Page 20 of 29
OG7.1 | Maternal Physiological Changes in Pregnancy — SDL Guide
Learning Objectives
- Describe the anatomical and functional changes in the genital tract and breast during pregnancy
- Explain the cardiovascular adaptations of pregnancy including changes in cardiac output, blood volume, and vascular resistance
- Describe the haematological changes including physiological anaemia, iron and folate demands, and hypercoagulability
- Explain respiratory changes and their physiological basis
- Describe renal adaptations including changes in GFR and implications for laboratory interpretation
- Describe gastrointestinal and endocrine/metabolic changes during pregnancy
- Apply knowledge of normal physiological ranges in pregnancy to clinical decision-making
INSTRUCTIONS
Pregnancy is not a disease — it is a state of profound physiological adaptation. The maternal body remodels its cardiovascular, haematological, respiratory, renal, and endocrine systems to support a rapidly growing feto-placental unit while preserving the mother's own homeostasis. Understanding these changes is essential: a laboratory result that would prompt urgent action in a non-pregnant patient may be completely normal in pregnancy, and vice versa. This module systematically maps each system's transformation, the hormones that drive it, and the clinical decisions these changes inform.
References
- DC Dutta's Textbook of Obstetrics, 9th ed, Chapter 5 — Changes in the Maternal Body During Pregnancy (textbook)
- Cunningham FG et al. Williams Obstetrics, 25th ed, Chapter 4 — Maternal Physiology (textbook)
- Shaw's Textbook of Gynaecology, 17th ed (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old primigravida at 28 weeks gestation presents to the antenatal clinic. Her haemoglobin is 10.2 g/dL — below the laboratory's non-pregnant reference range of 12–16 g/dL. Her serum creatinine is 0.5 mg/dL, her resting pulse is 88 bpm, and she reports occasional breathlessness on climbing stairs. She is otherwise well, with a normally growing fetus. Should you treat her anaemia aggressively? Is her tachycardia pathological? Is her breathlessness a red flag? The answer to all three questions depends entirely on knowing what is normal in pregnancy — and the answer is not the same as outside it.
WHY THIS MATTERS
Maternal physiological changes underpin virtually every clinical decision in obstetric care. Misinterpreting dilutional anaemia as iron deficiency leads to over-investigation and anxiety; missing true anaemia by applying non-pregnant thresholds leads to under-treatment. A blood pressure of 130/85 mmHg early in pregnancy, when SVR has fallen and BP should be at its lowest, may actually signal emerging hypertension. The renal GFR nearly doubles, meaning that a creatinine of 0.9 mg/dL — entirely unremarkable outside pregnancy — warrants investigation in a pregnant woman. Drug dosing, anticoagulation decisions, VTE risk stratification, and interpretation of every biochemical panel depend on knowing these shifts. These are not abstract physiology facts — they are daily clinical tools.
RECALL
Before exploring how pregnancy changes the body, recall the non-pregnant baselines from your Physiology course. Cardiac output at rest is approximately 5 L/min, driven by heart rate (~70 bpm) and stroke volume (~70 mL). GFR is roughly 100–120 mL/min, maintaining serum creatinine around 0.6–1.0 mg/dL. Tidal volume at rest is about 500 mL; FRC (functional residual capacity) is the air remaining after a normal exhalation. Normal haemoglobin is 12–16 g/dL in women. Recall that progesterone is a smooth-muscle relaxant and respiratory stimulant, and that oestrogen promotes fluid retention and vascular growth. These baseline values and hormonal principles form the foundation for understanding every change that follows.
Why the Body Transforms: Clinical Relevance of Maternal Physiology
Pregnancy imposes a series of physiological demands that no other life stage replicates. The feto-placental unit is a low-resistance vascular bed that must receive a sustained, high-volume blood supply — at term, the uterus alone receives approximately 500–700 mL/min of blood, up from less than 50 mL/min before conception. The fetus must be supplied with oxygen and nutrients continuously without competing with maternal organ perfusion. The fetus generates metabolic waste that must be cleared through maternal kidneys. The enlarging uterus mechanically displaces abdominal organs and the diaphragm. The placenta secretes hormones — progesterone, oestrogen, hCG, human placental lactogen (hPL) — that remodel maternal physiology from the earliest weeks.
These adaptations are purposeful and predictable. They occur in a defined temporal sequence: cardiovascular expansion begins in the first trimester and peaks around 28–32 weeks; renal GFR rises by the end of the first trimester; haematological expansion follows the cardiovascular lead. Understanding this timeline helps clinicians interpret findings against gestational age, not just against non-pregnant norms. A haematocrit of 32% at 28 weeks is physiological; the same value at 6 weeks postpartum requires investigation.
The central clinical lesson is this: physiological changes of pregnancy are adaptive responses, not pathological departures. They serve survival of both mother and fetus. The clinician's task is to distinguish these predictable normal shifts from early signals of pathology — pre-eclampsia, gestational diabetes, anaemia of iron deficiency — that can be superimposed on an otherwise normal physiological state.
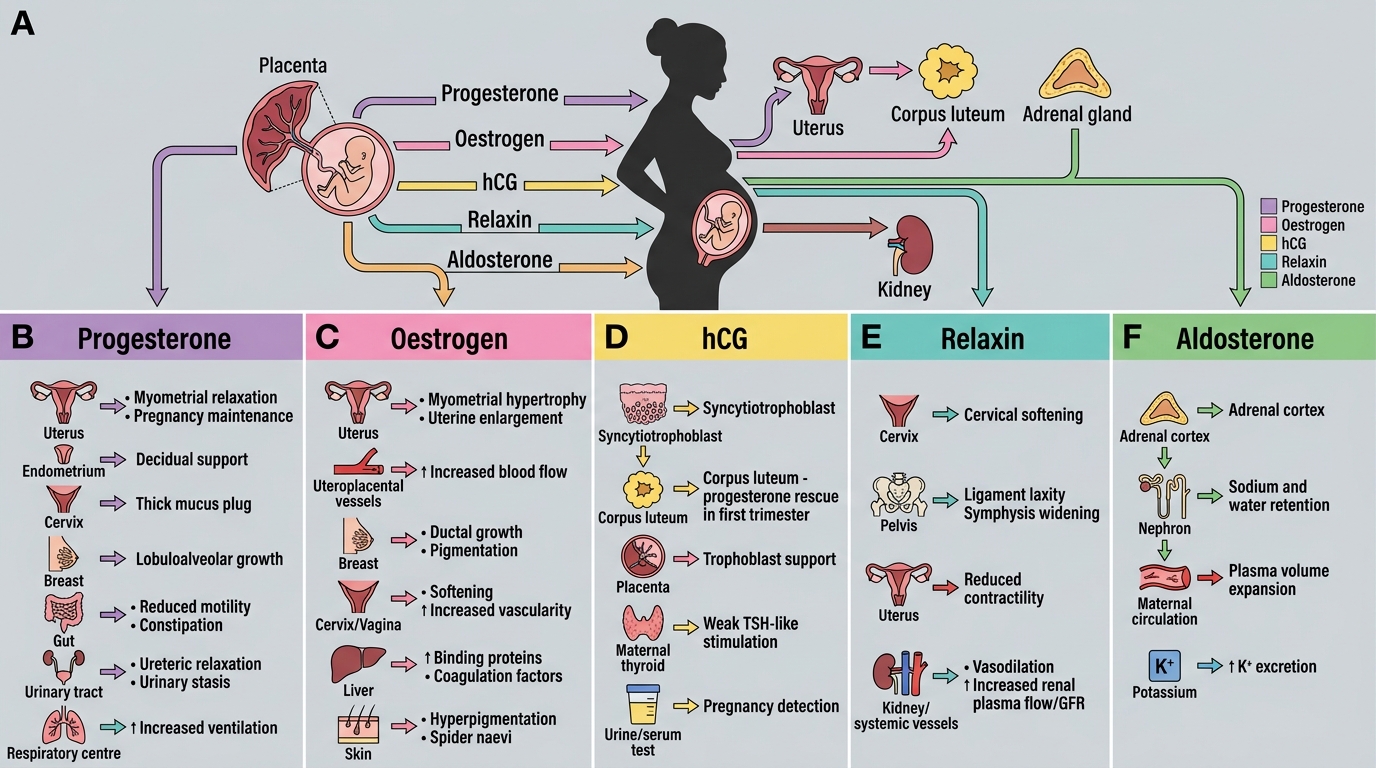
Pregnancy Hormones and Systemic Physiological Effects
Genital Tract and Breast Changes
The genital tract undergoes dramatic structural and functional remodelling during pregnancy, driven primarily by oestrogen and progesterone, and further supported by increased blood flow. These changes are the source of several classical clinical signs that have diagnostic value in early pregnancy examination.
The uterus undergoes the most spectacular transformation. Before pregnancy it weighs approximately 60–80 g and has a capacity of about 10 mL. By term it weighs 1,000–1,200 g (20-fold increase) with a capacity of 5–10 litres. Growth occurs by hypertrophy of existing myometrial smooth muscle fibres (driven by oestrogen) and by hyperplasia in early pregnancy. The fibromuscular wall softens progressively. Braxton Hicks contractions — painless, irregular uterine tightenings — begin from about 6 weeks (imperceptible early, palpable from mid-trimester), representing coordinated but non-progressive myometrial activity that prepares the uterus for labour. The decidua (the specialised endometrium of pregnancy) lines the uterine cavity and provides immunological tolerance of the semi-allogeneic fetus.
The cervix is the site of three classical pregnancy signs: Goodell's sign (softening of the cervix, felt from 6–8 weeks — the non-pregnant cervix has the consistency of a nasal tip; in pregnancy it softens to lip consistency), Chadwick's sign (bluish-violet discolouration of the cervix and vaginal walls from vascular engorgement and venous congestion, visible from 8 weeks), and Hegar's sign (compressibility and softening of the isthmus of the uterus — felt on bimanual examination at 6–10 weeks, a classic early pregnancy sign). The cervix also develops an endocervical mucus plug (operculum) that seals the cervical canal and provides a physical and immunological barrier to ascending infection throughout pregnancy. Loss of the mucus plug ("show") near term signals cervical preparation for labour.
The vagina shows increased vascularity with a characteristic bluish-pink hue (part of Chadwick's sign). Vaginal secretions increase (leucorrhoea of pregnancy), with a lower pH (~3.5–4.0) due to glycogen breakdown by Lactobacilli — providing protection against ascending infection. Vaginal walls become congested and hypertrophied.
The breasts enlarge from the first trimester under the influence of oestrogen (ductal growth) and progesterone (alveolar/lobular development). Montgomery's tubercles — hypertrophic sebaceous glands on the areola — become prominent from 8 weeks; they secrete a lubricating, bacteriostatic fluid that protects the nipple during breastfeeding. The areola darkens (primary areola; a paler secondary areola develops around it). From approximately 12–16 weeks, colostrum — the precursor to mature breast milk, rich in secretory IgA, lactoferrin, and protein — can be expressed. Full lactogenesis (milk production) is suppressed during pregnancy by high progesterone; it begins after delivery when progesterone withdrawal unmasks prolactin's lactogenic action.
| Sign | System | Description | Approximate gestation first detectable |
|---|---|---|---|
| Goodell's sign | Cervix | Cervical softening (lip consistency) | 6–8 weeks |
| Chadwick's sign | Cervix/vagina | Bluish-violet discolouration | 8 weeks |
| Hegar's sign | Uterine isthmus | Isthmic compressibility on bimanual examination | 6–10 weeks |
| Braxton Hicks | Uterus | Painless irregular contractions | 6 weeks (palpable mid-trimester) |
| Montgomery's tubercles | Breast areola | Hypertrophic sebaceous glands, prominent | 8 weeks |
Cardiovascular Changes
The cardiovascular system undergoes the most dramatic functional changes of any organ system in pregnancy. These changes begin within weeks of conception and are driven primarily by the low-resistance uteroplacental circulation and the vasodilatory effects of progesterone, nitric oxide, and oestrogen.
Cardiac output (CO) increases by 30–50% above non-pregnant values, rising from approximately 5 L/min to 7–8 L/min by 28–32 weeks gestation. This increase is achieved by two mechanisms: (1) stroke volume rises first (by 10–15%), driven by increased preload from plasma volume expansion, and reaches its peak in the second trimester; (2) heart rate increases progressively throughout pregnancy by 10–20 bpm (from ~70 to ~85–90 bpm at term), contributing substantially to CO in the third trimester. After 28–32 weeks, CO may plateau or slightly fall as the enlarging uterus begins to compress the inferior vena cava in the supine position, reducing venous return — this is aortocaval compression, which can cause supine hypotensive syndrome in the third trimester (pallor, bradycardia, dizziness when lying flat). Lateral positioning restores venous return.
Systemic vascular resistance (SVR) falls by 20–30% from early pregnancy, driven by progesterone-mediated smooth muscle relaxation, nitric oxide-induced vasodilation, and the development of the low-resistance uteroplacental bed. This fall in SVR is why blood pressure actually decreases in the first and second trimesters (typically nadir at 20–24 weeks) before rising slightly in the third trimester back toward pre-pregnancy levels. A systolic BP of 100–110 mmHg at 20 weeks is normal — not cause for concern. The clinical implication: any BP ≥140/90 after 20 weeks must be taken seriously as it represents a rise against this backdrop of expected low pressure (pre-eclampsia threshold).
Blood volume expands markedly: plasma volume increases by 45–50% (from ~2,600 mL to ~3,800 mL), beginning in the first trimester and peaking at 32–34 weeks. This expansion exceeds the increase in red cell mass (~25% rise), producing a fall in haematocrit and haemoglobin — the basis of physiological (dilutional) anaemia (see Haematological Changes section).
Structural and auscultatory changes accompany these haemodynamic shifts. The heart is displaced upward and to the left by the diaphragm. A physiological systolic ejection murmur (grade 1–2/6, heard at the left sternal edge, due to increased flow through the pulmonary and tricuspid valves) is normal in over 90% of pregnant women and should not trigger unnecessary investigation. True pathological murmurs are diastolic, loud (grade 3+), or associated with symptoms. S1 may be loud; a third heart sound (S3) is common and physiological in pregnancy. The ECG may show left axis deviation and a non-specific ST or T-wave change due to cardiac displacement.
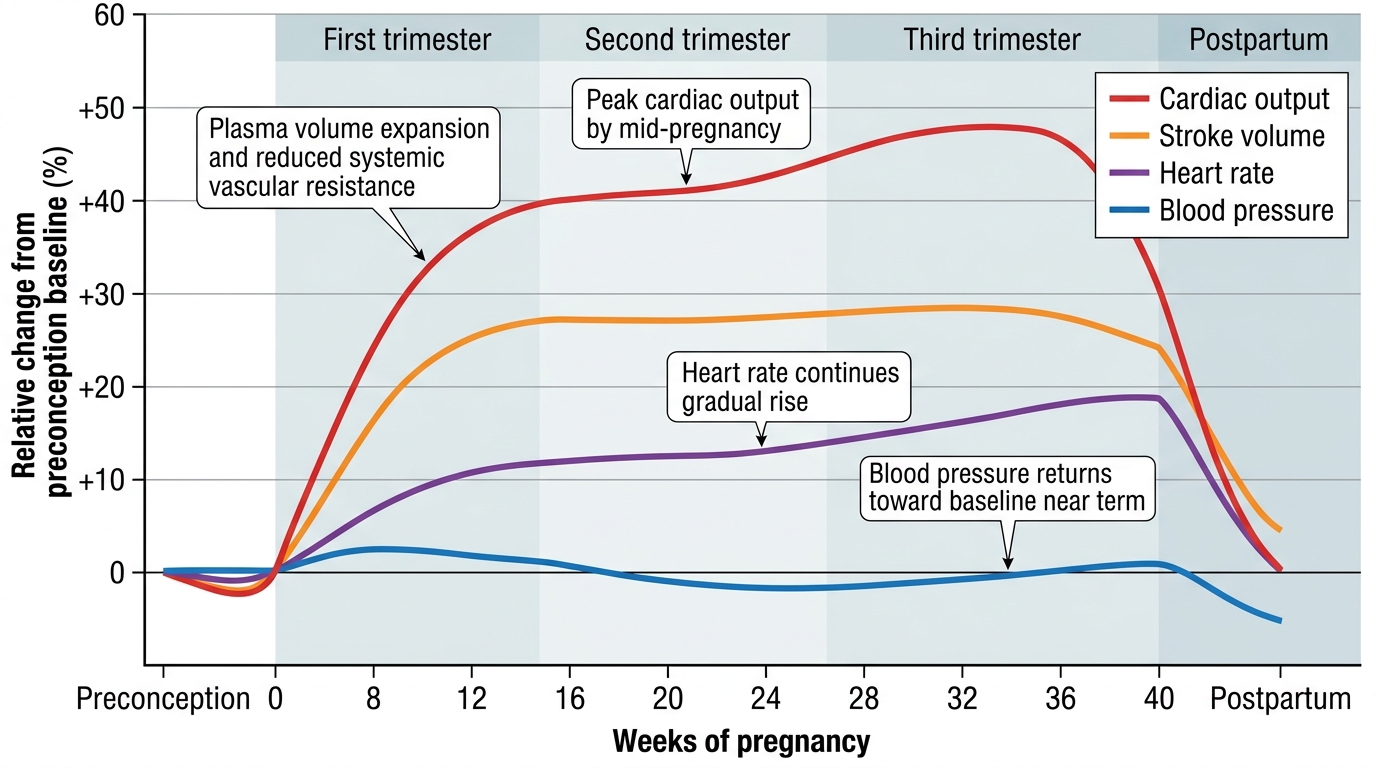
Maternal Cardiovascular Changes Across Pregnancy