Page 15 of 27
OG37.6 | Outlet Forceps, Vacuum and Breech Delivery Observation — SDL Guide (Part 3)
Observing Complications — Maternal and Neonatal
Assisted delivery carries specific risks for both the mother and the neonate that differ between the three methods. The informed observer should recognise these complications as they are identified and documented, and understand the rationale for each part of the post-delivery examination.
Maternal complications:
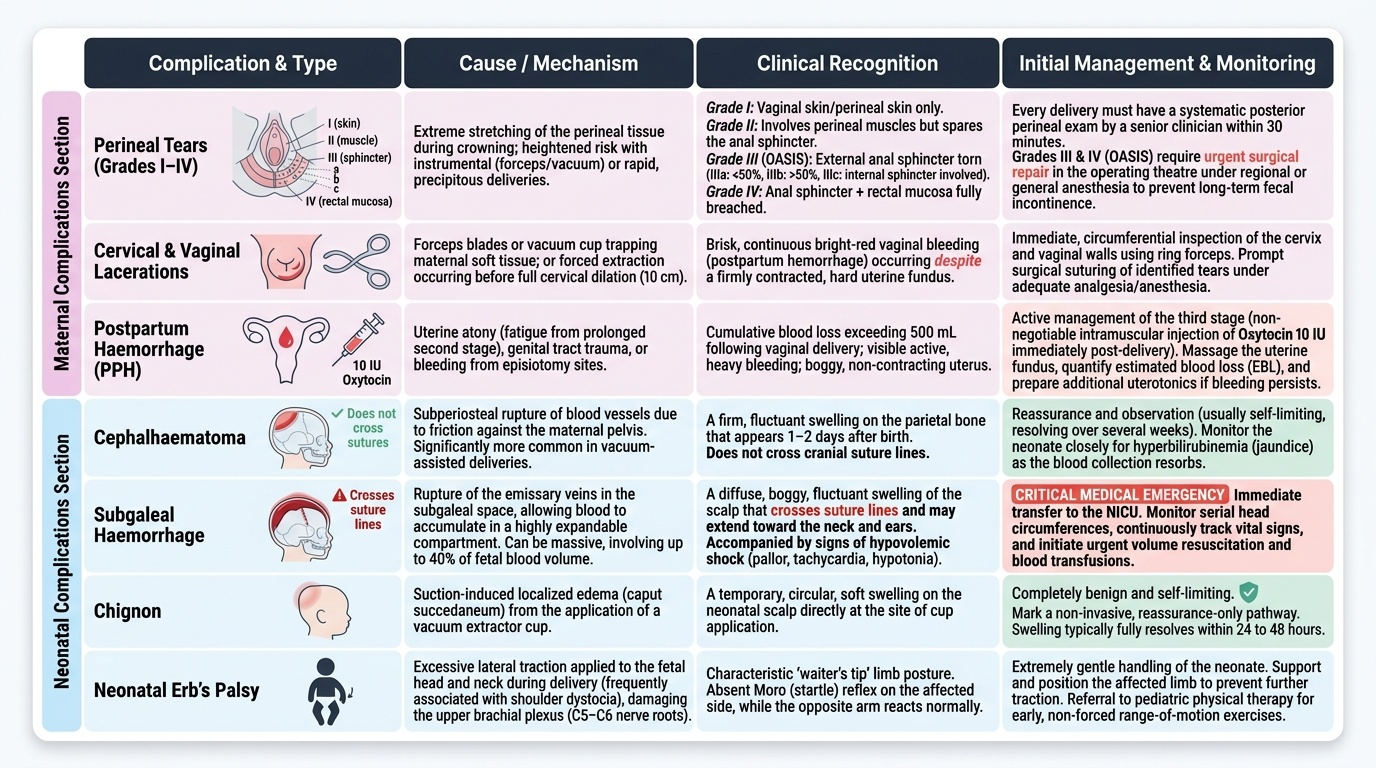
Perineal tears are classified by degree and must be systematically assessed after every delivery, instrumental or spontaneous. Grade I = skin only; Grade II = perineum muscles but not sphincter; Grade III = external anal sphincter (IIIa <50% torn, IIIb >50%, IIIc includes internal sphincter); Grade IV = anal sphincter + rectal mucosa. Grade III/IV tears (obstetric anal sphincter injuries, OASIS) require surgical repair under regional or general anaesthesia and carry long-term risk of faecal incontinence. All instrumental deliveries — and high-tone, precipitous spontaneous deliveries — should have a careful systematic posterior perineal examination by a senior clinician within 30 minutes of delivery.
Cervical and vaginal lacerations occur when forceps blades or the vacuum cup are applied against maternal soft tissue, or when delivery occurs before full dilatation. After delivery, the cervix and vaginal walls are inspected using ring forceps to examine the cervical lip circumferentially. Unrecognised cervical tears can bleed briskly and cause PPH — the first port of call when a fundus is contracted but PPH continues after instrumental delivery is cervical and vaginal inspection.
Postpartum haemorrhage: Instrumental delivery increases the risk of PPH through atony (prolonged second stage → uterine fatigue), trauma lacerations, or episiotomy bleeding. Active management of the third stage (oxytocin 10 IU IM immediately after delivery) is non-negotiable. The observer should note the estimated blood loss and whether additional uterotonics were needed.
Neonatal complications:
Cephalhaematoma — a subperiosteal collection of blood (does not cross suture lines) that appears as a firm, fluctuant swelling on the parietal bone, peaking at 1–2 days and resolving over weeks. More common with vacuum than forceps. Usually self-limiting but can cause jaundice.
Subgaleal haemorrhage — bleeding in the subgaleal space (beneath the epicranial aponeurosis); crosses suture lines and can be massive, with up to 40% of fetal blood volume potentially lost into this space. The scalp feels boggy, the swelling is diffuse and increasing. This is a neonatal emergency — the paediatric team must be alerted immediately.
Chignon — the dome of oedematous scalp tissue drawn up into the ventouse cup; always present after vacuum and resolves within 24–48 hours; normal finding, not a complication per se but parents should be reassured.
Erb's palsy — brachial plexus injury from lateral neck traction in breech delivery; presents as a floppy arm with adduction and internal rotation at the shoulder, pronation of the forearm, loss of biceps reflex. Most cases recover spontaneously within months; rare persistent cases require physiotherapy and orthopaedic review.
Provided image
Self-Assessment — Assisted Delivery Observation
Use the following questions to test your knowledge before attending an assisted delivery and to consolidate your learning afterwards. These questions are pitched at the SH level (observe and assist) appropriate for NMC OG37.6. Constructing complete answers from memory before consulting a reference is considerably more effective for long-term learning than passive reading — force yourself to articulate the reasoning, not just the answer. The questions progress from factual recall to clinical reasoning, which is the level you need to perform at in a structured viva or OSCE. After your labour-ward session, discuss these questions with the registrar who performed the procedure — asking about their intraoperative decision-making is one of the highest-yield uses of your time in the labour room.
Think through each question carefully before reviewing the answers:
- List the five prerequisites for instrumental vaginal delivery using the ABCDE mnemonic and explain the clinical consequence if any one prerequisite is absent.
- What is the correct order of blade insertion in a Wrigley's forceps delivery, and why is the left blade inserted first?
- Where precisely is the 'flexion point' of the fetal head, and why is cup placement at this point critical for vacuum extraction?
- A ventouse cup pops off three times without progress. What decision should be made and why?
- Name three types of breech presentation and state which has the highest risk of cord prolapse.
- What is the 'hands off the breech' principle, and at what point does intervention become appropriate?
- Describe the Mauriceau-Smellie-Veit manoeuvre in your own words. Why are fingers placed on the malar bones rather than the mandible?
- What is the difference between a cephalhaematoma and a subgaleal haemorrhage, and which is an emergency?
- Name the degrees of perineal tear from I to IV, and state which degree requires surgical repair under anaesthesia.
- Why did the TERM Breech Trial change practice globally toward CS for term breech presentations?
CLINICAL PEARL
The decision to proceed to CS from a failed instrumental delivery must be made early and definitively — not after three failed vacuum pop-offs plus two forceps attempts. Sequential use of vacuum followed by forceps (or vice versa) substantially increases neonatal intracranial morbidity, and there is never justification for trying both instruments on the same patient at the same sitting. The correct decision tree is: attempt instrumental delivery once with one instrument, assess progress after two pulls, and if there is no descent or if the situation is deteriorating, move to CS. The phrase every registrar learns and every student should know is: 'If in doubt — cut.' Assisted delivery is time-limited and has no prize for persistence.
SELF-CHECK
After a ventouse delivery, the neonate's scalp has a diffuse, boggy, fluctuant swelling that crosses the sagittal suture and appears to be enlarging over the first hour of life. The baby is pale and has a heart rate of 170 bpm. What is the most likely diagnosis and immediate action?
A. Chignon from vacuum cup — normal, reassure parents, no action needed
B. Cephalhaematoma — self-limiting, observe for jaundice in 24–48 hours
C. Subgaleal haemorrhage — neonatal emergency; alert paediatric team immediately, IV access and blood volume support
D. Caput succedaneum — pre-existing labour scalp oedema, resolves in 48 hours
Reveal Answer
Answer: C. Subgaleal haemorrhage — neonatal emergency; alert paediatric team immediately, IV access and blood volume support
A diffuse, boggy swelling that crosses suture lines, is enlarging, and is associated with pallor and tachycardia is subgaleal haemorrhage — a neonatal emergency. Blood accumulates in the virtual space beneath the epicranial aponeurosis, which can accommodate up to 40% of the neonate's blood volume. Urgent paediatric resuscitation is required. Cephalhaematoma is firm, does not cross suture lines, and does not cause haemodynamic instability. Chignon is a firm dome directly inside the cup imprint and is not enlarging. Caput is present at birth, does not enlarge postnatally.