Page 12 of 29
OG5.1-2 | Preconception Counselling — SDL Guide
Learning Objectives
- Explain the rationale for preconception counselling and identify women who require it
- Describe the key risks associated with pre-existing medical conditions — diabetes, hypertension, renal disease, SLE, obesity, epilepsy, and cardiac disease — in the context of pregnancy planning
- Identify teratogenic medications requiring pre-conception substitution and state the safe alternatives
- Verify immunisation status and apply the appropriate pre-conception vaccination schedule
- Apply the correct folic acid dosing strategy based on individual risk factors for neural tube defects
- Conduct a structured preconception risk assessment to identify and document maternal high-risk factors
INSTRUCTIONS
Preconception care is the most upstream intervention in maternal health — optimising a woman's health before conception reduces maternal mortality, congenital anomalies, and adverse pregnancy outcomes more effectively than any intrapartum intervention. This module equips you to conduct a systematic preconception consultation, recognise high-risk conditions, modify teratogenic drug regimens, and verify immunisation status before pregnancy begins.
References
- Dutta DC. Textbook of Obstetrics, 10th ed., New Central Book Agency, 2021. Ch 5 (textbook)
- NICE Guideline NG201: Epilepsy in adults, 2022. Section on valproate in women of childbearing potential (guideline)
- FOGSI Good Clinical Practice Recommendations on Preconception Care, 2020 (guideline)
- Cunningham FG et al. Williams Obstetrics, 26th ed., McGraw-Hill, 2022. Ch 8 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Priya, a 28-year-old woman with epilepsy, comes to the antenatal clinic at 8 weeks of pregnancy. Her neurologist had started her on sodium valproate two years ago for well-controlled idiopathic generalised epilepsy. She did not tell her doctor she was trying to conceive. The obstetrician reviews her medications and explains, with difficulty, that valproate carries a 10% risk of major congenital malformations and a 30–40% risk of developmental problems in the child — risks that could have been substantially reduced if she had sought preconception advice, been switched to a safer anticonvulsant, and taken high-dose folic acid before conceiving. This scenario plays out across multiple conditions — diabetes, hypertension, SLE, heart disease — every week in every major hospital. The consultation that prevents it is called preconception counselling, and you are about to learn exactly how to conduct it.
WHY THIS MATTERS
More than 50% of pregnancies globally are unplanned, yet many medical conditions and medications that cause the greatest harm to the developing embryo exert their teratogenic effect during organogenesis — weeks 3–8 of embryonic development — before most women even know they are pregnant. Preconception counselling, when delivered to women with medical conditions who are planning pregnancy, can prevent congenital anomalies, reduce maternal mortality (particularly in high-risk cardiac disease, SLE, and renal disease), and optimise pregnancy outcomes at negligible cost. As a clinician, you will encounter women with these conditions in every specialty, and the ability to counsel them about pregnancy risk is an expected competency from the first year of practice.
RECALL
From your pharmacology and physiology courses, recall three foundational concepts. First, organogenesis — the formation of the major organ systems — occurs between weeks 3 and 8 of embryonic development (weeks 5–10 of the last menstrual period). Teratogenic exposure during this window causes structural malformations; exposure after organogenesis may cause growth restriction or functional deficits but rarely structural anomalies. Second, the placenta is not a perfect barrier — lipophilic, small-molecular-weight drugs cross freely, and some drugs are actively transported to the fetus. Third, folic acid is required for neural tube closure, which is complete by day 28 post-fertilisation — before most women know they are pregnant. These principles justify the logic of all preconception interventions: act before conception to protect the embryo during the window when it is most vulnerable and least visible.
Clinical Indication: Who Needs Preconception Counselling and Why
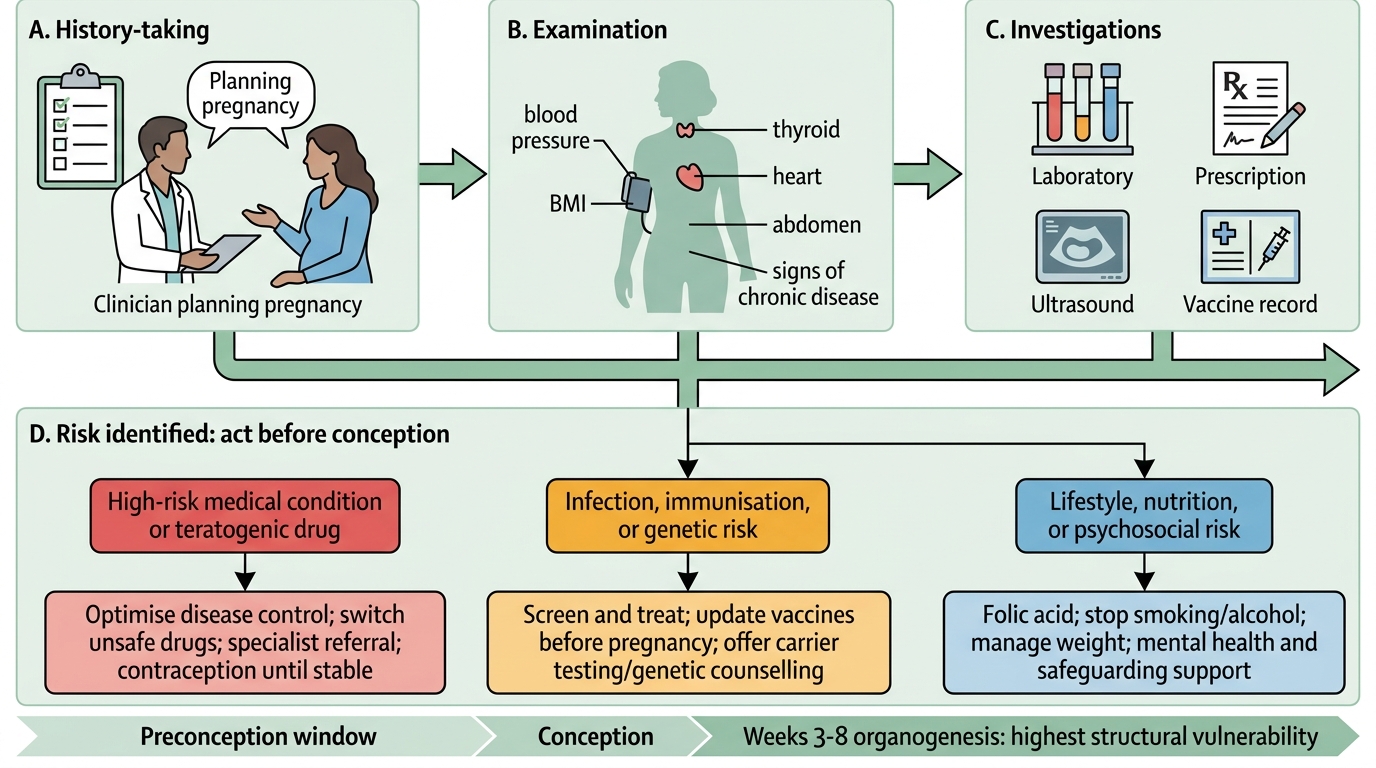
Preconception counselling is a structured, proactive clinical consultation offered to women (and ideally their partners) before a planned pregnancy, with the goal of identifying and modifying risk factors that could harm the mother or the developing embryo. It is not a single visit but a process — ideally beginning 3–6 months before the planned conception, allowing time for medication switches to take effect, for vaccination-induced immunity to develop, and for lifestyle changes such as weight optimisation to be meaningful. The distinction between preconception care and antenatal care is temporal and consequential: antenatal care begins after conception, by which time the critical window of organogenesis (weeks 3–8 of embryonic life) may already be partly or fully over. Structural cardiac malformations, neural tube defects, and limb anomalies can be caused by teratogenic drug exposure in the first 6–8 weeks of embryonic life — a window during which many women have not yet had a positive pregnancy test, let alone attended a clinic. Preconception counselling is therefore the only intervention that can prevent this category of harm. It converts 'reactive' antenatal damage limitation into proactive prevention.
Every woman of reproductive age deserves brief preconception advice as part of routine care. However, the following groups warrant a dedicated, detailed preconception consultation:
- Women with pre-existing medical disorders — diabetes, hypertension, renal disease, SLE, epilepsy, cardiac disease, thyroid disease, coeliac disease, thrombophilias, and mental health conditions
- Women on potentially teratogenic medications — anticonvulsants (especially valproate), isotretinoin, methotrexate, mycophenolate, ACE inhibitors, angiotensin receptor blockers, warfarin, lithium, thalidomide-analogues, some chemotherapy agents
- Women with previous adverse pregnancy outcomes — recurrent miscarriage, stillbirth, neonatal death, fetal anomaly, severe pre-eclampsia, gestational diabetes
- Women with a family history of hereditary conditions — chromosomal disorders, single-gene disorders, consanguinity
- Women with nutritional deficiencies or extreme BMI
- Adolescents planning or at risk of pregnancy
In India, given the high prevalence of anaemia, hypothyroidism, type 2 diabetes, and rheumatic heart disease in women of reproductive age, preconception counselling has particular public health significance. The FOGSI Good Clinical Practice Recommendations emphasise integration of preconception care into routine gynaecology consultations rather than as a separate specialist service.
Preconception Risk Assessment Pathway
Governing Principles of Preconception Risk Assessment
Effective preconception counselling rests on a small number of governing principles that provide the logical framework for every decision made in the consultation. Understanding these principles allows you to reason from first principles when you encounter a drug or condition not covered by a specific guideline.
Principle 1 — The window of vulnerability: The embryo is most vulnerable to structural teratogenic harm during organogenesis (weeks 3–8 of embryonic life). By the time most women present to antenatal care at 8–10 weeks, organogenesis is complete or nearly so. Interventions must therefore be in place BEFORE conception — not at first antenatal booking. This is the single most important argument for preconception care.
Principle 2 — Teratogenicity is dose-, timing- and agent-specific: Not all drugs that cross the placenta are teratogenic, and not all teratogens are equally harmful. Valproate causes a ~10% rate of major congenital malformations at therapeutic doses; lamotrigine at therapeutic doses has a much lower rate (~2–3% in registry data). The risk is also timing-dependent: ACE inhibitors are harmful in the second and third trimesters (causing renal dysplasia and oligohydramnios) but the first-trimester risk is less certain. Knowing the specific risk of each drug — not just 'avoid drugs in pregnancy' — is what enables safe prescribing decisions.
Principle 3 — Disease stability matters as much as drug choice: Poorly controlled epilepsy poses a direct risk from maternal seizures (hypoxia, falls, trauma) that may outweigh a moderate teratogenic risk from a necessary anticonvulsant. Poorly controlled SLE in the 6 months before conception predicts worse pregnancy outcomes regardless of drug choice. The goal is not to stop all medication but to achieve the best possible disease control with the safest available drugs.
Principle 4 — Risk stratification guides the intensity of counselling: A healthy 28-year-old with a well-controlled single-drug epilepsy on lamotrigine needs different advice from a 35-year-old with lupus nephritis, uncontrolled hypertension, and a creatinine of 200 μmol/L. Risk stratification tools — the WHO maternal cardiac risk classification, CKD staging, SLE activity scores, HbA1c — provide objective anchors for risk communication.
Medical Disorders and Their Preconception Management
Each of the medical conditions that commonly co-exist with reproductive-age women has a specific risk profile in pregnancy and a set of targeted pre-conception interventions. The ability to recall the key risk and the key intervention for each condition — rapidly and accurately — is tested in both written examinations and clinical practice. The following sections present the six most important conditions you will encounter, organised by the type of harm they pose and the action required before conception. For each condition, there is a primary maternal risk (what happens to the woman), a primary fetal or neonatal risk (what happens to the baby), and a lead pre-conception intervention that reduces that risk most effectively. The framework for each condition is: identify the risk level → modify the modifiable risk factors → stabilise the disease → review medications → prescribe appropriate nutritional supplements → time the pregnancy to a window of maximal safety. Learning this framework for each condition, rather than isolated facts, builds the clinical reasoning pattern that serves you across a career.
Provided image
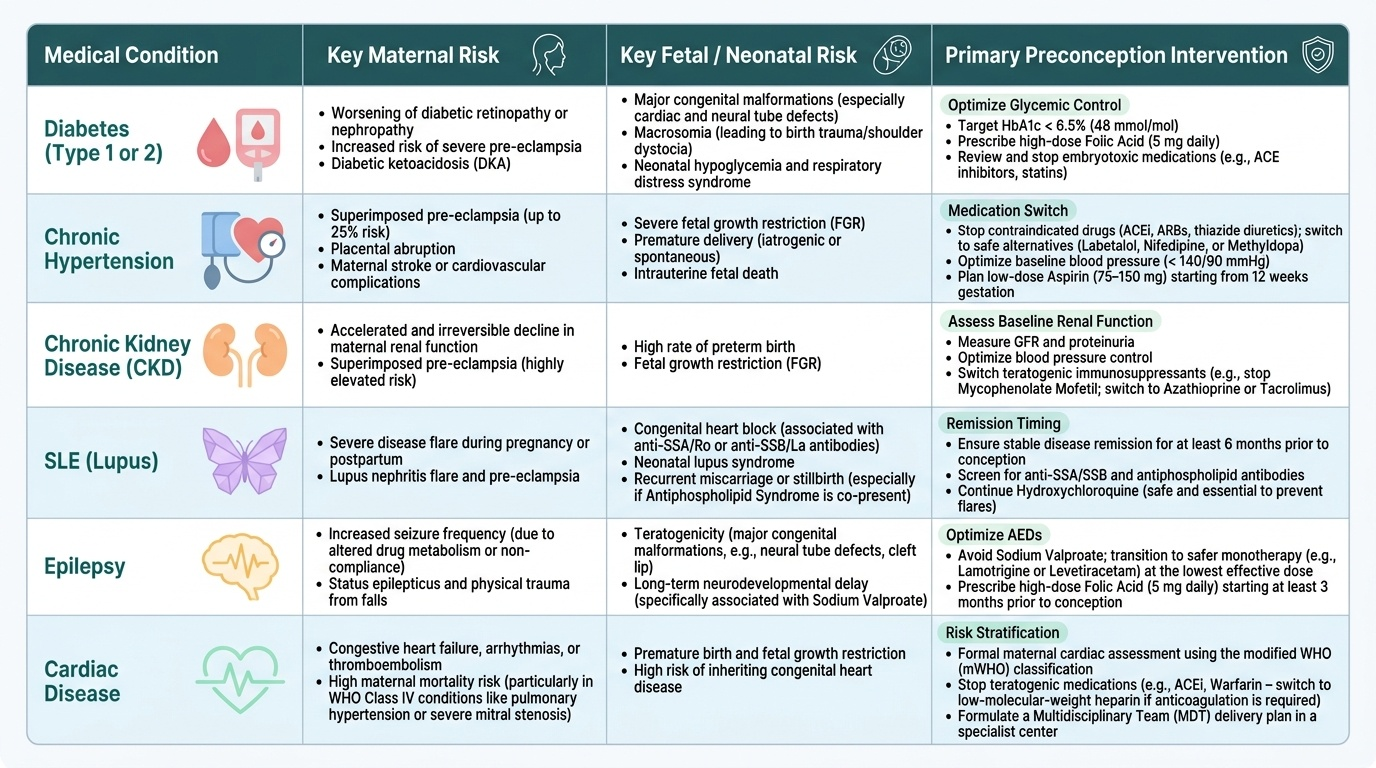
Diabetes (Type 1 or Type 2): Pre-existing diabetes carries a significantly elevated risk of congenital malformations (especially cardiac and neural tube defects), pre-eclampsia, macrosomia, and stillbirth. The single most modifiable risk factor is HbA1c. Pre-conception HbA1c targets should be ≤48 mmol/mol (≤6.5%) if achievable without unacceptable hypoglycaemia; if HbA1c is >86 mmol/mol (>10%), the risk of congenital anomaly is substantially elevated and the woman should be advised to defer pregnancy until better control is achieved. All women with pre-existing diabetes need 5 mg folic acid daily (high-dose) from at least one month before conception. Metformin can continue in pregnancy; oral hypoglycaemics other than metformin are generally replaced with insulin under specialist guidance.
Hypertension: Essential hypertension requires medication review — ACE inhibitors and angiotensin receptor blockers (ARBs) must be switched before conception (fetotoxic in second and third trimesters: oligohydramnios, renal dysplasia, intrauterine growth restriction). Safe antihypertensives in pregnancy include methyldopa, labetalol, and oral nifedipine. A baseline 24-hour urine protein and renal function establish whether hypertension has a secondary renal cause, which alters the pregnancy risk category.
Renal disorders (CKD): CKD increases the risk of pre-eclampsia, preterm birth, and intrauterine growth restriction in proportion to the degree of renal impairment. Women with eGFR <30 mL/min/1.73m² should receive detailed specialist counselling about the risks of further permanent renal function decline with pregnancy. Women with eGFR <15 or on dialysis should generally be advised to defer pregnancy until after successful renal transplantation. Proteinuria >1 g/day at baseline significantly worsens prognosis.
SLE: Disease activity in the 6 months before conception is the strongest predictor of pregnancy outcomes in SLE. Active lupus nephritis at conception substantially increases the risk of pre-eclampsia, preterm birth, intrauterine fetal death, and permanent renal impairment. Ideally, SLE should be in remission (SLEDAI score ≤4) for at least 6 months before conception. Hydroxychloroquine (compatible with pregnancy) should be continued or started before conception; it reduces lupus flares and is associated with better neonatal outcomes. Mycophenolate mofetil and methotrexate — commonly used in SLE — are teratogenic and must be discontinued and substituted (e.g. azathioprine, which is compatible with pregnancy) at least 3–6 months before conception.
Obesity (BMI >30 kg/m²): Obesity independently increases the risk of gestational diabetes, pre-eclampsia, venous thromboembolism, macrosomia, shoulder dystocia, caesarean delivery, and anaesthetic complications. Women with BMI >30 need 5 mg folic acid daily (high-dose). Pre-conception weight loss is the most effective modifiable intervention — even a 5–10% reduction in body weight significantly reduces the risk of gestational diabetes. Bariatric surgery, if required, should be completed and weight should be stable for at least 12–18 months before attempting conception.
Epilepsy: This is the highest-stakes preconception medication issue in routine gynaecology practice. Sodium valproate carries the highest teratogenic risk of all anticonvulsants — approximately 10% major congenital malformations (cardiac, neural tube, facial clefts, limb abnormalities) and 30–40% risk of neurodevelopmental problems (autism spectrum disorder, intellectual disability). Women on valproate who plan pregnancy must be reviewed by a neurologist well before conception; where clinically safe, valproate should be switched to lamotrigine or levetiracetam (lower teratogenic risk). If valproate cannot be safely withdrawn, high-dose folic acid (5 mg/day) should be prescribed and the patient counselled fully using the SABRE programme. ALL women with epilepsy need high-dose folic acid (5 mg/day) pre-conception.
Heart disease: Maternal cardiac disease accounts for the largest proportion of direct maternal deaths in many developed countries, and congenital heart disease is increasingly prevalent as more women with repaired congenital lesions reach reproductive age. Risk stratification uses the WHO Maternal Cardiovascular Risk Classification (I–IV). Class III conditions (e.g. mechanical heart valves, systemic right ventricle) carry significant risk (15–30% maternal morbidity/mortality) and require intensive counselling and specialist co-management. Class IV conditions — including Eisenmenger's syndrome, severe pulmonary hypertension (pulmonary arterial hypertension), severe left ventricular dysfunction (EF <30%), and severe mitral/aortic stenosis — carry a maternal mortality risk >25% and are absolute contraindications to pregnancy. These women must be counselled clearly that pregnancy is not safe, and permanent contraception discussed.
SELF-CHECK
A 26-year-old woman with idiopathic generalised epilepsy is controlled on sodium valproate 1000 mg/day. She presents asking about pregnancy planning. What is the most important initial action?
A. Advise her to stop valproate immediately and use no anticonvulsant during pregnancy
B. Refer to neurology for medication review with a view to switching to a lower-risk anticonvulsant before conception, and prescribe high-dose folic acid 5 mg/day immediately
C. Reassure her that modern antiepileptics are safe in pregnancy and that no change is needed
D. Advise her to wait until she is pregnant before changing her anticonvulsant to avoid seizure risk
Reveal Answer
Answer: B. Refer to neurology for medication review with a view to switching to a lower-risk anticonvulsant before conception, and prescribe high-dose folic acid 5 mg/day immediately
Valproate carries a ~10% risk of major congenital malformations and a 30–40% risk of neurodevelopmental problems. The correct approach is: (1) refer to neurology for medication review before conception — if clinically safe, switch to lamotrigine or levetiracetam; (2) prescribe folic acid 5 mg/day immediately (high-dose for all women with epilepsy). Stopping without review risks breakthrough seizures; waiting until pregnant means organogenesis has already occurred on valproate.