Page 20 of 27
OG38.1-3 | Endoscopic and Sterilization Observation — SDL Guide
Learning Objectives
- State the clinical indications for diagnostic laparoscopy, operative laparoscopy, hysteroscopy, and laparoscopic tubal sterilization
- Describe the anatomical landmarks for laparoscopy port placement and the physiological principles of CO2 pneumoperitoneum
- Outline the step-by-step technique of laparoscopy (Veress entry, pneumoperitoneum, trocar placement, diagnostic survey) and hysteroscopy (distension medium, panoramic survey, operative steps)
- Describe the technique of laparoscopic tubal sterilization using Filshie clip and Falope ring
- Identify normal and abnormal endoscopic findings and describe the decision points, complications, and escalation criteria observed during supervised endoscopic procedures
INSTRUCTIONS
Gynaecological endoscopy — laparoscopy and hysteroscopy — has transformed both the diagnosis and surgical management of gynaecological conditions over the past four decades. As a final-year student, you will observe these procedures in the operation theatre. Laparoscopic tubal sterilization remains the most widely used permanent contraceptive method in India. This module prepares you to observe all three procedures with structured clinical understanding, so that your observation is active and purposeful rather than passive. These are OBSERVE competencies (OG38) — your role at this stage is structured observation, not independent performance.
References
- DC Dutta's Textbook of Gynaecology, 7th ed., Ch 12 (Endometriosis) + Ch 28 (Endoscopy in Gynaecology) (textbook)
- Shaw's Textbook of Gynaecology, 16th ed., Ch 22 (Endoscopic and Minimal Access Surgery) (textbook)
- Jeffcoate's Principles of Gynaecology, 8th ed., Ch on Operative Gynaecology (textbook)
- FOGSI Good Clinical Practice Recommendations: Laparoscopic Sterilization, 2019 (guideline)
- Sutton's Gynaecological Endoscopy, 3rd ed. — Chapters on Diagnostic and Operative Laparoscopy, Hysteroscopy (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 32-year-old woman with three living children requests permanent contraception. She is listed for laparoscopic tubal sterilization. As you stand at the OT table, the surgeon asks: 'Which part of the tube do I clip — and why does the position of the clip matter for both efficacy and reversibility?' Ten minutes later, completing a hysteroscopy in the next case (abnormal uterine bleeding), she holds up the scope and asks: 'What fluid am I using and what am I watching the deficit for?' Your readiness to answer — tube anatomy, clip mechanics, distension media, fluid monitoring — reflects how well you have prepared for this observation session.
WHY THIS MATTERS
Gynaecological endoscopy is the backbone of modern minimal-access gynaecological surgery. Laparoscopy (OG38.1) allows both diagnostic evaluation of the pelvis and therapeutic intervention — from adhesiolysis and cystectomy to management of ectopic pregnancy — without the morbidity of laparotomy. Hysteroscopy (OG38.2) provides direct visualisation of the uterine cavity, replacing blind curettage as the gold standard for evaluation of abnormal uterine bleeding, suspected submucosal fibroids, endometrial polyps, and uterine septa. Laparoscopic tubal sterilization (OG38.3) is the most commonly performed sterilization procedure in India, accounting for over 80% of all sterilizations in the National Family Health Survey data — making it a procedure you will encounter repeatedly throughout your career, both in elective and post-partum settings. A final-year student who understands these procedures can assist intelligently, recognise complications early, and counsel patients and families with accuracy.
RECALL
Refresh the following anatomical and physiological foundations before observing: (1) The uterus is a muscular, pear-shaped organ lying between the bladder (anteriorly) and the rectum (posteriorly) in the pelvis; the fallopian tubes arise from the uterine cornua and traverse to the ovaries. (2) The isthmic portion of the fallopian tube — the 2–3 cm segment adjacent to the uterine cornua — is the narrowest and most surgically accessible for sterilization clip application. (3) The broad ligament is a double peritoneal fold that contains the tube, ovary (attached by the mesosalpinx), and round ligament. (4) CO2 is the insufflation gas of choice for pneumoperitoneum because it is rapidly absorbed and does not support combustion; it is irritant to the peritoneum and contributes to referred shoulder tip pain postoperatively. (5) Normal saline is the preferred distension medium for diagnostic and operative hysteroscopy (with bipolar energy); older glycine 1.5% (electrolyte-free) was used with monopolar instruments and carries a hyponatraemia risk from absorption.
Indications for Laparoscopy, Hysteroscopy, and Laparoscopic Sterilization
Understanding the clinical question that drives each procedure is the first step in structured observation. Before you enter the OT, you should know why this particular patient is having this particular operation — and what the surgeon is looking for or planning to do. Without this, you are watching without a frame of reference, and your observation yields little learning.
Diagnostic laparoscopy (OG38.1) is indicated when clinical, biochemical, and imaging evaluation cannot definitively answer the pelvic question. The most common indications include: suspected endometriosis (pelvic pain, dysmenorrhoea, dyspareunia with a normal ultrasound — laparoscopy remains the gold standard for diagnosis); investigation of chronic pelvic pain of unknown origin; evaluation of tubal patency in infertility workup (combined with chromopertubation — injection of methylene blue through the cervix to visualise tubal spillage); assessment of an adnexal mass when ultrasound findings are indeterminate; and diagnosis of a suspected ectopic pregnancy when haemodynamically stable.
Operative (therapeutic) laparoscopy extends diagnostic laparoscopy to include surgical intervention in the same setting. Common operative applications include: laparoscopic ovarian cystectomy (for benign endometrioma or dermoid cyst); adhesiolysis for tubo-ovarian adhesions; salpingectomy or salpingostomy for ectopic pregnancy; myomectomy for subserosal or pedunculated fibroids; and staging and excision of endometriotic deposits.
Hysteroscopy (OG38.2) is indicated for the evaluation and treatment of intrauterine pathology. The major diagnostic indications are: abnormal uterine bleeding (heavy, irregular, or postmenopausal bleeding) where endometrial pathology is suspected; recurrent pregnancy loss where a uterine septum, intrauterine adhesions (Asherman syndrome), or polyps may be contributing; and infertility workup to evaluate the uterine cavity. Operative hysteroscopy allows directed polypectomy, myomectomy of submucosal fibroids, septal resection, and lysis of intrauterine adhesions.
Laparoscopic tubal sterilization (OG38.3) is requested by a woman who has completed her family and desires permanent, highly effective contraception. Counselling is mandatory and must confirm that the decision is voluntary, fully informed (including that sterilization is intended to be permanent and reversal success rates are low), and that alternative long-acting reversible methods (such as the copper IUCD CuT 380A, effective for 10 years) have been discussed. Informed written consent is obtained before the procedure.
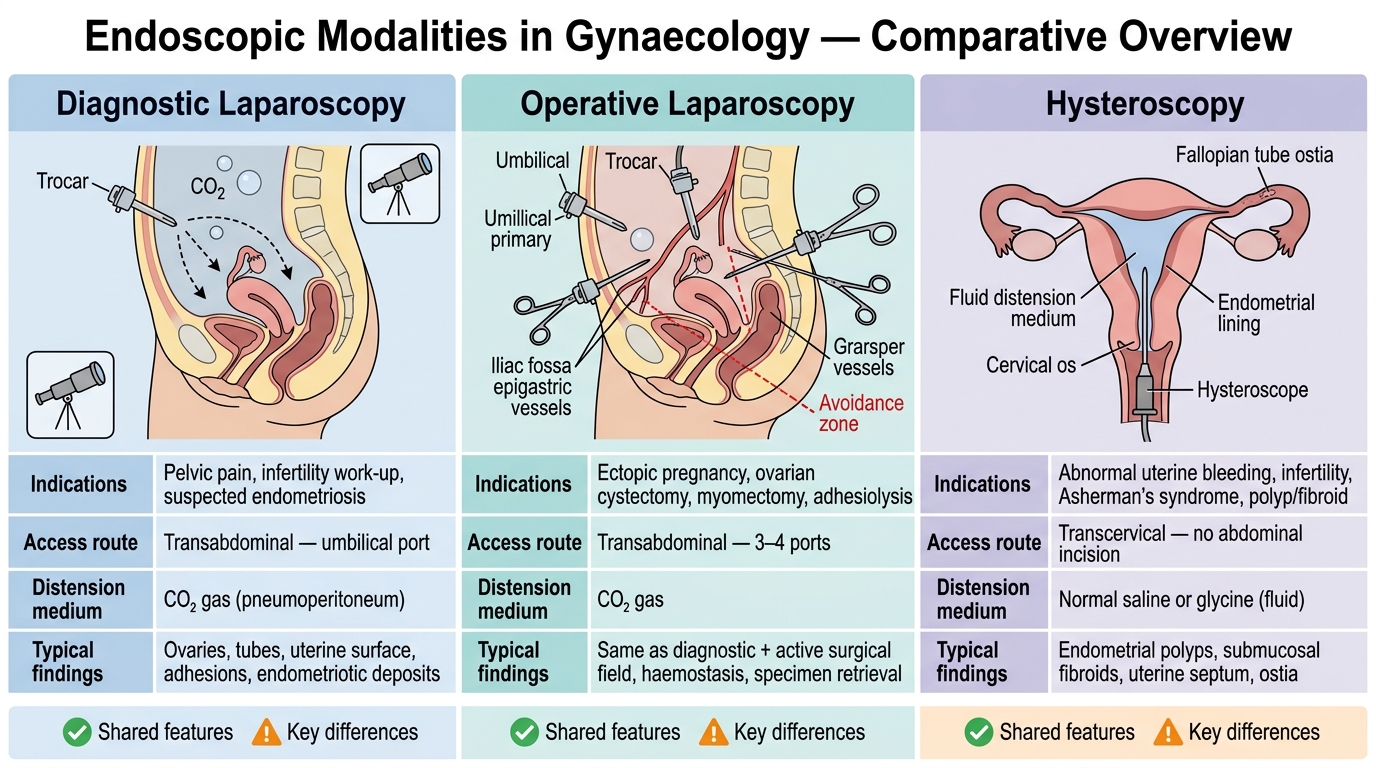
Comparison of Gynaecological Endoscopic Modalities: Laparoscopy vs Hysteroscopy
Relevant Anatomy and Physiological Principles of Endoscopy
Safe endoscopic surgery is grounded in precise anatomical knowledge — specifically, the structures at risk during port insertion and the physiological changes created by the operative environment. Knowing this anatomy as an observer allows you to understand why the surgeon chooses a specific entry point or why an anaesthetist makes ventilator adjustments during a laparoscopy.
Port placement anatomy for laparoscopy: The primary port (for the telescope) is almost always inserted at or just below the umbilicus, where the abdominal wall is thinnest and the underlying pelvic organs are accessible. The anterior abdominal wall at this level contains the skin, subcutaneous fat, linea alba, and peritoneum — with no muscle intervening at the midline. Critically, the inferior epigastric vessels (branches of the external iliac artery) run laterally and must be avoided by the secondary (operating) ports, which are typically placed in the right and left iliac fossae lateral to the rectus muscle. The bladder must be emptied with a urinary catheter before port insertion to reduce its dome below the symphysis pubis and prevent inadvertent cystotomy.
CO2 pneumoperitoneum physiology: Creating an adequate working space requires distension of the peritoneal cavity with carbon dioxide insufflated to a pressure of 12–15 mmHg. CO2 is chosen because it is inert, rapidly absorbed, and does not support combustion (important when electrosurgery is used). The physiological consequences of pneumoperitoneum include: elevation of the diaphragm (reducing lung compliance and functional residual capacity — anaesthesia compensates by increasing tidal volume or PEEP); cardiovascular effects — modest increase in heart rate and peripheral resistance; and systemic CO2 absorption, which raises end-tidal CO2 (ETCO2) and requires the anaesthetist to increase minute ventilation. In the Trendelenburg position (head-down, 15–20 degrees) used for pelvic access, these effects are compounded: venous return increases but respiratory compliance is further reduced.
Hysteroscopy distension principles: The uterine cavity is a potential space that collapses without distension. Normal saline (isotonic, used with bipolar energy systems) is the modern first-choice distension medium: it carries minimal risk if absorbed since it is isotonic. Older glycine 1.5% (used with monopolar energy) is hypotonic and electrolyte-free — absorption causes dilutional hyponatraemia, cerebral oedema, and the TURP-like syndrome. A fluid deficit (volume instilled minus volume recovered) must be continuously monitored: safe limit is approximately 2500 mL for saline and 1000 mL for glycine/sorbitol — the procedure should be stopped and electrolytes checked if these thresholds are approached.
Fallopian tube anatomy for sterilization: The fallopian tube has four segments — intramural (within the uterine wall), isthmic (narrow 2–3 cm segment adjacent to the cornua), ampullary (widest, site of fertilisation), and fimbrial (fringed end near the ovary). Both the Filshie clip and the Falope ring are applied to the isthmic portion, 2–3 cm from the uterine cornua, to maximise efficacy and minimise the amount of tube destroyed (preserving the maximum length for potential reversal, though reversal is not guaranteed).
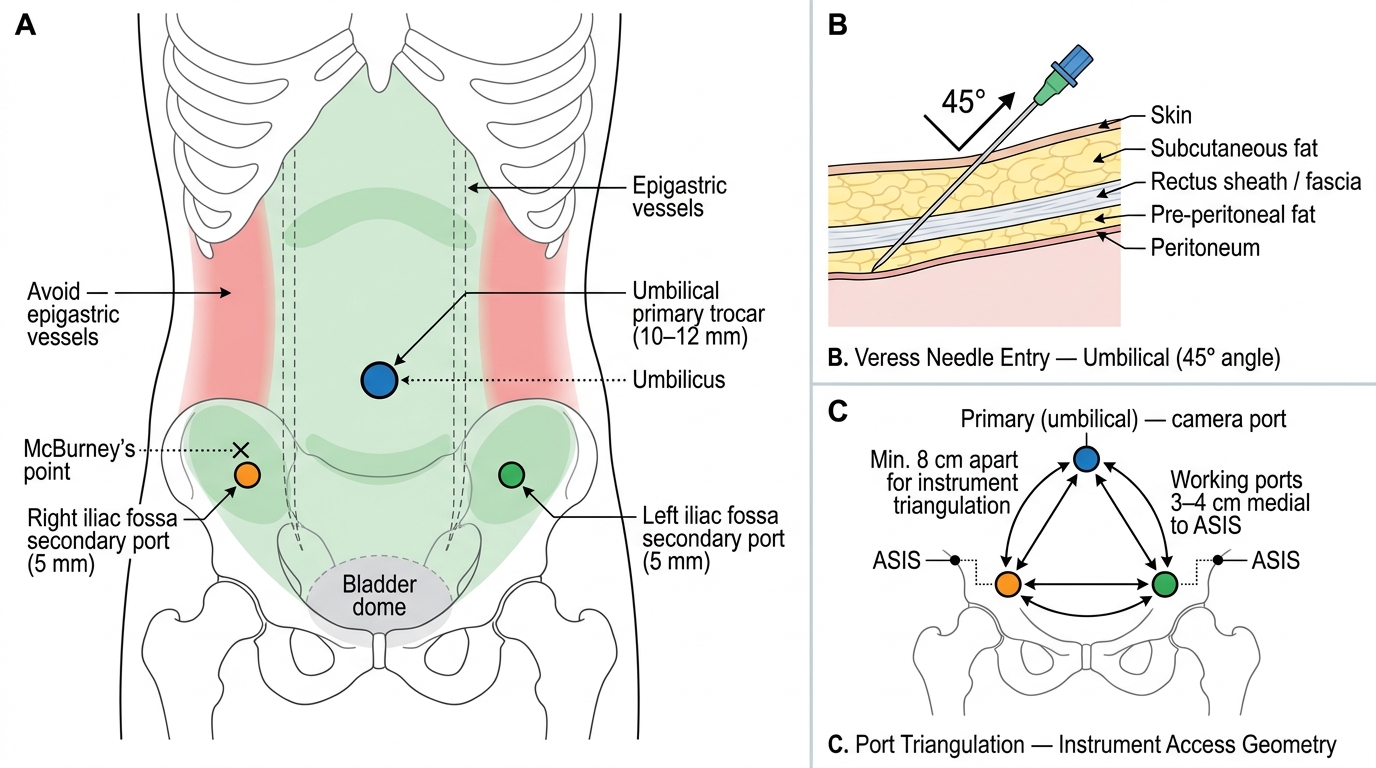
Standard Laparoscopy Port Positions and Entry Technique
Laparoscopy Technique: Entry, Survey, and Operative Steps
The laparoscopy procedure begins before any incision — with a pre-operative check, patient positioning, and team brief that establish safety. As an observing student, watching this pre-operative sequence teaches you the communication and coordination standards of minimal-access surgery.
Positioning and preparation: The patient is placed in a modified lithotomy position with both legs in stirrups, allowing the surgeon access to the perineum (for a uterine manipulator if needed) while operating at the abdomen. A urinary catheter is inserted to empty the bladder. A uterine manipulator (e.g., Cohen cannula) may be placed vaginally to allow intraoperative uterine movement and position change — this is essential for chromopertubation and for retracting the uterus away from pelvic structures during dissection.
Entry technique — Veress needle: The most common closed entry technique uses a Veress needle — a spring-loaded needle with a blunt inner stylet that retracts on meeting resistance and extends (protecting viscera) once through the peritoneum. The needle is inserted through a small umbilical incision at a 45-degree angle toward the pelvis (60 degrees in obese patients). Correct intraperitoneal placement is confirmed by: (a) the hanging-drop test — a drop of saline placed in the needle hub is aspirated in with negative pressure when the needle tip is free in the peritoneal cavity; (b) initial insufflation pressure below 10 mmHg — high initial pressure (>10 mmHg) suggests the needle tip is in preperitoneal fat or against bowel; (c) equal gas distribution causing the abdomen to distend symmetrically.
CO2 insufflation and trocar insertion: Once the Veress needle position is confirmed, CO2 is insufflated to 12–15 mmHg. The needle is withdrawn and the primary trocar (10–12 mm, for the 0° or 30° telescope) is inserted at the umbilical incision with a controlled, twisting motion. Secondary 5 mm operating trocars are placed in the lower quadrants under direct laparoscopic vision, lateral to the inferior epigastric vessels.
Diagnostic survey — the 360° systematic review: On entering the peritoneum with the telescope, the surgeon performs a systematic evaluation covering: the uterus (size, surface, any fibroids or adhesions), both fallopian tubes (course, fimbrial ends), both ovaries (size, cyst, surface), the Pouch of Douglas (free fluid, endometriotic deposits), the anterior peritoneum and vesico-uterine fold, and the appendix and adjacent bowel. This systematic approach ensures no pathology is missed.
Operative steps (example — chromopertubation): Methylene blue is injected through the uterine manipulator into the cervix. The surgeon watches the fallopian tube fimbrial ends for blue dye spillage — free spill confirms tubal patency; no spill on one side suggests tubal block (relevant in infertility evaluation).
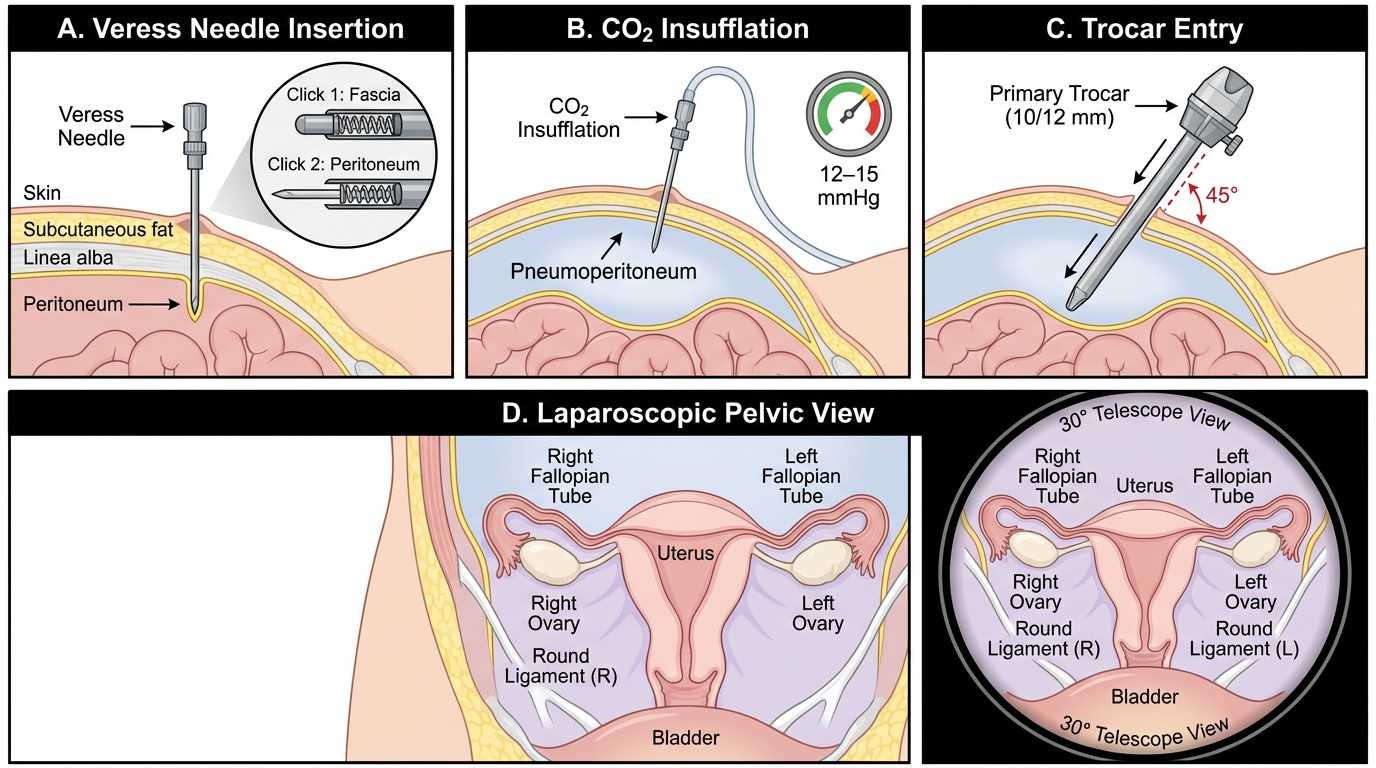
Laparoscopic Entry Technique: Veress Needle to Pelvic Survey