Page 14 of 27
OG37.6 | Outlet Forceps, Vacuum and Breech Delivery Observation — SDL Guide (Part 2)
Vacuum Extraction (Ventouse) — Observing the Technique
Vacuum extraction with a ventouse (suction) cup is an alternative to forceps that many obstetricians prefer because it causes less maternal perineal trauma and allows more physiological descent of the fetal head. The principles of cup placement and traction direction mirror those of forceps, but the mechanics are different — and the observer must understand what 'correct cup placement' means to follow the procedure.
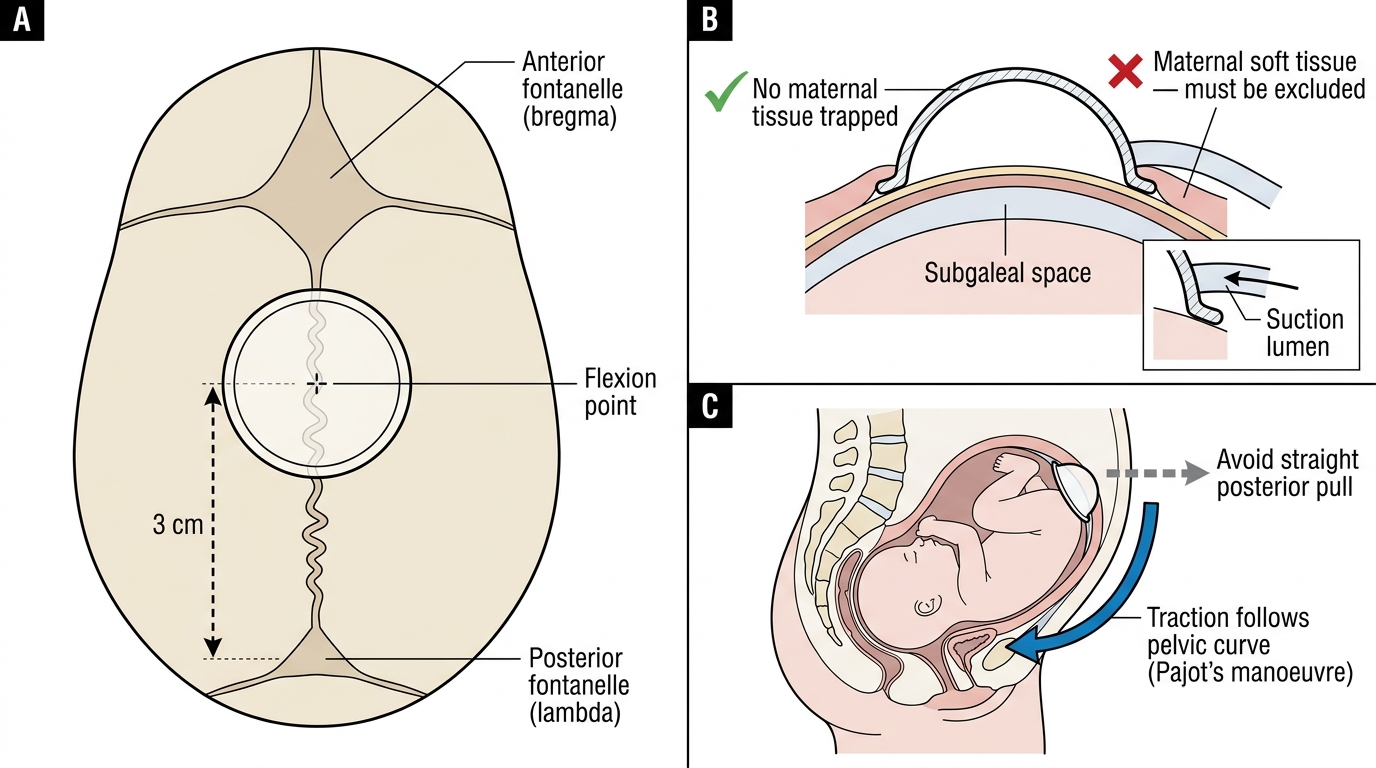
The flexion point of the fetal head is the key anatomical landmark for cup placement. It is located on the sagittal suture, approximately 3 cm anterior to the posterior fontanelle (and 6 cm from the anterior fontanelle). Cup placement at the flexion point ensures that traction flexes the head (reducing the presenting diameter from the suboccipitofrontal to the suboccipitobregmatic — a reduction of approximately 1 cm), which is the optimal position for delivery. Placement too far forward (near the anterior fontanelle) results in deflexion and a larger presenting diameter, increasing the traction force required and the risk of cup detachment.
Technique observed:
Step 1 — Cup selection and preparation. A silicone or metal cup is selected based on availability and indication. The silicone cup (Kiwi OmniCup) is more flexible and easier to apply in non-OA positions; the metal cup allows greater traction force for difficult cases. The cup is connected to a suction device (manual or electric pump).
Step 2 — Cup insertion and positioning. The cup is introduced into the vagina and placed on the fetal scalp at the flexion point (posterior to the anterior fontanelle, on the sagittal suture). No maternal tissue should be caught under the cup rim — the operator sweeps a finger around the entire cup circumference to verify this.
Step 3 — Negative pressure build-up. Suction is applied gradually: from 0 to the target pressure in two steps (start at 0.2 kg/cm2, then increase to 0.6 kg/cm2 for metal, up to 0.8 for difficult cases) over 1–2 minutes. This creates the chignon — a dome of scalp tissue drawn up into the cup, which is normal and resolves within 48 hours. Watch the anaesthesiologist or midwife managing the pressure; premature high-pressure application risks cup detachment and scalp injury.
Step 4 — Traction. Traction is applied in the axis of the pelvis, coordinated with uterine contractions and maternal pushing, exactly as with forceps. The Pajot-like downward then upward trajectory is followed. Detachment of the cup ('pop-off') during traction indicates either malposition, excessive caput, or inadequate suction — the cup is reapplied. However, after three pop-offs or three pulls with no descent, the procedure should be abandoned and CS considered.
Step 5 — Delivery. As the vertex crowns, suction is released and the cup removed. Head delivery proceeds as per normal.
Ventouse Cup Placement: Flexion Point, Rim Check, and Traction Direction
SELF-CHECK
During ventouse extraction, the cup pops off ('detaches') three times despite correct placement and adequate pressure. Progress has been minimal — only 1 cm of descent over 30 minutes. What should the operator do?
A. Switch to forceps for a combined forceps-and-vacuum delivery to maximise traction
B. Increase negative pressure to the maximum possible and attempt further traction
C. Abandon instrumental delivery and proceed to emergency caesarean section
D. Ask an assistant to apply stronger fundal pressure while traction continues
Reveal Answer
Answer: C. Abandon instrumental delivery and proceed to emergency caesarean section
Three cup detachments (pop-offs) without descent indicate that instrumental delivery is failing — likely due to CPD, malposition not correctable by vacuum alone, or excessive caput preventing cup adhesion. Sequential use of vacuum then forceps (or vice versa) significantly increases neonatal morbidity and is not recommended. The correct decision is to abandon vaginal instrumental delivery and proceed to emergency CS. Increasing pressure beyond safe limits risks scalp injury and subgaleal haemorrhage.
Breech Delivery — Observing Assisted Breech and Manoeuvres
Vaginal breech delivery is increasingly uncommon in modern obstetric practice following the TERM Breech Trial (Hannah et al., Lancet 2000), which demonstrated that planned CS for term singleton breech presentation resulted in significantly lower perinatal mortality and neonatal morbidity than planned vaginal breech delivery. As a result, most term breech presentations in hospitals with available CS capacity are now delivered by planned CS. However, vaginal breech delivery still occurs — in unbooked or precipitous labours, in preterm deliveries where the body delivers before the surgeon can reach the patient, in multiple pregnancy with a second twin that presents breech, and in centres with specific expertise and appropriate patient selection. The final-year student must understand the types of breech presentation, the basic manoeuvres, and the critical point at which help must be called.
Types of breech presentation:
- Frank breech (65% of breech presentations): hips flexed, both knees extended — the most favourable for vaginal delivery as the buttocks form a relatively smooth presenting part
- Complete breech (10%): hips and knees both flexed in a 'tailor' position — also manageable vaginally in appropriate cases
- Footling/incomplete breech (25%): one or both feet present — the highest risk type as the foot does not dilate the cervix adequately, and cord prolapse is a serious risk. Footling breech is generally not suitable for planned vaginal delivery.
Observing assisted vaginal breech delivery — general principles:
The key principle of vaginal breech delivery is 'hands off the breech' — the body should be allowed to deliver spontaneously by gravity and uterine contractions, with minimal intervention, until the shoulders and arms have delivered. Handling the breech prematurely stimulates the fetus to breathe before the head is delivered (risking aspiration) and may cause umbilical cord compression. The operator only intervenes when the umbilicus has delivered (the cord is accessible), when arm delivery is needed, or when the after-coming head must be managed.
Lovset's manoeuvre (for extended arms): If the fetal arms are extended upward (splinted by the uterine wall) rather than folded across the chest, they cannot be delivered by the usual downward sweep. The operator grasps the fetal pelvis bimanually and rotates the trunk 180 degrees so that the posterior arm (which is in the wider posterior pelvis) comes into the anterior position. By rotating back 180 degrees in the opposite direction, both arms can be delivered in sequence. The observer watches the operator's hands on the pelvis — NOT on the body or limbs.
Burns-Marshall manoeuvre (for after-coming head): After the body is delivered to the level of the nape, the baby is allowed to hang by its own weight for a few seconds. The operator then grasps the fetal ankles and swings the trunk upward in a wide arc over the maternal abdomen, while an assistant applies suprapubic pressure. This manoeuvre flexes and delivers the after-coming head by allowing it to negotiate the pelvic curve.
Mauriceau-Smellie-Veit (MSV) manoeuvre: The more controlled technique for the after-coming head. The operator places the fetal body across their forearm, with the index and middle fingers of that hand placed on the fetal malar bones (cheekbones, not the jaw — pressure on the jaw risks mandibular fracture; pressure on the cheekbones promotes flexion). The other hand is placed on the fetal occiput with the middle finger applying supraoccipital pressure to flex the head. The assistant provides fundal pressure. The operator then gently applies downward traction, following the pelvic curve, to deliver the occiput under the symphysis. The head delivery is controlled — never rapid — to prevent sudden decompression causing intracranial haemorrhage.
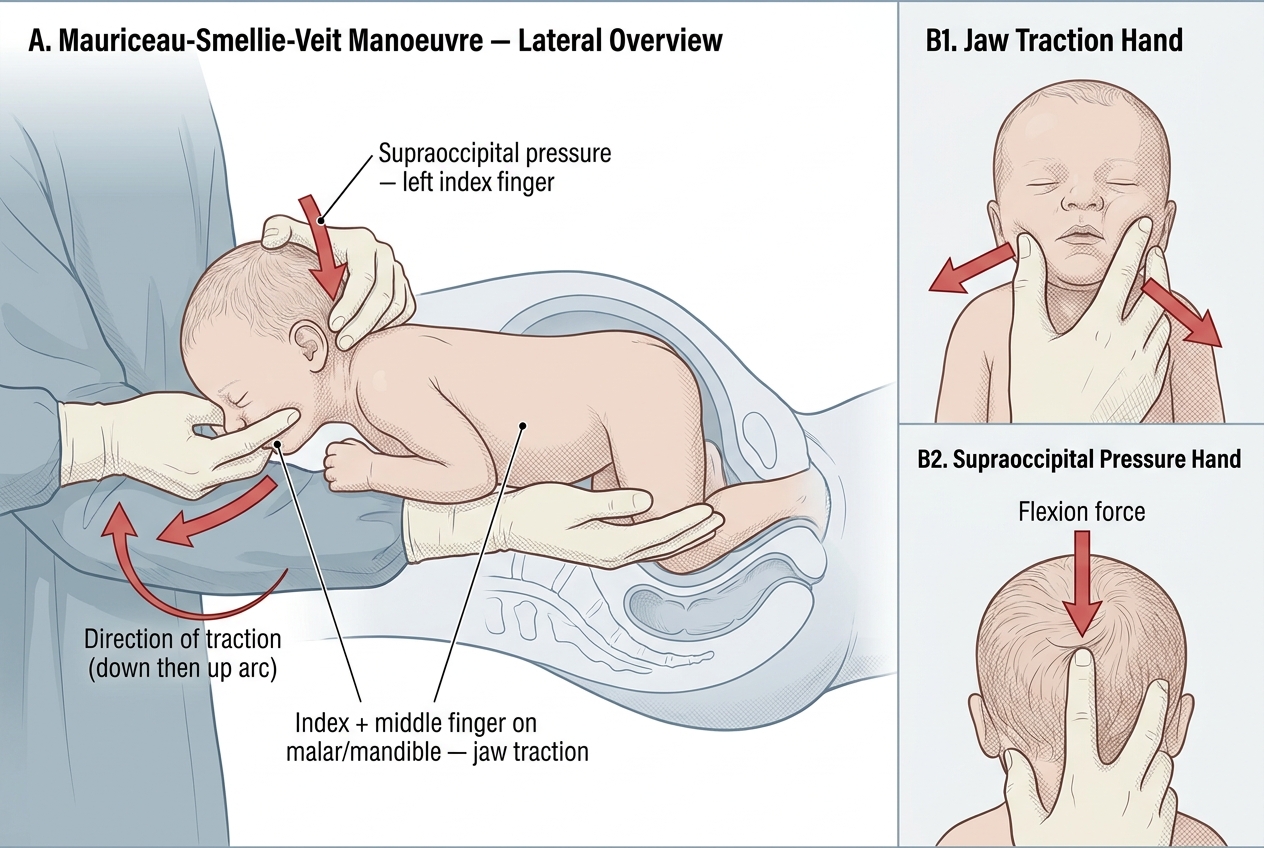
Mauriceau-Smellie-Veit Manoeuvre — After-Coming Head in Breech Delivery
Intraoperative Findings — What the Observer Interprets
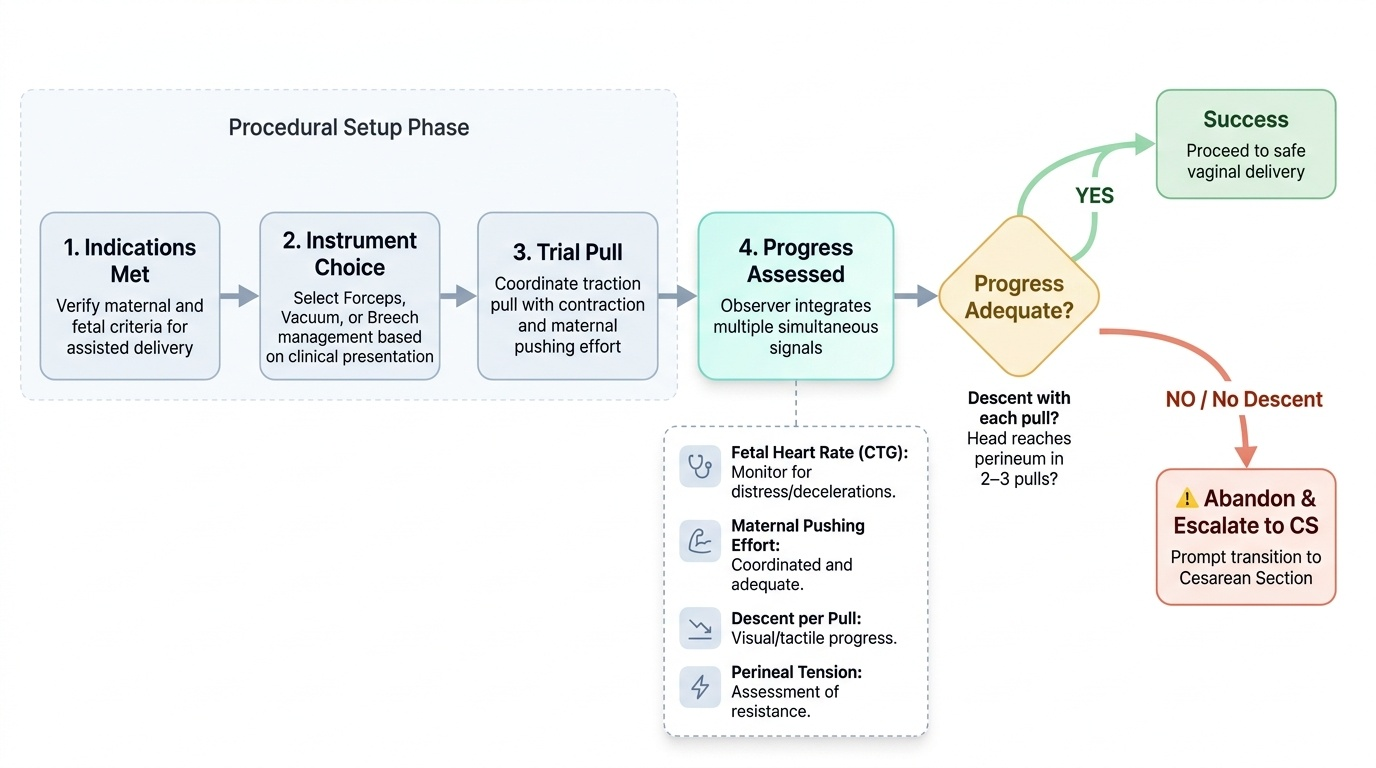
Reading the progress of an assisted delivery — whether forceps, vacuum, or breech — requires the observer to integrate multiple simultaneous signals: the fetal heart rate on the CTG, the maternal pushing effort, the degree of descent per pull, and the perineal tension. Understanding what 'progress' looks like helps the observer assess whether the procedure is going well or whether escalation to CS is needed.
For forceps and vacuum: Descent should occur with each contraction and traction pull. In a successful outlet delivery, the head should reach the perineum within two or three pulls. If there is no descent after two pulls, the operator reassesses the application and station. If there is still no descent after three pulls, the procedure is failing and CS should be arranged. Progress is measured not just by descent (the head moving downward) but by rotation (the position moving from OT or OP toward OA) and extension (the head deflexing as it clears the symphysis).
For breech delivery: The observer should watch the cord once it appears at the vulva. If the cord appears thin, pale, or pulseless — cord compression is occurring and delivery must be completed urgently. The most dangerous moment in breech delivery is entrapment of the after-coming head by an incompletely dilated cervix (usually in a preterm breech where the body delivers quickly through a not-fully-dilated cervix). If this occurs, the operator will attempt MSV manoeuvre with maximum downward traction; if the head is still trapped, emergency assistance is called immediately and the anaesthetic team is alerted for possible CS.
Recognising a failed instrumental delivery: Signs that the procedure should be abandoned include: three pulls without descent; cup detachment three times; persistent fetal bradycardia without recovery between pulls; failure to maintain application despite correct technique. The decision to proceed to CS should be made early — not after prolonged failed attempts that exhaust both the mother and the fetus.
Provided image
SELF-CHECK
A 31-year-old grand multipara arrives at the labour room in advanced labour with a well-grown baby in frank breech presentation. She is fully dilated and the breech has descended onto the perineum. There is no time to arrange a CS. As the baby delivers spontaneously to the level of the umbilicus, what is the most important principle guiding the observer and the medical team at this moment?
A. Apply traction to the fetal legs immediately to speed up delivery
B. Hands off the breech — allow the body to deliver by gravity and contractions until the shoulders are accessible; minimal intervention until then
C. Apply forceps to the after-coming head as soon as the body is delivered
D. Insert a hand into the uterus to reposition the baby into a vertex presentation
Reveal Answer
Answer: B. Hands off the breech — allow the body to deliver by gravity and contractions until the shoulders are accessible; minimal intervention until then
The fundamental principle of assisted vaginal breech delivery is 'hands off the breech' — the body should be allowed to deliver spontaneously by gravity and uterine contractions, with minimal intervention, until the umbilicus and then the shoulders have delivered. Early handling stimulates the fetus to breathe before the head is delivered, risking aspiration, and premature traction on the trunk risks trapped arms or cord compression. Intervention is reserved for extended arms (Lovset's) and the after-coming head (Burns-Marshall or MSV). Attempting to reposition a descending breech vaginally is not feasible.