Page 21 of 27
OG38.1-3 | Endoscopic and Sterilization Observation — SDL Guide (Part 2)
Hysteroscopy Technique and Laparoscopic Tubal Sterilization
Two of the three competencies in this cluster — hysteroscopy (OG38.2) and laparoscopic tubal sterilization (OG38.3) — involve distinct techniques that you will observe in separate procedure contexts. Both share the requirement for careful instrument setup, patient selection, and real-time monitoring.
Hysteroscopy technique: The hysteroscope consists of a rigid telescope (2.7–4 mm diameter, 0° or 30° optic), an outer sheath with inflow and outflow channels, and — for operative hysteroscopy — an additional working channel for instruments (scissors, resectoscope loop, bipolar electrode). The procedure follows this sequence: (1) the cervix is exposed with a Sims speculum and held with a tenaculum; (2) the cervical canal is gently dilated if narrow (Hegar dilators to 5–6 mm); (3) the sheath is introduced through the internal os under direct vision or with a vaginoscopic (no-touch) technique (no tenaculum, no speculum, continuous saline flow guides entry — better tolerated under local anaesthesia); (4) distension medium flows continuously, maintaining cavity distension at 50–80 mmHg intrauterine pressure; (5) the surgeon performs a panoramic survey — examining the posterior wall, anterior wall, tubal ostia (one on each side), and the endometrial surface; (6) targeted biopsy, polypectomy, or septal resection is performed under direct vision.
For operative hysteroscopy, fluid deficit monitoring is continuous — an assistant tracks volumes instilled and recovered on a whiteboard in real time. The procedure is stopped and a fluid check ordered if the deficit approaches the threshold.
Laparoscopic tubal sterilization technique: After standard laparoscopic entry and pneumoperitoneum establishment, the fallopian tube is identified and elevated at its isthmic portion (2–3 cm from the uterine cornua) using atraumatic grasping forceps. Two devices are in common use:
- Filshie clip — a titanium clip lined with silicone rubber, applied at right angles across the isthmus using a specially designed applicator. When correctly applied, the clip crushes the tube to complete occlusion and the silicone rubber expands slightly to maintain secure contact. It is the most widely used clip worldwide; failure rate approximately 1 in 200 cumulative 10-year risk.
- Falope ring (silastic band) — a silicone ring applied to a 2 cm loop of the isthmic tube, drawn up into the applicator barrel and then released to constrict the loop base. It destroys a slightly larger segment of tube than the Filshie clip.
Both methods require that the tube is positively identified (not the round ligament or a vessel) before the device is applied — a critical safety step the surgeon performs by tracing the tube from the cornua.
| Feature | Filshie Clip | Falope Ring | Pomeroy (open) |
|---|---|---|---|
| Material | Titanium + silicone | Silastic silicone | Absorbable suture |
| Tube segment destroyed | Minimal (isthmic, ~5 mm) | ~2 cm loop | ~2 cm mid-isthmus |
| Reversibility potential | Highest (least tissue lost) | Moderate | Low |
| Failure rate (10-yr) | ~1 in 200 | ~1 in 150 | ~1 in 200 |
| Preferred setting | Interval; laparoscopic | Interval; laparoscopic | Post-partum open |
SELF-CHECK
During laparoscopy, the Veress needle is inserted at the umbilicus. The initial CO2 insufflation pressure reads 15 mmHg immediately on starting the flow. What does this most likely indicate?
A. Correct intraperitoneal needle placement — proceed with insufflation
B. Preperitoneal or incorrect needle placement — reposition the Veress needle before continuing
C. A normal finding in obese patients — increase the gas flow rate
D. Gas embolism — stop the procedure immediately
Reveal Answer
Answer: B. Preperitoneal or incorrect needle placement — reposition the Veress needle before continuing
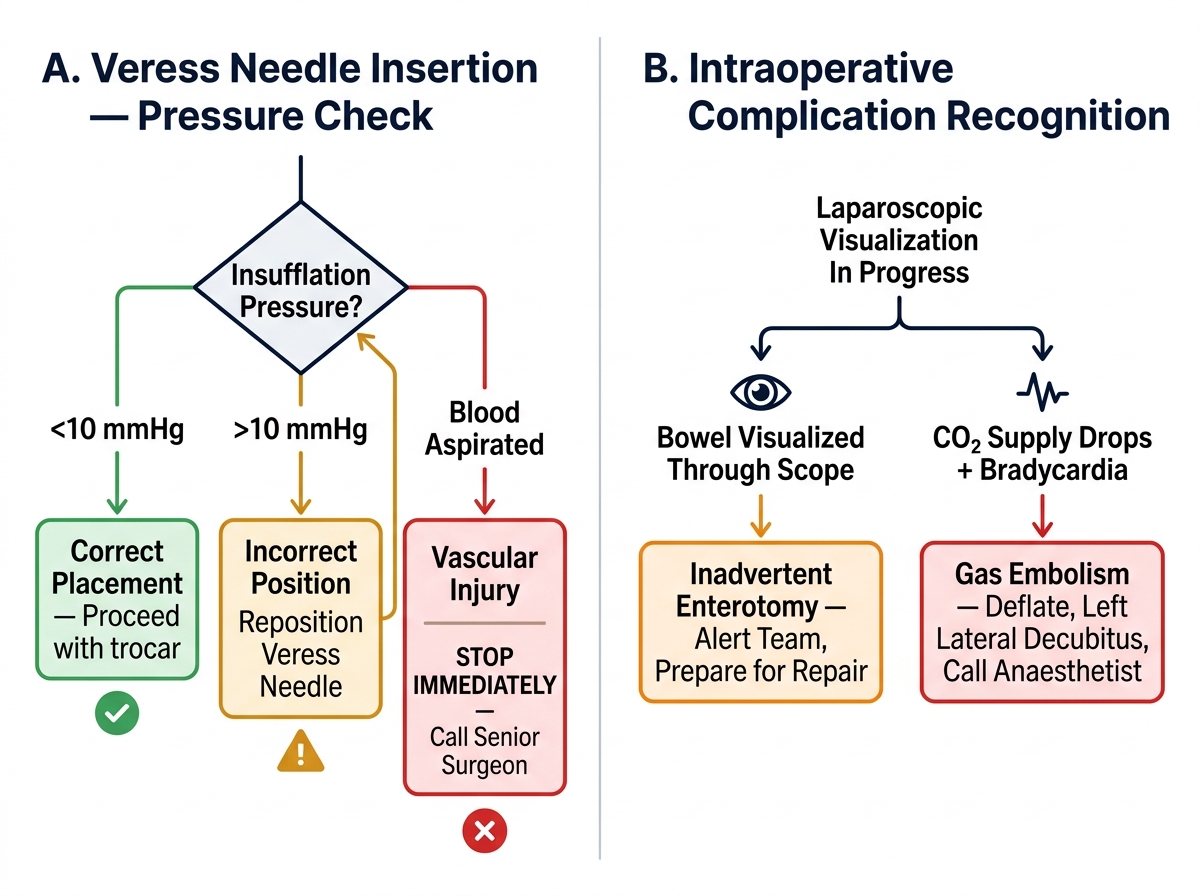
Initial insufflation pressure above 10 mmHg strongly suggests that the Veress needle tip is NOT in the free peritoneal cavity — it is most likely lodged in preperitoneal fat, against bowel wall, or in an adhesion. Correct intraperitoneal placement should show initial pressure below 10 mmHg. The needle should be repositioned and the hanging-drop test and pressure check repeated before proceeding. Gas embolism would require blood aspiration and vascular signs, not simply high pressure.
Interpreting Endoscopic Findings
A key learning goal for the observing student is to develop a vocabulary of normal and abnormal endoscopic appearances. The quality of your observation depends on knowing what normal looks like, so that deviations are immediately apparent. This section describes the most important findings you are likely to encounter during diagnostic laparoscopy and hysteroscopy.
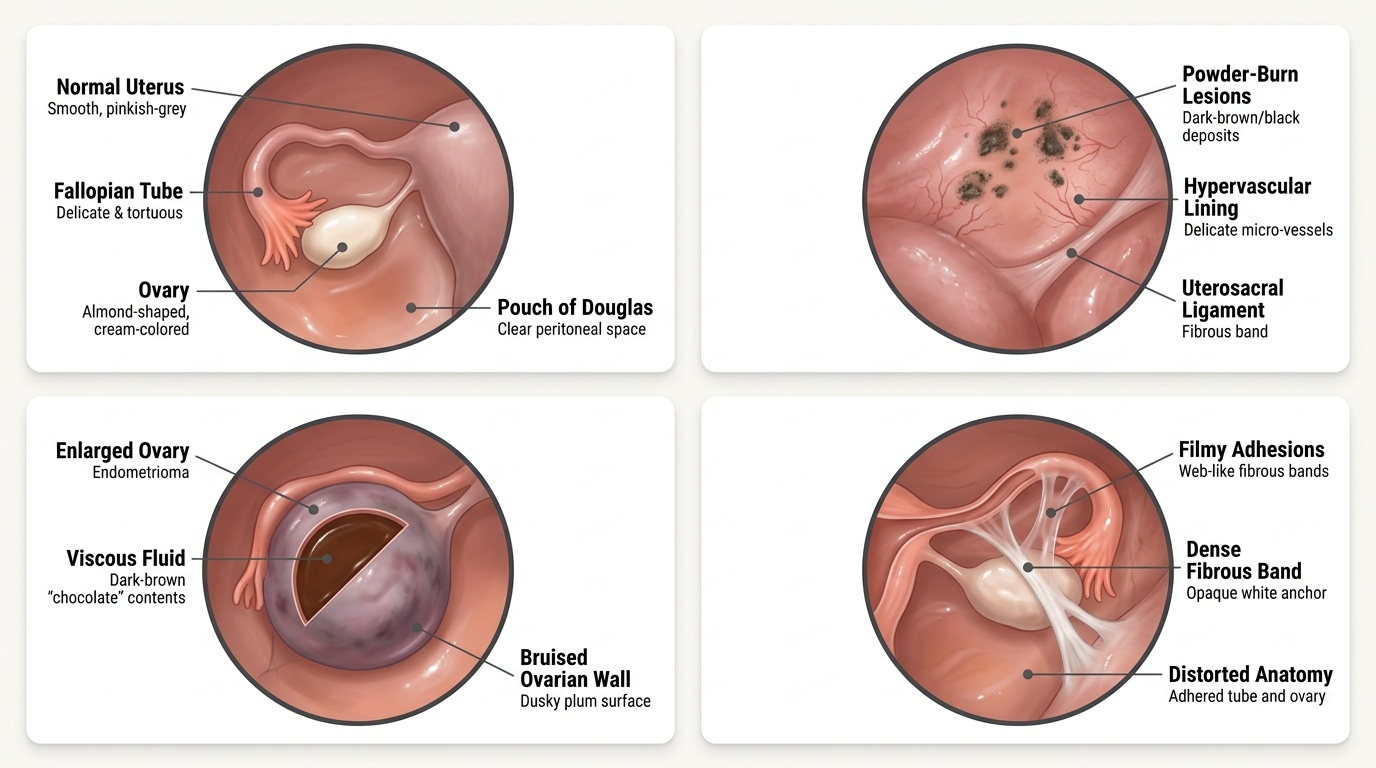
Normal laparoscopic pelvic anatomy: The uterus appears as a smooth, muscular, pinkish-grey organ. The fallopian tubes are visible as delicate, tortuous structures with fimbrial ends that drape toward the ovaries. The ovaries are almond-shaped, smooth-surfaced, and cream-coloured; follicles and corpora lutea may be visible as surface cysts depending on cycle day. The Pouch of Douglas should be free of fluid (small amounts of clear fluid are normal in the secretory phase); the peritoneal surfaces should be smooth and glistening.
Endometriosis on laparoscopy: The classical appearances of endometriosis are varied but include: powder-burn lesions — dark brown-black deposits of haemosiderin-laden macrophages on the peritoneum, particularly in the Pouch of Douglas, uterosacral ligaments, and ovarian surface; endometriomas (chocolate cysts) — ovarian cysts with dark brown ('chocolate') contents due to repeated haemorrhage; adhesions — filmy or dense fibrous bands between tube and ovary, uterus and bowel, or between adjacent pelvic structures; and scarring with obliteration of the Pouch of Douglas in severe disease.
Ectopic pregnancy on laparoscopy: A tubal ectopic is seen as a sausage-shaped swelling at the ampullary or isthmic-ampullary junction, often with surface bruising (haemorrhage under the serosa). The Pouch of Douglas may contain haemoperitoneum. The contralateral tube and ovary should always be assessed.
Normal hysteroscopic findings: The uterine cavity appears as a triangular or pear-shaped space when distended. The endometrium has a smooth, regular surface (appearance varies with cycle phase — thin and pale in the proliferative phase; thickened, vascular, and glandular in the secretory phase). Both tubal ostia are visible as small, round openings in the upper lateral corners of the cavity.
Abnormal hysteroscopic findings: Endometrial polyps appear as smooth, soft, pedunculated or sessile projections with their own vascular stalk; they are mobile in the distension medium. Submucosal fibroids are smooth-surfaced, firm, whitish protrusions that distort the cavity and are attached to the myometrium (not pedunculated like polyps). Uterine septa appear as a central midline ridge of fibromuscular tissue dividing the cavity — its surface is avascular and paler than surrounding endometrium; unlike a bicornuate uterus (an external deformity), a septum is an internal defect amenable to hysteroscopic resection.
Provided image
SELF-CHECK
During a diagnostic hysteroscopy for recurrent miscarriage, the surgeon identifies a midline ridge that divides the uterine cavity into two compartments. The ridge is avascular, paler than the surrounding endometrium, and extends from the fundus toward the cervix. What is the most likely diagnosis?
A. Submucosal fibroid — plan laparoscopic myomectomy
B. Uterine septum — amenable to hysteroscopic septal resection
C. Bicornuate uterus — requires laparoscopic metroplasty
D. Intrauterine adhesions (Asherman syndrome) — plan adhesiolysis
Reveal Answer
Answer: B. Uterine septum — amenable to hysteroscopic septal resection
An avascular, pale midline ridge extending from the fundus into the cavity is the classic hysteroscopic appearance of a uterine septum. Septa are fibromuscular, hypovascular (hence paler), and arise from incomplete fusion of the Müllerian ducts. They are an intrauterine (not external) structural defect and are amenable to hysteroscopic septal resection. A bicornuate uterus has an external fundal indentation and two cavities, visible on imaging and laparoscopy; it is not corrected hysteroscopically. Submucosal fibroids are smooth, firm protrusions, not midline ridges.
Observing Endoscopic Procedures: Decision Points, Complications and Escalation
Your role during observation is not passive attendance but active pattern recognition. The following complications represent the moments when a surgical procedure can change course rapidly. Understanding their mechanisms — and the surgeon's response — is the highest-value learning you will take from the OT.
Entry complications (laparoscopy):
Vascular injury — inadvertent puncture of a major vessel (aorta, inferior vena cava, iliac vessels, inferior epigastric artery) is the most catastrophic entry complication. Signs: blood aspirated through the Veress needle before gas, or a rapid pooling of blood in the Pouch of Douglas visible immediately on telescope insertion. Response: immediate conversion to emergency laparotomy, call senior vascular/gynaecological consultant, IV access and blood products. This is an operating theatre emergency.
Bowel injury — the Veress needle or primary trocar may enter the small or large bowel, particularly in patients with previous laparotomy (adhesions bringing bowel to the abdominal wall). Sign: faecal smell on gas release, bowel mucosa visible through the telescope, bowel content in the aspirate. Response: stop procedure, assess extent, convert to laparotomy for repair.
Preperitoneal insufflation — CO2 enters the preperitoneal space instead of the peritoneal cavity; the abdomen distends asymmetrically, there is subcutaneous emphysema, and laparoscopic vision shows fatty preperitoneal layers rather than the peritoneum. Response: deflate, reposition Veress needle, use open (Hasson) entry technique.
Gas embolism — rare but life-threatening: CO2 enters a torn vein and causes a frothy lock in the right heart. Signs: sudden severe hypotension, a characteristic mill-wheel murmur on cardiac auscultation, and an abrupt fall in end-tidal CO2. Response: stop insufflation immediately, place patient head-down left lateral (Durant's manoeuvre), aspirate gas via central venous catheter, call anaesthesia and intensivist.
Hysteroscopy — fluid overload: Excessive intrauterine pressure or prolonged procedure leads to absorption of distension medium. Watch for: progressive fluid deficit on the whiteboard, anaesthesia noting declining sodium (for glycine) or dilutional signs. The surgeon will stop the procedure, obtain urgent electrolytes, and manage as dilutional hyponatraemia (sodium correction for glycine-TURP syndrome).
Failed clip application during sterilization: If the Filshie clip fails to fully close (visible gap on inspection) or is applied to the wrong structure (round ligament mistaken for tube), the surgeon removes the clip and reapplies after confirming tube identity. Bilateral application must be confirmed before closure.
| Complication | Sign you observe | Immediate response |
|---|---|---|
| Vascular injury (Veress) | Blood aspirated; haemoperitoneum on entry | Laparotomy; call senior; blood products |
| Bowel injury | Faecal odour; bowel mucosa visible | Laparotomy; repair |
| Preperitoneal insufflation | Asymmetric distension; fat visible | Deflate; reposition; Hasson entry |
| Gas embolism | Hypotension; mill-wheel murmur; ETCO2 drop | Stop gas; Durant's manoeuvre; ICU |
| Hysteroscopy fluid overload | Fluid deficit approaching threshold | Stop; electrolytes; treat hyponatraemia |
| Failed clip / wrong structure | Clip gap visible; structure doesn't track from cornua | Reapply after re-identifying tube |
Laparoscopic Complication Recognition: Veress Insertion Pressure Check and Intraoperative Decision Algorithm
SELF-CHECK
During laparoscopic tubal sterilization, the Filshie clip has been applied to what appears to be the right fallopian tube. Before closing the abdomen, the surgeon traces the structure proximally and realises it originates from the lateral pelvic wall, not the uterine cornua. What is the correct action?
A. Leave the clip in place — the structure has already been occluded
B. Remove the clip and reapply after positively identifying the right fallopian tube from its origin at the uterine cornua
C. Proceed to the left tube and document the right as a technical difficulty
D. Convert to laparotomy for open Pomeroy sterilization
Reveal Answer
Answer: B. Remove the clip and reapply after positively identifying the right fallopian tube from its origin at the uterine cornua
The clip has been applied to the wrong structure — most likely the round ligament, which originates from the lateral uterus and exits through the inguinal canal (not the cornua). The round ligament does not connect to the ovary and has no role in fertility. Leaving the clip in place would result in a failed sterilization (the tube is intact). The correct action is to remove the clip, positively re-identify the right fallopian tube by tracing it from the uterine cornua to the fimbrial end, and apply a new clip to the isthmic portion. Conversion to laparotomy is not warranted for a recognised instrument error that can be corrected laparoscopically.
CLINICAL PEARL
Always trace the fallopian tube from the uterine cornua before applying a sterilization clip. The round ligament and the fallopian tube both exit the uterus in the same anatomical region and can look deceptively similar to an inexperienced eye, particularly in a patient with adhesions distorting normal anatomy. The definitive identifier is origin: the tube arises from the uterine cornua (upper lateral uterus), has a fimbrial end near the ovary, and is adjacent to the mesosalpinx. The round ligament arises slightly anteriorly, has no fimbrial end, and exits via the inguinal canal. In a report reviewing laparoscopic sterilization failures, misidentification of the round ligament accounted for a small but consistent proportion of late failures. The single safest habit is to never apply a clip to any structure you have not traced from end to end.
Self-Assessment: Endoscopic Procedures Knowledge Check
The three endoscopic competencies in this module — diagnostic and operative laparoscopy (OG38.1), hysteroscopy (OG38.2), and laparoscopic tubal sterilization (OG38.3) — span a range of procedures, anatomical landmarks, physiological principles, and findings that must be integrated into a single coherent mental model. Consolidating this knowledge requires you to actively retrieve what you have learned rather than simply re-reading it. Self-quizzing — particularly without looking at the source material — is among the most effective study strategies for retaining procedural and anatomical knowledge, backed by extensive evidence from cognitive science (retrieval practice, Roediger & Karpicke 2006). The questions below span all three competencies and correspond directly to what an examiner will test in a viva voce and what a senior will ask in the OT during your next observation session. Work through each question from memory first, then check your answers against the relevant module sections.
Key recall questions:
- What are the three main clinical indications for diagnostic laparoscopy in gynaecology?
- Why is the urinary bladder catheterised before laparoscopy, and which vessel must the secondary ports avoid?
- What initial insufflation pressure confirms correct Veress needle placement, and what does a pressure above 10 mmHg suggest?
- What is the safe fluid deficit threshold for saline (bipolar) hysteroscopy, and what complication does exceeding it cause?
- What is the hysteroscopic appearance that distinguishes a uterine septum from a submucosal fibroid?
- Why must the fallopian tube be traced from the uterine cornua before Filshie clip application?
- What is Durant's manoeuvre and when is it used during laparoscopy?
Quick self-test: Without notes, sketch the approximate positions of the three laparoscopy ports and name two structures the secondary ports must avoid. Check your sketch against the anatomy image in this module.