Page 8 of 29
OG3.1 | Ovulation, Menstruation, Fertilization and Implantation — SDL Guide
Learning Objectives
- Describe the stages of folliculogenesis from primordial follicle to ovulation, and explain the hormonal triggers involved
- Outline the phases of the menstrual cycle and correlate endometrial changes with their hormonal drivers
- Compare oogenesis and spermatogenesis, including the timing and products of meiotic divisions
- Explain the sequential events of fertilisation, from capacitation and the acrosome reaction to zygote formation
- Describe blastocyst implantation, the implantation window, trophoblast invasion, and the role of hCG in early pregnancy maintenance
INSTRUCTIONS
Understanding the physiology of ovulation, menstruation, fertilisation and implantation is central to clinical obstetrics and gynaecology. This module explains the sequence of events from follicular recruitment to embryo implantation, equipping you to explain the basis of pregnancy tests, understand timing-based and hormonal contraception, and counsel patients about fertility and early pregnancy.
References
- Dutta DC. Textbook of Obstetrics, 10th ed., New Central Book Agency, 2021. Ch 3 (textbook)
- Cunningham FG et al. Williams Obstetrics, 26th ed., McGraw-Hill, 2022. Ch 5 (textbook)
- Ganong WF. Review of Medical Physiology, 26th ed., McGraw-Hill, 2019. Ch 25 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A couple presents to the gynaecology outpatient department after 18 months of unprotected intercourse without conception. The wife's cycles are regular, 28–30 days. Her basal body temperature chart shows a clear biphasic pattern — a sustained temperature rise after day 14, suggesting she is ovulating. The husband's semen analysis is normal. Yet conception has not occurred. The treating physician explains: 'Even when ovulation and sperm are both present, fertilisation and implantation are highly time-sensitive events with multiple potential failure points.' To understand why — and how to help this couple — you need to know exactly what happens from the moment a follicle ruptures to the moment a blastocyst burrows into the endometrium.
WHY THIS MATTERS
The physiology of the reproductive cycle underpins almost every clinical domain in OG. It explains why a pregnancy test turns positive (hCG from implanting trophoblast), how hormonal contraceptives work (suppressing the LH surge), when the 'safe period' is and why it is unreliable, why infertile couples undergo timed intercourse or intrauterine insemination, and how IVF protocols are designed around follicular recruitment. Every question about amenorrhoea, infertility, ectopic pregnancy, and early pregnancy failure requires this foundational knowledge.
RECALL
Bring to mind the hypothalamo-pituitary-ovarian axis from your physiology course. GnRH, released in pulses from the hypothalamus, stimulates the anterior pituitary to secrete FSH and LH. These gonadotrophins act on the ovarian follicles to drive oestrogen production, which feeds back both negatively (most of the cycle) and positively (the mid-cycle LH surge) on the hypothalamus and pituitary. Also recall from biochemistry that meiosis produces haploid cells (n=23) from diploid precursors (2n=46) through two sequential divisions, and that crossing-over during meiosis I creates genetic diversity. These concepts are the scaffolding on which this module builds.
Orientation: Why Understanding the Reproductive Cycle Matters
The human reproductive cycle represents one of the most precisely orchestrated hormonal sequences in the body. Over approximately 28 days (range 21–35 days), the hypothalamus, pituitary gland, ovary, and uterus coordinate through a cascade of hormonal signals to produce a single mature oocyte, prepare a receptive endometrium, and — if fertilisation occurs — create the conditions for embryo implantation. This is not merely an academic sequence; it is the physiological substrate for diagnosing and managing the most common conditions in clinical OG.
When a woman presents with a missed period, the clinician's first thought is whether the luteal phase has been extended by progesterone from a rescued corpus luteum — i.e., whether pregnancy-derived hCG is present. When a woman cannot conceive, the question is at which step the process fails: follicular development, ovulation, fertilisation, transport, or implantation? When a woman requests contraception, the choice among methods depends on understanding which step each method blocks. The physiology you are about to learn is directly translatable into clinical reasoning.
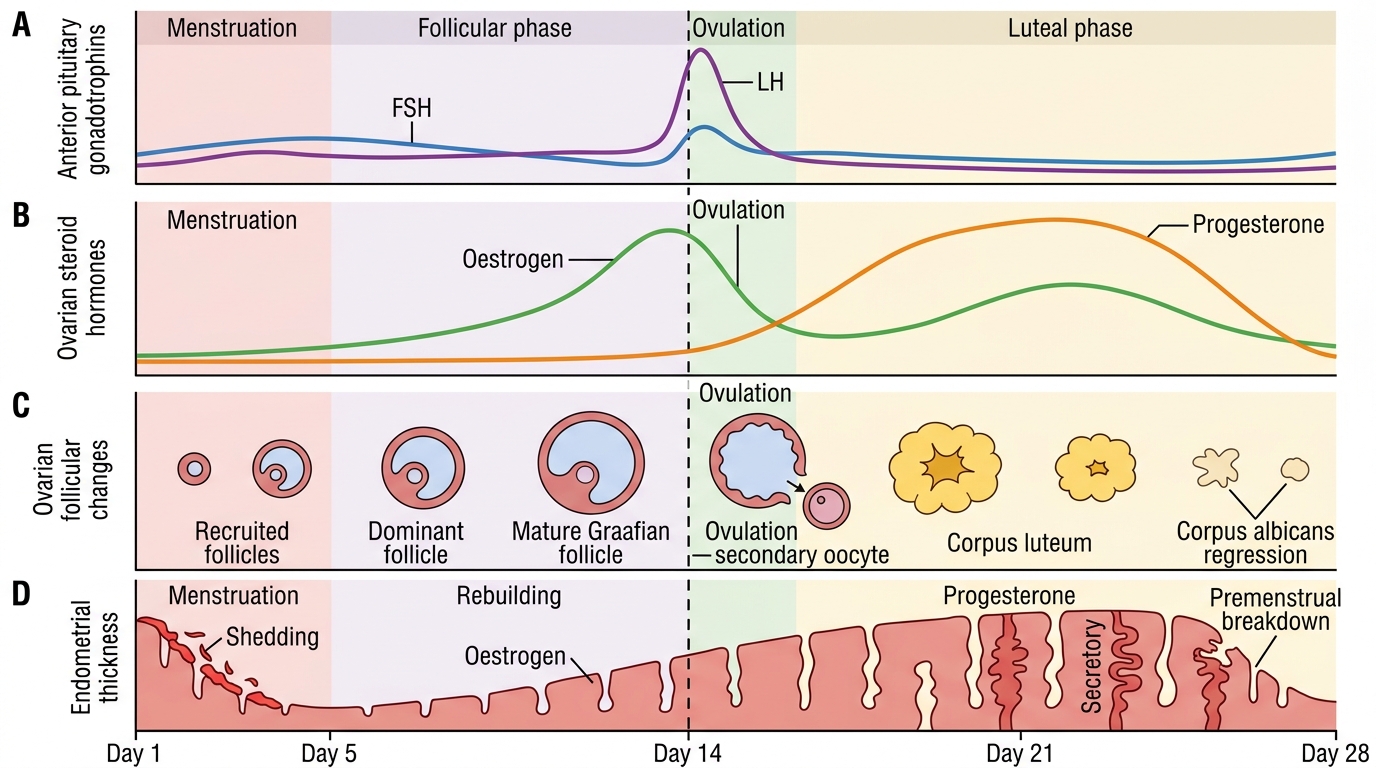
Integrated 28-Day Menstrual Cycle
Folliculogenesis, Ovulation and the Corpus Luteum
At birth, the ovaries contain approximately 1–2 million primordial follicles — each consisting of a primary oocyte arrested in the first meiotic prophase (diplotene stage) surrounded by a single layer of flattened granulosa cells. By puberty this pool has declined to approximately 400,000, largely through the continuous process of atresia that removes follicles regardless of gonadotrophin stimulation. Over an entire reproductive lifetime, only approximately 400 follicles will complete development and ovulate; the rest undergo atresia. This attrition is relentless — even before a girl is born, the process of follicular selection and loss has already begun. It is why ovarian reserve declines with advancing age, why fertility falls steeply after 35, and why a woman in her early 40s may have difficulty conceiving despite regular ovulation. The clinical relevance of this primordial follicle biology is therefore profound: ovarian reserve testing (AMH, antral follicle count) is an attempt to estimate how much of this finite pool remains.
Follicular development proceeds through a series of stages that are mostly gonadotrophin-independent early on but become critically FSH-dependent in the antral phase:
- Primordial follicle: arrested primary oocyte + flat granulosa cells
- Primary follicle: oocyte grows; granulosa cells become cuboidal; zona pellucida begins forming
- Secondary (preantral) follicle: multiple granulosa cell layers; theca cells differentiate around the outside; zona pellucida complete
- Tertiary (antral) follicle: fluid-filled antrum appears within the granulosa layer; FSH-dependent growth begins
- Graafian (dominant) follicle: one follicle is selected and grows to ~20 mm; oocyte + cumulus oophorus project into the antrum
The two-cell, two-gonadotrophin model explains how oestrogen is produced: FSH stimulates granulosa cells to convert androgens → oestradiol (via aromatase); LH stimulates theca cells to produce androgens (androstenedione, testosterone) that diffuse to granulosa cells. Rising oestradiol from the dominant follicle triggers the mid-cycle LH surge (positive feedback at the hypothalamus and anterior pituitary). The LH surge triggers:
1. Resumption of meiosis I in the oocyte (completion of the first meiotic division, producing the secondary oocyte + first polar body)
2. Luteinisation of granulosa cells
3. Follicular rupture (ovulation) approximately 36 hours after the onset of the LH surge
After ovulation, the ruptured follicle collapses and becomes vascularised, forming the corpus luteum — a temporary endocrine gland that secretes both progesterone and oestradiol. The corpus luteum has a fixed lifespan of approximately 14 days. If implantation does not occur, the corpus luteum regresses (luteolysis), progesterone falls, and menstruation begins. If implantation occurs, the syncytiotrophoblast produces human chorionic gonadotrophin (hCG), which binds LH receptors on the corpus luteum and rescues it — maintaining progesterone production until the placenta takes over at approximately 8–10 weeks (the 'luteal-placental shift').
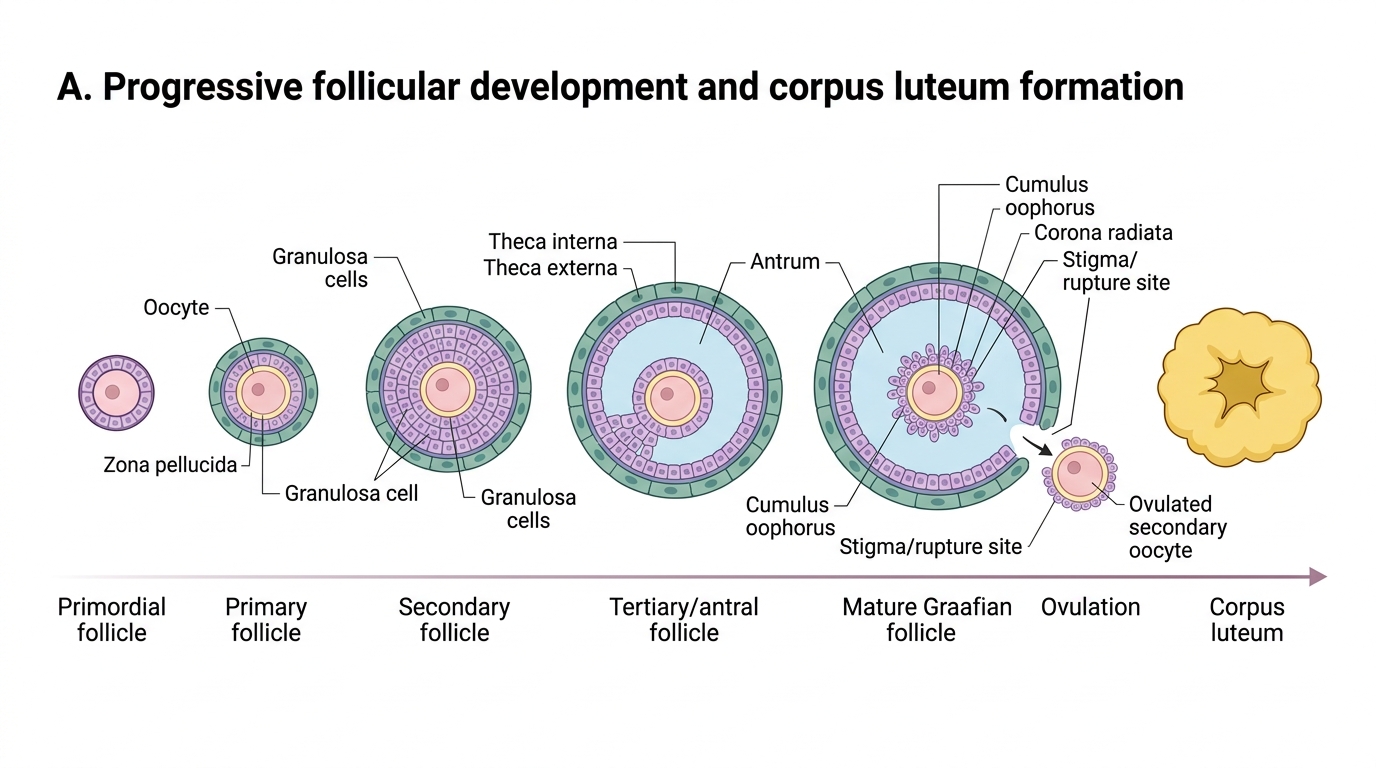
Progressive Follicular Development and Ovulation
SELF-CHECK
The LH surge triggers ovulation approximately how many hours after its onset, and which process in the oocyte does it simultaneously restart?
A. 12 hours; completion of meiosis II
B. 36 hours; resumption and completion of meiosis I
C. 48 hours; resumption of mitosis in the primary oocyte
D. 24 hours; formation of the zona pellucida
Reveal Answer
Answer: B. 36 hours; resumption and completion of meiosis I
The LH surge triggers follicular rupture (ovulation) approximately 36 hours after its onset. It simultaneously triggers resumption of meiosis I in the primary oocyte, which completes to yield the secondary oocyte and the first polar body. Meiosis II is then arrested at metaphase II — it completes only if a sperm penetrates the oocyte.
The Menstrual Cycle: Hormonal and Endometrial Changes
The menstrual cycle is traditionally described in two overlapping pairs of phases — the ovarian cycle (follicular and luteal) and the uterine/endometrial cycle (menstrual, proliferative, and secretory). These are driven by the same hormones and are inseparable in practice; understanding their synchrony is essential for interpreting investigations such as timed endometrial biopsies, cycle-day-specific hormone assays, and fertility treatment protocols.
Follicular/Proliferative phase (days 1–14 in a 28-day cycle):
Menstruation (days 1–5) represents shedding of the functional endometrial layer as progesterone and oestrogen withdraw after corpus luteum regression. Rising FSH from the pituitary recruits a cohort of antral follicles; the dominant follicle then drives rising oestradiol. Under oestradiol's influence, the endometrium proliferates — glands become elongated and slightly tortuous, stroma becomes cellular, and the epithelium thickens from ~2–4 mm (post-menstrual) to ~8–10 mm by late follicular phase. Cervical mucus becomes thin, watery, and acellular (characteristic 'Spinnbarkeit' or stretchable mucus up to 10–15 cm), facilitating sperm passage. A positive-feedback peak of oestradiol triggers the mid-cycle LH surge, causing ovulation.
Ovulation (day 14 in a 28-day cycle, but variable):
The dominant follicle ruptures; the secondary oocyte is released and swept by the fimbriae into the fallopian tube. Basal body temperature rises by 0.2–0.5°C after ovulation and remains elevated throughout the luteal phase — a retrospective marker of ovulation. LH detection in urine (using ovulation prediction kits) is the prospective marker, rising 12–24 hours before ovulation.
Luteal/Secretory phase (days 15–28 in a 28-day cycle):
The corpus luteum secretes progesterone (and some oestradiol), which transforms the endometrium from a proliferative to a secretory pattern — glands become coiled and tortuous with serrated lumens, glycogen-rich secretions accumulate, and the stroma becomes oedematous and then decidualised. This creates the implantation window (approximately cycle days 20–24), during which the endometrium is maximally receptive. The cervical mucus becomes thick and viscid under progesterone, forming a 'mucous plug' that prevents further sperm penetration. The luteal phase is remarkably constant at approximately 14 days (range 12–16 days) regardless of overall cycle length — it is the follicular phase that varies, making the luteal phase duration the 'fixed' phase.