Page 21 of 29
OG7.1 | Maternal Physiological Changes in Pregnancy — SDL Guide (Part 2)
Haematological Changes
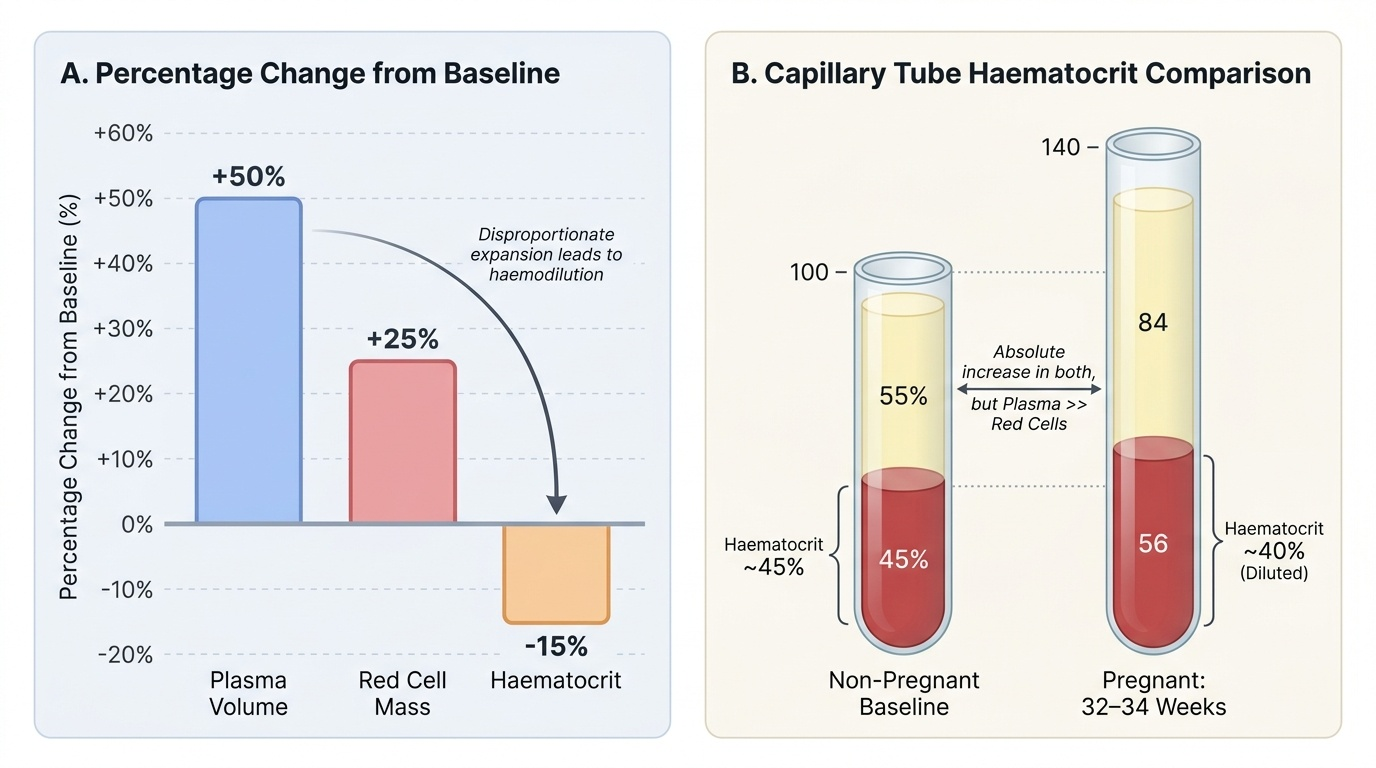
The haematological system adapts to the increased circulatory demands of pregnancy through expansion of blood volume components — but plasma and red cells expand at different rates, with significant clinical consequences. Simultaneously, the coagulation system shifts to a pro-thrombotic state, a protective mechanism against haemorrhage at delivery that also carries the risk of pathological thrombosis.
Plasma volume expands by approximately 45–50% above the non-pregnant baseline by 32–34 weeks. This is the larger component of blood volume expansion. Red cell mass expands by approximately 25% above baseline — substantially less than the plasma expansion. This disproportionate increase means that haematocrit and haemoglobin concentration fall despite an absolute increase in red cell mass. This is physiological (dilutional) anaemia of pregnancy — not a deficiency state, not pathological in itself, but a normal haemodilutional consequence of the greater plasma expansion. The World Health Organization (WHO) defines anaemia in pregnancy as haemoglobin <11 g/dL in the first and third trimesters, and <10.5 g/dL in the second trimester — accounting for this dilutional nadir. Any haemoglobin above these thresholds, even if below the non-pregnant norm, does not require treatment for anaemia per se.
However, the absolute increase in red cell mass does create a genuine increased demand for iron and folate. Iron requirements increase to approximately 27 mg/day (vs 18 mg/day in non-pregnant women), reflecting expansion of maternal red cell mass, fetal red cell synthesis, and placental demands. Supplemental iron is recommended routinely in pregnancy in India. Folate requirements increase to 0.4–0.6 mg/day; in women at high risk for neural tube defects (previous NTD, anticonvulsant therapy), 4–5 mg/day is recommended.
The coagulation system undergoes a deliberate pro-thrombotic shift in preparation for placental separation and delivery. Fibrinogen increases markedly (from ~2–4 g/L to ~4–6 g/L by term) and is the single most important change. Factors VII, VIII, and X also increase substantially; Factor XII rises; von Willebrand factor increases. In contrast, protein S (a natural anticoagulant) falls progressively during pregnancy. Together, these changes create a hypercoagulable state (one arm of Virchow's triad, combined with venous stasis from uterine compression and reduced physical activity). This is adaptive — it limits haemorrhage at delivery. The clinical cost is a 5–10-fold increased risk of venous thromboembolism (DVT/PE) compared to non-pregnant women of the same age, a risk that persists into the puerperium.
Leucocyte count rises in pregnancy (from ~7,000 to ~9,000–12,000/µL), primarily due to neutrophilia. This is physiological and should not be misinterpreted as infection. In labour, counts can transiently reach 20,000–25,000/µL. Platelet count tends to fall slightly due to dilution and increased consumption, but remains within the normal range in uncomplicated pregnancy.
Provided image
Respiratory Changes
Pregnancy imposes increased ventilatory demands — the fetus requires oxygen and produces CO₂ that must be cleared by the maternal lungs — while simultaneously reducing the mechanical capacity of the thorax as the uterus elevates the diaphragm. The net result is a characteristic pattern of increased ventilation achieved through changes in tidal volume rather than respiratory rate, with predictable acid-base consequences.
Tidal volume (TV) increases by approximately 40% during pregnancy — from the non-pregnant resting value of ~500 mL to ~700 mL at term. This is the primary respiratory adaptation. Respiratory rate increases only slightly (from 15 to ~16–18 breaths/min). The combination produces a marked increase in minute ventilation (tidal volume × respiratory rate) by 30–50%. The drive for this increased ventilation comes from progesterone, which acts as a respiratory stimulant at the level of the central respiratory centres, lowering the threshold for CO₂-driven breathing. Progesterone also increases sensitivity to CO₂. This is why many pregnant women notice a feeling of dyspnoea even at rest — it is a direct hormonal effect, not cardiac or pulmonary disease.
Functional residual capacity (FRC) decreases by approximately 20% as the uterus elevates the diaphragm — it reduces both the expiratory reserve volume (ERV) and the residual volume (RV). Total lung capacity (TLC) is essentially unchanged or minimally reduced. Vital capacity (VC) and FEV₁ remain normal. The clinical consequence of reduced FRC is that oxygen reserves are diminished: pregnant women desaturate more rapidly during apnoea (e.g., at induction of anaesthesia) than non-pregnant women, making rapid-sequence intubation and pre-oxygenation especially critical in obstetric anaesthesia.
The acid-base consequence of increased ventilation is respiratory alkalosis: PaCO₂ falls from the non-pregnant ~40 mmHg to approximately 30–32 mmHg by term. To maintain near-normal pH (~7.44), the kidneys compensate by excreting bicarbonate — serum HCO₃⁻ falls from ~24 mEq/L to ~18–22 mEq/L. This compensated respiratory alkalosis means that an arterial blood gas showing PaCO₂ of 38–40 mmHg in a labouring woman is not normal — it suggests relative CO₂ retention and should prompt evaluation. The lower PaCO₂ also facilitates fetal CO₂ transfer across the placenta by maintaining a favourable CO₂ gradient.
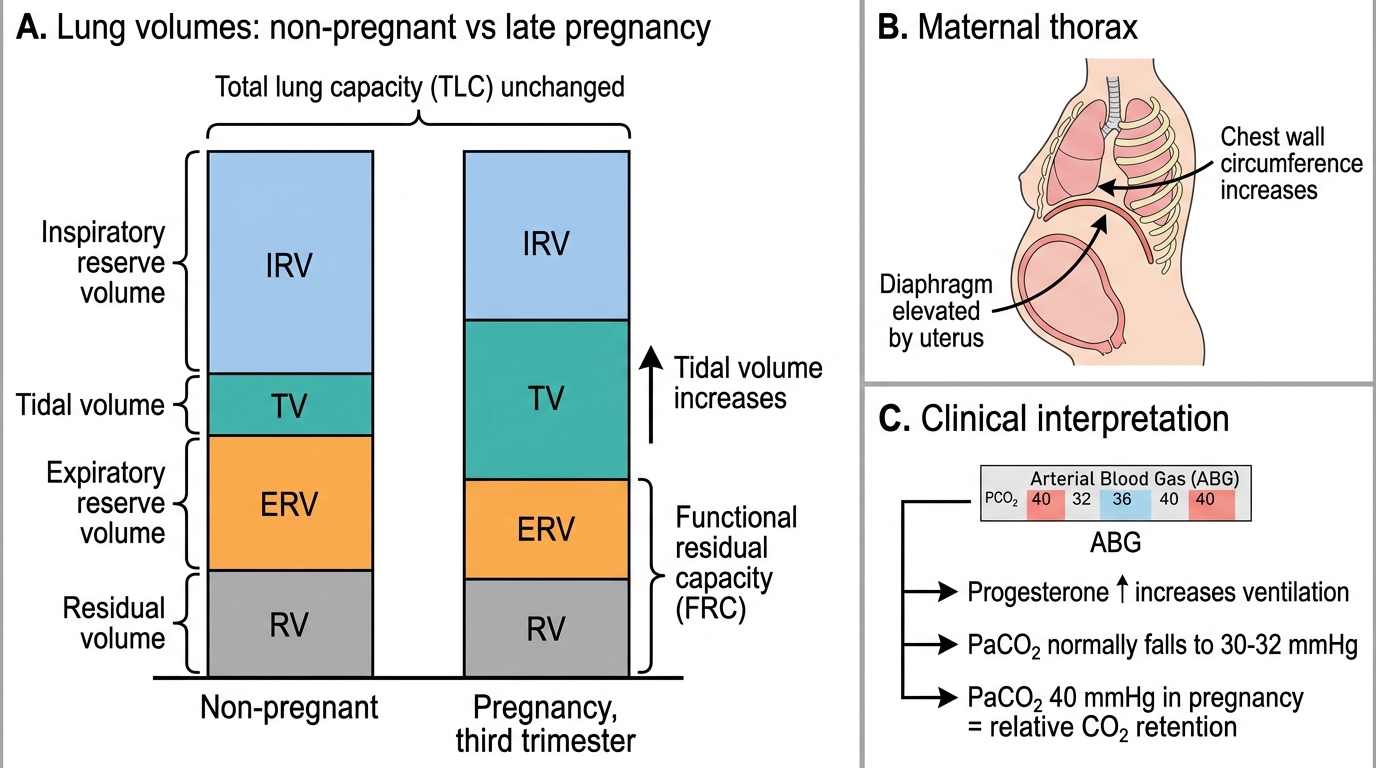
Lung Volume Changes in Pregnancy
SELF-CHECK
A pregnant woman at 30 weeks gestation has an arterial blood gas showing PaCO₂ of 40 mmHg and pH of 7.38. Which best describes this result?
A. Normal for pregnancy — CO₂ is within standard reference range
B. Relative CO₂ retention — PaCO₂ should be ~30–32 mmHg in pregnancy
C. Respiratory alkalosis — pH is below the pregnant norm of 7.44
D. Metabolic acidosis — bicarbonate has been over-excreted
Reveal Answer
Answer: B. Relative CO₂ retention — PaCO₂ should be ~30–32 mmHg in pregnancy
In pregnancy, progesterone drives increased minute ventilation, lowering PaCO₂ to approximately 30–32 mmHg. A PaCO₂ of 40 mmHg — the non-pregnant norm — represents relative CO₂ retention in a pregnant woman and may signal early respiratory failure, severe asthma, or impending deterioration. It should not be accepted as 'normal'.
Renal Changes
The kidneys undergo some of the most dramatic functional changes in pregnancy, expanding their filtration capacity to handle the increased metabolic load of both mother and fetus. These changes have direct and important consequences for the interpretation of every renal function test ordered in pregnancy.
Renal plasma flow (RPF) increases by approximately 50–80% during pregnancy, beginning in the first trimester and peaking in mid-pregnancy. Glomerular filtration rate (GFR) increases by approximately 40–60% above non-pregnant baseline (creatinine clearance rises from ~100 mL/min to ~140–160 mL/min). This functional hyperfiltration means that serum creatinine and urea are significantly lower than non-pregnant norms in an uncomplicated pregnancy. Normal serum creatinine in pregnancy is approximately 0.4–0.6 mg/dL (non-pregnant women: ~0.6–1.0 mg/dL); normal serum urea falls to ~2–4 mmol/L. A serum creatinine of 0.9 mg/dL that would be unremarkable in a non-pregnant woman is a marker of significant renal impairment during pregnancy. This is one of the most clinically important laboratory interpretation shifts in obstetrics.
Physiological glycosuria is common in pregnancy — up to 300 mg/day of glucose may be excreted in the urine even with normal blood glucose. This occurs because the rise in GFR exceeds the tubular reabsorptive capacity for glucose, so glucose 'spills' into the urine. Importantly, this means that a urine dipstick positive for glucose cannot reliably diagnose or exclude gestational diabetes — formal OGTT is required for GDM screening.
Ureteric dilation (hydroureter and hydronephrosis) is physiological in pregnancy, more marked on the right than the left (due to dextrorotation of the uterus and the right ovarian vein crossing the ureter). It results from both progesterone-mediated smooth muscle relaxation (reducing peristaltic tone) and mechanical compression by the gravid uterus. This physiological stasis predisposes to urinary tract infections (UTIs) — asymptomatic bacteriuria complicates 4–7% of pregnancies and, if untreated, can ascend to cause pyelonephritis in up to 30% of affected women (compared to <1–2% in non-pregnant women). Screening and treatment of asymptomatic bacteriuria is therefore routine antenatal care.
The kidneys are also involved in the sodium and water retention of pregnancy. Aldosterone levels rise markedly (stimulated by activation of the renin-angiotensin-aldosterone axis), promoting sodium and water retention. Despite this, plasma sodium falls slightly (~3–4 mEq/L) due to the disproportionately greater water retention — the pregnancy-adjusted normal for serum sodium is ~135–136 mEq/L.
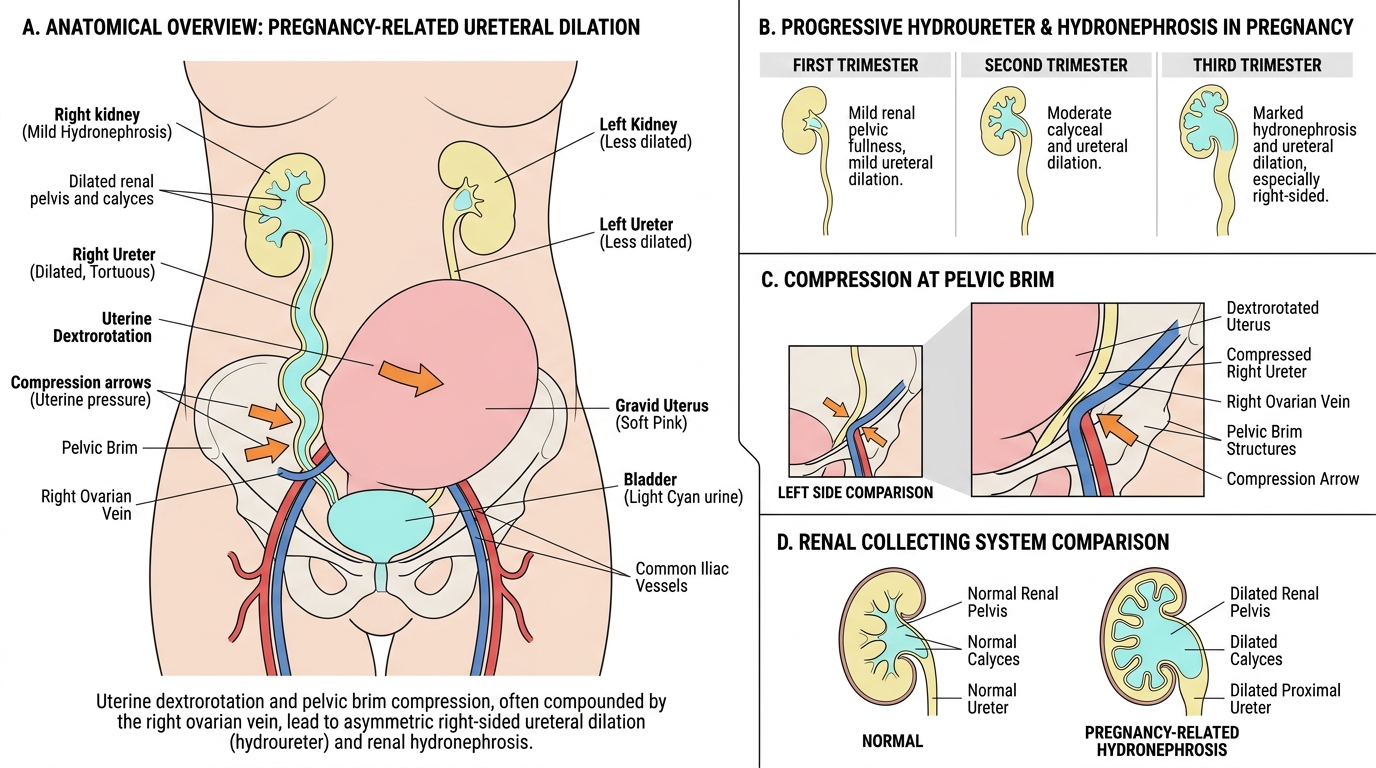
Pregnancy-Related Hydroureter and Hydronephrosis