather than close it.
Gestational age determination (OG35.8) from the LMP is the standard first-line method when the LMP is known and the cycle is regular. Count the number of completed weeks and days from the first day of the LMP to the date of examination. Gestational age is expressed in weeks + days (e.g. 34+3 = 34 weeks and 3 days). Fundal height provides a corroborating clinical estimate after 20 weeks.
Naegele's rule for EDD (Expected Date of Delivery / Estimated Date of Confinement, EDC):
> EDD = LMP + 1 year − 3 months + 7 days
This formula is mathematically equivalent to adding 280 days (40 weeks) to the LMP, which reflects the average human gestation from LMP. The rule assumes a regular 28-day menstrual cycle with ovulation on day 14. If the cycle is longer (e.g. 35 days), add the difference in days to the calculated EDD (e.g. add 7 days for a 35-day cycle). If the cycle is shorter (e.g. 21 days), subtract the difference.
EDD by Naegele's Rule: Worked Example, Trimester Timeline, and Fundal Height Milestones
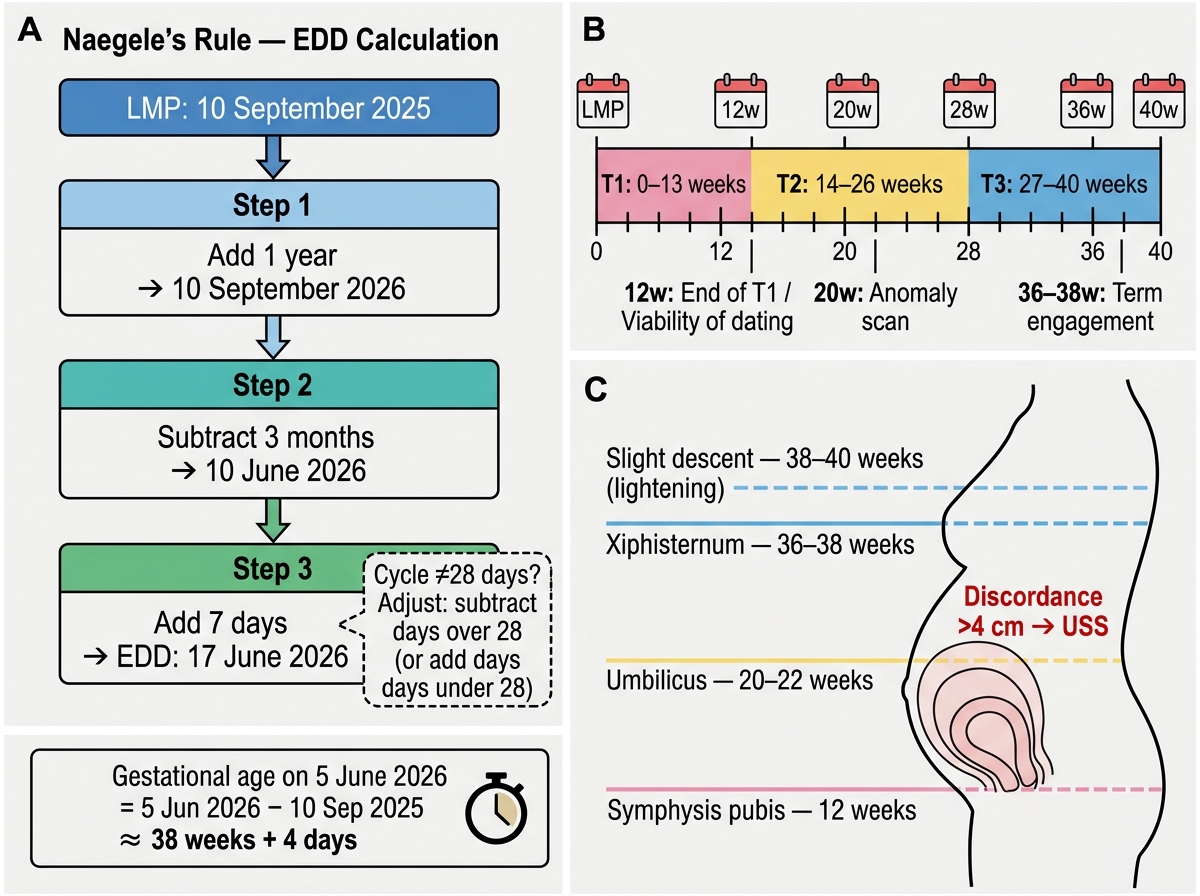
Worked example: LMP = 10 September 2025, regular 28-day cycle.
- Step 1: Add 1 year → 10 September 2026
- Step 2: Subtract 3 months → 10 June 2026
- Step 3: Add 7 days → 17 June 2026 (EDD)
- At examination on 5 June 2026: gestational age = (date of exam) − (LMP) = 5 June 2026 − 10 September 2025 = approximately 38 weeks + 4 days
Ultrasound dating is preferred when the LMP is uncertain, the cycle is irregular, or there is a discrepancy of >2 weeks between LMP-based and fundal-height-based estimates. First-trimester crown-rump length (CRL) is the most accurate dating method.
Fundal height–gestational age correlation: After 20 weeks, fundal height in centimetres approximates gestational age in weeks. The uterus is typically at the symphysis pubis at 12 weeks, at the umbilicus at 20–22 weeks, at the xiphisternum at 36–38 weeks, and descends slightly at 38–40 weeks as the head engages (lightening). Discordance >4 cm between fundal height and dates should prompt ultrasound assessment for fetal growth restriction, macrosomia, polyhydramnios, or oligohydramnios.
Constructing the obstetric formula summary: Having confirmed the GPAL formula from the history and the gestational age from the LMP (and fundal height), write a composite clinical summary line — this is the opening statement of the obstetric case record: e.g. "Mrs XYZ, 28 years, G3 P1 A1 L1, at 36 weeks of gestation by LMP (EDD 17 June 2026), admitted with — "
Supervised Bedside Practice and Case Record Writing
The transition from reading about clinical examination to performing it under supervision is the most critical step in achieving SH-level competence. At the bedside, you are not merely going through a checklist — you are practising a professional act that requires physical skill, cognitive integration, and interpersonal sensitivity simultaneously. Supervised bedside practice in OG follows a structured apprenticeship model: observe once, perform under supervision, perform independently with supervision available.
During supervised practice, your supervisor will observe and provide real-time feedback on: (1) your technique for each Leopold's manoeuvre — hand placement, pressure, sequence, interpretation; (2) your approach to the patient — communication, consent, positioning, draping, respect for dignity; (3) the accuracy and completeness of your clinical findings; (4) the logic of your provisional diagnosis synthesis. Active engagement — asking clarifying questions, articulating your findings aloud as you examine — accelerates skill acquisition more than passive observation.
Writing the complete case record (OG35.11) is the written consolidation of the clinical encounter. A complete OG case record includes all sections listed below; omission of any section is a documentation failure.
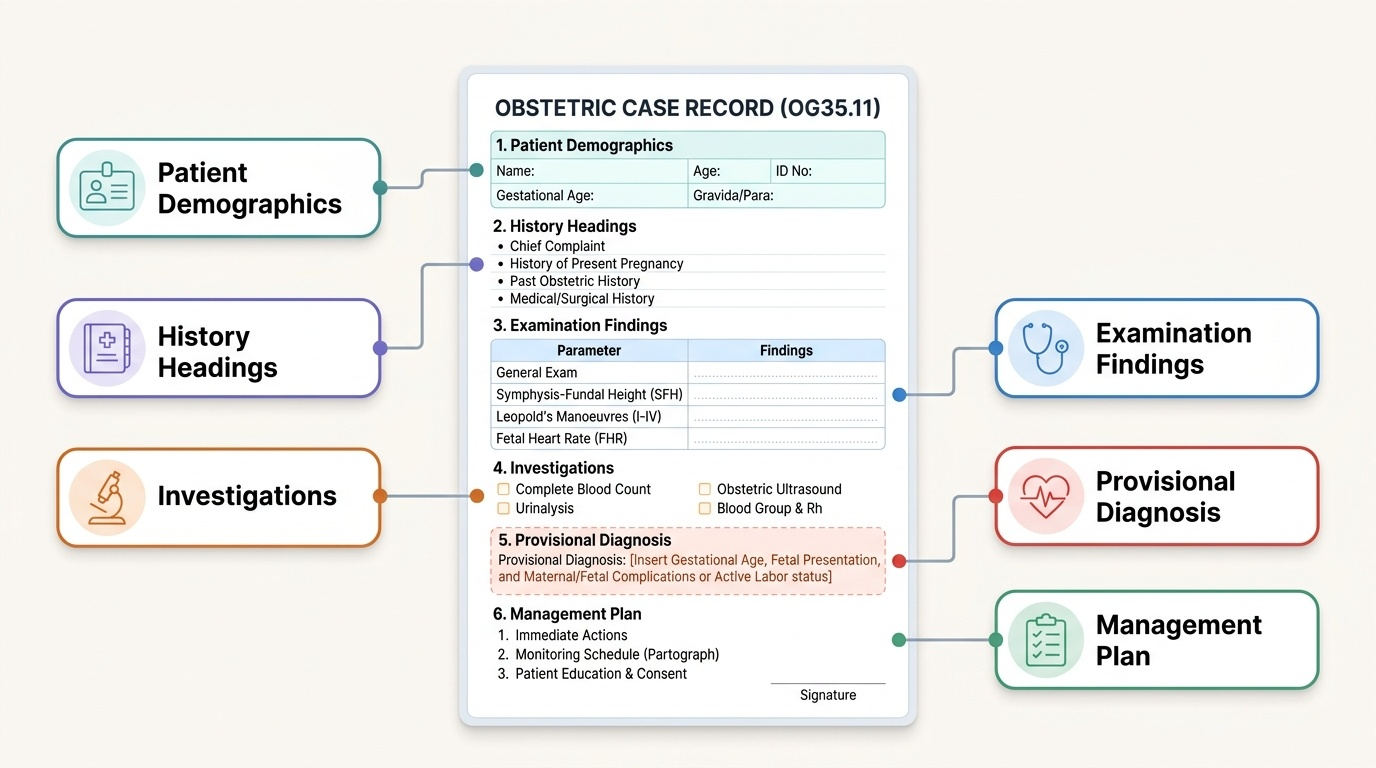
Provided image
A worked clinical example:
Patient: Mrs Priya Sharma, 25 years, G2 P1 A0 L1, LMP 12 August 2025, EDD 19 May 2026 (Naegele's rule, 28-day regular cycle). Referred at 38+2 weeks for routine ANC check.
History: No presenting complaints. Last normal fetal movements today morning. No vaginal bleeding, discharge, or leaking. Previous delivery: term SVD 2 years ago, baby 2.8 kg, no complications. No hypertension, diabetes, or chronic illness. No relevant family or drug history. Married, husband well.
General examination: Conscious, co-operative, moderately built, well-nourished. No pallor, icterus, or oedema. BP 118/74 mmHg, Pulse 82/min regular, Temp 36.8°C.
Systemic examination: CVS — S1 S2 heard, soft ejection murmur (physiological). RS — clear. No focal neurological deficit.
Obstetric abdominal examination:
- Inspection: abdomen ovoid, linea nigra present, no surgical scars, fetal movements visible.
- Fundal height: 37 cm (appropriate for 38 weeks ± 2 cm).
- Fundal grip: breech (soft, irregular) in fundus.
- Lateral grip: fetal back on left side, limbs on right — longitudinal lie.
- Pawlik's grip (1st pelvic): head (hard, round) at lower pole — vertex presentation; fixed (not ballotable) — head engaged.
- 2nd pelvic grip: fingers converge below presenting part — engaged.
- FHS: 142 bpm, regular.
Provisional diagnosis: G2 P1 A0 L1 at 38+2 weeks gestation, vertex presentation, left occipito-anterior (LOA) position, head engaged, good fetal heart rate — normal ANC visit at term.
Case record structure (all sections):
1. Patient identification (name, age, registration number, date, ward)
2. Obstetric formula summary line (G_P_A_L_, gestational age, EDD)
3. Presenting complaint
4. History of presenting illness
5. Menstrual history (LMP, cycle, regularity)
6. Obstetric history (GPAL, each pregnancy detailed)
7. Marital and contraceptive history
8. Past medical / surgical / drug history
9. Family and social history
10. General examination findings
11. Systemic examination findings
12. Obstetric abdominal examination findings (inspection, fundal height, Leopold's, FHS)
13. Investigations ordered / pending
14. Provisional diagnosis
15. Management plan
16. Clinician signature, date, and time
CLINICAL PEARL
Naegele's rule assumes a 28-day cycle — and so does the 280-day convention. In clinical practice, always ask for the cycle length before applying the rule. A woman with a 35-day cycle ovulates approximately 7 days later than a 28-day cycle woman; her EDD is 7 days later than Naegele's formula gives. Documenting this adjustment (and its rationale) in the case record protects both the patient and the clinician. Similarly, LMP-based dating becomes unreliable if the last period was not typical (e.g. break-through bleeding on the OCP mistaken for a period, or post-pill amenorrhoea followed by an irregular period). When in doubt, document the uncertainty and recommend first-trimester ultrasound.