Page 13 of 29
OG5.1-2 | Preconception Counselling — SDL Guide (Part 2)
Medication Review, Immunisation and Nutritional Optimisation
Beyond the condition-specific issues above, every preconception consultation must address medication safety, immunisation status, and nutritional optimisation — three areas where targeted intervention can prevent serious harm at minimal cost. These are not optional add-ons to the consultation; they represent the operational core of preconception care, applicable to virtually every woman who presents regardless of whether she has a specific medical condition. A woman who appears medically uncomplicated may be taking an over-the-counter herbal supplement that interacts with early pregnancy, or may be seronegative for rubella despite believing she was vaccinated in childhood (vaccine-derived immunity can wane). The habit of systematically reviewing medications, immunisation records, and nutritional status at every preconception encounter is what makes the consultation genuinely protective rather than merely reassuring.
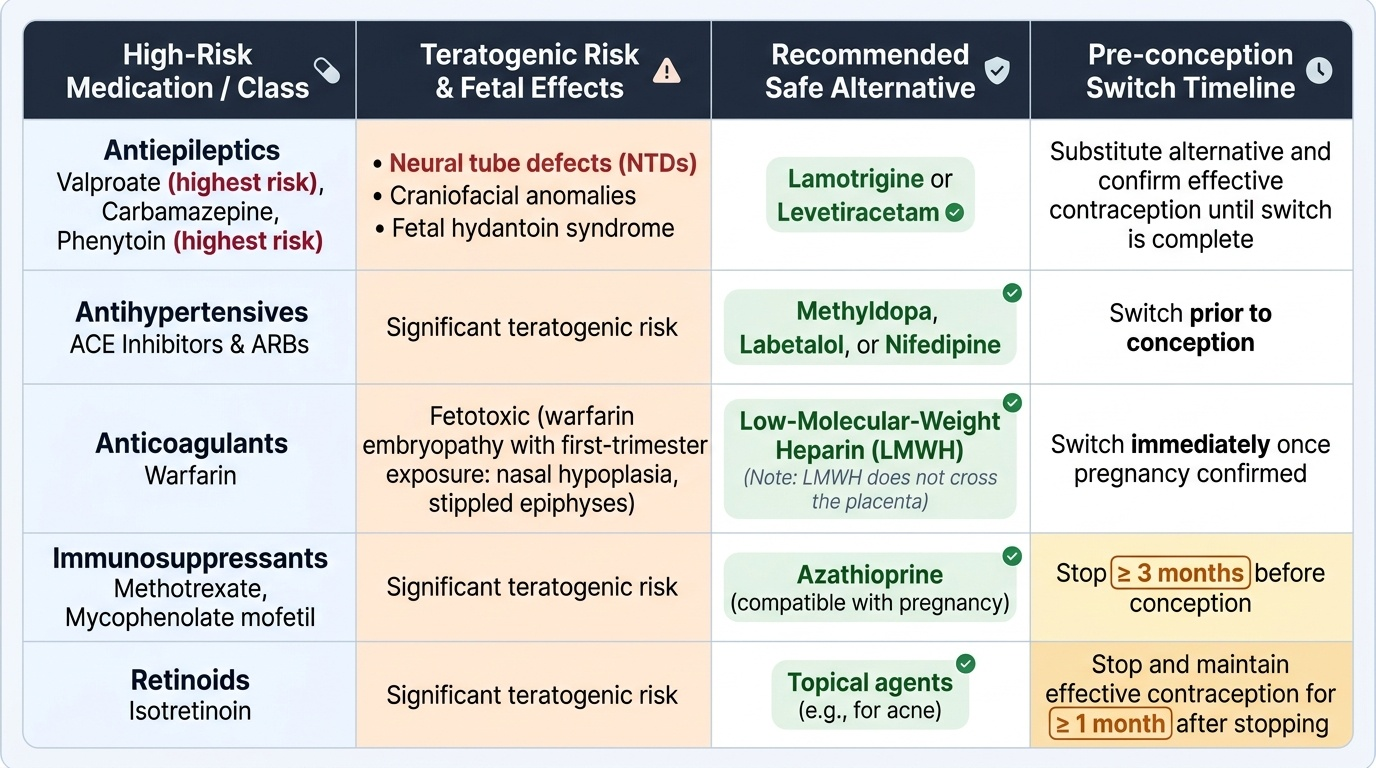
Teratogenic medication review: Several commonly prescribed drugs carry significant teratogenic risk and must be reviewed before conception. The general principle is: identify the drug, confirm the teratogenic mechanism and critical period of risk, substitute a safer alternative while maintaining disease control, and confirm effective contraception until the switch is complete.
Provided image
Key teratogenic drug classes:
- Antiepileptics: valproate (highest risk — switch to lamotrigine/levetiracetam); carbamazepine (NTDs, craniofacial); phenytoin (fetal hydantoin syndrome)
- Antihypertensives: ACE inhibitors and ARBs — switch to methyldopa, labetalol, or nifedipine
- Anticoagulants: warfarin — fetotoxic (warfarin embryopathy with first-trimester exposure: nasal hypoplasia, stippled epiphyses); switch to low-molecular-weight heparin (LMWH) once pregnancy confirmed; note: LMWH does NOT cross the placenta
- Immunosuppressants: methotrexate and mycophenolate mofetil — stop ≥3 months before conception; switch to azathioprine (compatible with pregnancy)
- Retinoids: isotretinoin (acne) — must be stopped and effective contraception maintained for ≥1 month after stopping; acne may be managed with topical agents
- Lithium: associated with Ebstein's anomaly (tricuspid valve) at very high doses — risk lower than historically stated but warrants specialist review; gradual switch to alternative mood stabiliser if feasible
Immunisation: The preconception visit is the ideal time to review vaccination status and complete any outstanding immunisations, because several vaccines cannot be given during pregnancy.
| Vaccine | Type | Pre-conception action | In pregnancy |
|---|---|---|---|
| Rubella (MMR) | Live attenuated | Screen rubella IgG; vaccinate if seronegative; avoid conception for ≥1 month post-vaccination | Contraindicated |
| Varicella | Live attenuated | Screen varicella IgG; vaccinate if seronegative (2 doses); avoid conception ≥1 month | Contraindicated |
| Hepatitis B | Recombinant | Complete 3-dose series if not immune; check anti-HBs titre | Safe |
| Influenza | Inactivated | Vaccinate (annual) | Safe; recommended |
| COVID-19 | mRNA / viral vector | Vaccinate/booster | Safe; recommended |
| Tdap (tetanus, diphtheria, pertussis) | Toxoid/inactivated | Update if >10 years since last dose | Safe in pregnancy (27–36 weeks for pertussis protection of neonate) |
Folic acid and nutritional supplementation:
Folic acid (vitamin B9) is required for neural tube closure, which is complete by day 28 post-fertilisation. Neural tube defects (NTDs — anencephaly, spina bifida) affect approximately 1–2 per 1,000 births without supplementation; periconceptional folic acid reduces the risk by approximately 70%.
- Standard dose: 400 mcg (0.4 mg) per day — for all women without risk factors, starting at least one month before conception and continuing through the first trimester
- High-dose (5 mg/day): for women with: previous NTD-affected pregnancy; diabetes; epilepsy on anticonvulsants (all agents); BMI >30; malabsorption syndromes (coeliac disease, inflammatory bowel disease, bariatric surgery); multiple pregnancy
Additionally: iodine supplementation (150 mcg/day) is recommended for all women planning pregnancy in iodine-deficient regions; iron should be checked and corrected if anaemia is present before conception; vitamin D supplementation is recommended where deficiency is prevalent.
SELF-CHECK
Which of the following vaccines is SAFE to administer during pregnancy?
A. MMR (measles, mumps, rubella) vaccine
B. Varicella (chickenpox) vaccine
C. Inactivated influenza vaccine
D. Yellow fever vaccine
Reveal Answer
Answer: C. Inactivated influenza vaccine
Inactivated influenza vaccine is safe and indeed recommended during pregnancy — pregnant women are at higher risk of severe influenza. Live attenuated vaccines (MMR, varicella, yellow fever) are contraindicated in pregnancy because of theoretical risk of vaccine-strain transmission to the fetus. MMR and varicella should be given pre-conception with at least 1 month of contraception afterwards before attempting conception.
Identifying Maternal High-Risk Factors and Verifying Immunisation Status
In clinical practice, the ability to take a structured, systematic history that efficiently identifies all relevant high-risk factors is what distinguishes a competent preconception consultation from an incomplete one. This is a clinical skill, not merely a knowledge task — it requires the discipline to cover seven history domains without omission, the sensitivity to approach domestic violence and social risk screening, and the clinical acumen to translate history findings into an individualised risk profile that drives specific investigations and interventions. A woman can present with multiple overlapping risk factors — for example, type 2 diabetes (HbA1c poorly controlled), BMI 34, previous stillbirth, on enalapril, seronegative for rubella, smoking 10 cigarettes per day — and the preconception consultation must address all of these systematically rather than focusing only on the most visible concern. The following structure provides the framework for a complete preconception risk assessment. Use it as a mental checklist in every consultation until it becomes habitual.
History: The preconception history covers the following domains systematically:
- Obstetric history: Previous pregnancies — outcomes, gestational age, mode of delivery; previous NTDs, congenital anomalies, pre-eclampsia, gestational diabetes, preterm labour, stillbirth, recurrent miscarriage (≥3 consecutive losses suggests investigation for antiphospholipid syndrome, parental chromosome anomalies)
- Medical history: Known medical conditions (using the domains above — DM, HTN, renal, SLE, epilepsy, cardiac, thyroid, coeliac, thrombophilia); duration of illness; degree of control; recent specialist review
- Surgical history: Previous uterine surgery (myomectomy, caesarean section, cone biopsy — assess uterine scar, cervical competence)
- Medication history: ALL current medications, including over-the-counter and herbal preparations — classify each as safe, requires monitoring, or requires substitution; note dose and duration
- Family history: Hereditary conditions (autosomal dominant, recessive, X-linked); consanguinity (first-cousin marriage increases risk of autosomal recessive conditions 2–3× baseline); Down syndrome, chromosomal anomalies in first-degree relatives
- Social history: Smoking (cessation reduces miscarriage, IUGR, placenta praevia risk); alcohol (no known safe level — advise abstinence from conception onwards); recreational drug use; occupational exposures (teratogens, radiation, chemicals); domestic violence screen
- Nutritional history: Dietary habits, vegetarian/vegan diet (B12 and iron risk), known eating disorders, recent bariatric surgery
Examination: BMI (weight + height), blood pressure, examination for signs of poorly controlled systemic disease (e.g. SLE rash, diabetic retinopathy screen, cardiac auscultation)
Investigations (baseline and targeted):
- All women: FBC (anaemia), blood group and antibody screen, rubella IgG, varicella IgG, hepatitis B surface antigen, HIV serology, TSH, haemoglobin electrophoresis (sickle cell / thalassaemia carrier screen — mandatory in high-prevalence populations)
- Diabetes: HbA1c, renal function, urine ACR (albuminuria), ophthalmology review (retinopathy may worsen in pregnancy)
- Hypertension: Renal function, urine protein/creatinine ratio, ECG, 24-hour ABPM if indicated
- Epilepsy: Serum anticonvulsant levels; neurological review; EEG if recent change in seizure pattern
- Cardiac disease: Echocardiogram, WHO risk classification, cardiology review; exercise tolerance test if valvular disease
- SLE: SLEDAI score, complement levels (C3/C4), anti-dsDNA antibodies, antiphospholipid antibodies (anticardiolipin, anti-β2-GPI, lupus anticoagulant), renal function
SELF-CHECK
A 30-year-old woman presents for preconception counselling. She has a history of two consecutive first-trimester miscarriages. Her BMI is 29. She is not on any regular medications. Which investigation is MOST important to add to the routine preconception screen?
A. Karyotype of the couple and antiphospholipid antibody screen
B. Full cardiac echo and WHO risk classification
C. HbA1c and fasting glucose
D. Thyroid function tests and TSH receptor antibodies
Reveal Answer
Answer: A. Karyotype of the couple and antiphospholipid antibody screen
Two (or three) consecutive miscarriages warrant investigation for recurrent pregnancy loss. The two most important treatable causes to exclude are: (1) antiphospholipid syndrome (anticardiolipin, anti-β2-GPI, lupus anticoagulant), which is associated with recurrent first and second trimester loss and thrombosis; and (2) parental chromosomal anomalies (balanced translocations), detectable on karyotype. Cardiac echo and WHO classification apply to pre-existing cardiac disease, which is not suggested here.
Applied Practice: Running a Preconception Consultation
Preconception counselling is most effectively learned through structured worked cases — scenarios where you apply the framework above to a real patient situation and then receive feedback on your decision-making. The two cases below represent the highest-stakes presentations you will encounter as a final-year student and junior doctor, and they are chosen because they are commonly examined, commonly mismanaged, and commonly preventable. Working through them in detail — not just reading the answers but reasoning through each decision point — is the level of engagement required for this type of clinical reasoning to be genuinely internalised. As you read each case, try to formulate your own management plan before reading the annotated approach: what is the risk level, what medications need to change, what dose of folic acid, when should she conceive, and what enhanced antenatal monitoring will she need once pregnant? These are the exact questions the examiner will ask, and the exact decisions a junior doctor will face in a general medical or obstetric clinic.
Provided image
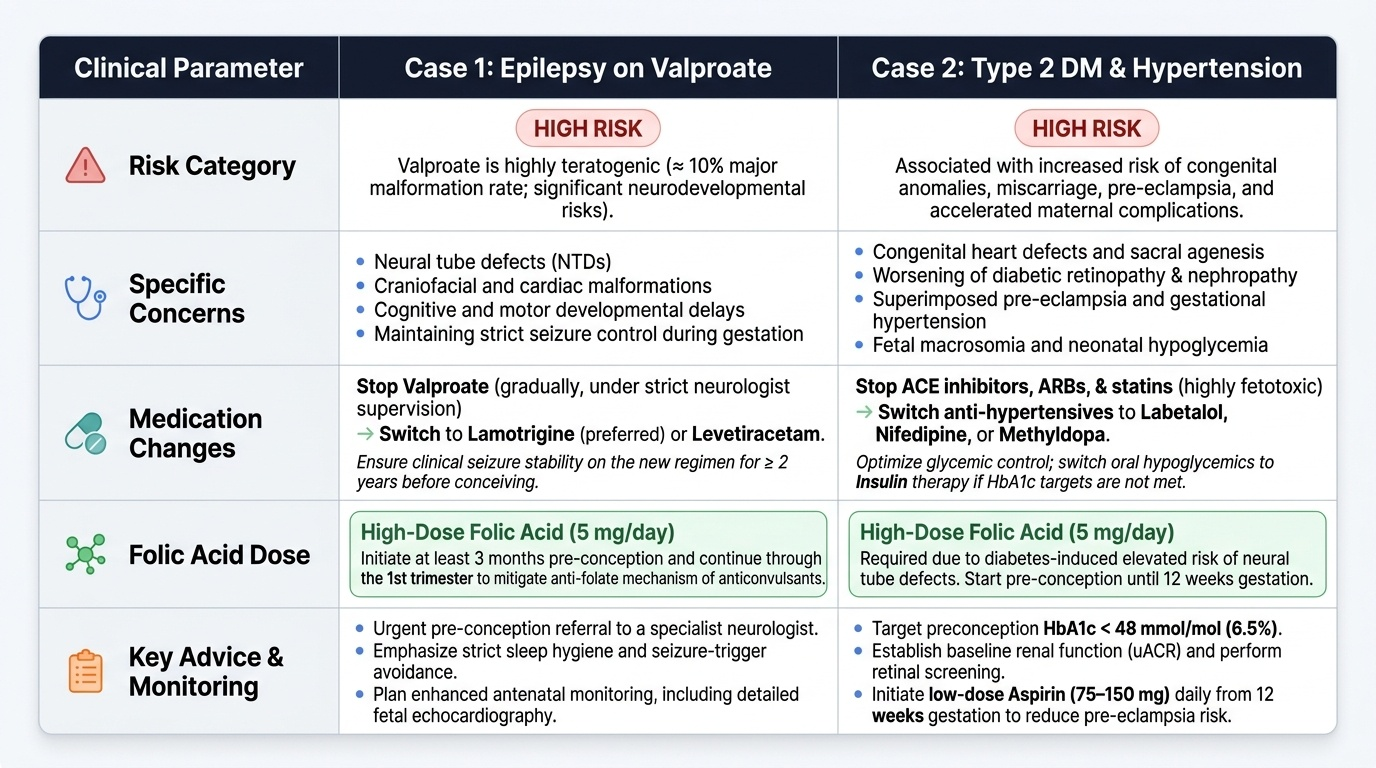
Case 1 — Epilepsy on valproate (from the opening scenario):
Pregnant patient on valproate = emergency management. But if seen pre-conception:
- Risk level: HIGH (valproate = highest-risk anticonvulsant; ~10% major malformation rate)
- Referral: neurologist urgently for medication review; switch to lamotrigine (preferred) or levetiracetam if seizures have been well controlled ≥2 years and the EEG/clinical picture permits
- Folic acid: 5 mg/day immediately
- Effective contraception during the transition period (anticonvulsant switch needs 3–6 months stabilisation before conception)
- Counsel: even on the safest anticonvulsant, epilepsy carries a small increased risk of congenital anomalies (~3%); seizures in pregnancy pose a direct risk to the mother and fetus
- Offer enhanced anomaly scanning (detailed 20-week anatomy scan) once pregnant
Case 2 — Type 2 DM + hypertension:
A 33-year-old woman with 7-year history of type 2 DM on metformin + lisinopril + amlodipine. BMI 34 kg/m². HbA1c 68 mmol/mol. BP 138/88 on medication.
- Risk level: HIGH (sub-optimal glycaemic control, teratogenic antihypertensive, obesity)
- Actions:
1. Stop lisinopril (ACE inhibitor) — switch to methyldopa or labetalol (or nifedipine as second agent); confirm renal function baseline
2. Optimise glycaemic control — target HbA1c ≤48 mmol/mol before conception; specialist endocrinology review; consider insulin if HbA1c not achievable on metformin alone
3. Folic acid 5 mg/day — high-dose (both diabetes and BMI >30 warrant this)
4. Weight management counselling — even 10% weight loss will significantly improve glycaemic control and reduce pre-eclampsia risk
5. Timing — advise deferring conception until HbA1c ≤48 mmol/mol and BP controlled on pregnancy-compatible medications
6. Screen for end-organ damage — diabetic retinopathy (baseline ophthalmic review), renal function, urine ACR
- Counsel: if HbA1c >86 mmol/mol, the major malformation risk is substantially elevated and pregnancy should be deferred; if she conceives with current HbA1c, offer detailed anatomy scan at 18–20 weeks and fetal echocardiogram (cardiac malformations 5× increased in poorly controlled DM)
CLINICAL PEARL
Folic acid dosing: standard 400 mcg vs high-dose 5 mg — know the indications for high-dose. Standard 400 mcg/day is for healthy women with no risk factors. High-dose 5 mg/day is for: previous NTD-affected pregnancy, diabetes (Type 1 or 2), all epilepsy (regardless of which anticonvulsant), BMI >30, malabsorption syndromes, multiple pregnancy. In India, where the prevalence of undiagnosed type 2 diabetes, overweight, and epilepsy is high in reproductive-age women, a large proportion of women presenting for preconception counselling will qualify for the high dose. When in doubt, prescribe 5 mg — the safety margin is wide and the downside of under-prescribing (an NTD) is irreversible.