Page 15 of 30
OG8.6-7 | Nutrition and Vaccination in Pregnancy — SDL Guide
Learning Objectives
- Assess and counsel a patient in a simulated environment regarding appropriate nutrition in pregnancy (OG8.6)
- Enumerate the indications for and types of vaccination in pregnancy (OG8.7)
- Prescribe correct micronutrient supplementation doses including IFA (60 mg elemental iron + 500 µg folic acid × 180 days) and calcium (1 g/day)
- State the Tetanus Toxoid/Td vaccination schedule and identify vaccines contraindicated in pregnancy
INSTRUCTIONS
India carries one of the world's highest burdens of maternal anaemia — nearly one in two pregnant women is anaemic (NFHS-5). At the same time, neonatal tetanus, though substantially reduced, remains a preventable cause of neonatal death in under-immunised communities. As a final-year student you will counsel pregnant women at every ANC contact about diet, supplements, and vaccinations. This module builds the skills to do that accurately and empathetically — using correct doses, correct schedules, and sound communication technique.
References
- DC Dutta's Textbook of Obstetrics, 10th ed., Ch. 5 (Antenatal Care) (textbook)
- Williams Obstetrics, 26th ed., Ch. 9 (Prenatal Care) (textbook)
- NHM India — Operational Guidelines on Maternal Nutrition 2018 (guideline)
- Ministry of Health & Family Welfare — Immunisation Schedule, National Immunisation Programme 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old primigravida at 16 weeks presents for her second ANC visit at a PHC. Her haemoglobin is 9.2 g/dL. She reports she cannot afford to eat meat and eats mainly rice and dal. Her husband asks whether the 'iron tablets make her sick' and whether they can stop them. Her vaccination card shows no TT doses recorded. You have 10 minutes to counsel her on diet, supplements, and vaccination. How do you proceed?
WHY THIS MATTERS
Nutritional deficiency and vaccine-preventable illness are two of the most directly modifiable contributors to maternal and perinatal mortality in India. The National Family Health Survey-5 (2019-21) reports that 52.2% of pregnant women in India are anaemic — the highest prevalence among any reproductive age group. Iron-deficiency anaemia in pregnancy increases the risk of preterm birth, low birth weight, postpartum haemorrhage, and maternal death. Folate deficiency in the periconceptional period is the leading preventable cause of neural tube defects. Meanwhile, neonatal tetanus, once responsible for hundreds of thousands of deaths annually in South Asia, has been dramatically curtailed by routine Tetanus Toxoid immunisation during pregnancy — yet coverage remains incomplete in rural and tribal areas. As a clinician at any level of care, your ability to counsel accurately on these two domains at every ANC contact directly prevents morbidity and mortality. This is not background knowledge — it is a clinical skill that the NMC expects you to demonstrate in a simulated environment (OG8.6, SH level) and to articulate in examinations (OG8.7, KH level).
RECALL
Before proceeding, recall the following from earlier modules: (1) The normal physiology of pregnancy — maternal plasma volume rises ~45% by 34 weeks, red cell mass rises ~20%, creating a dilutional 'physiological anaemia'; iron demand triples in the second and third trimesters. (2) Fetal neural tube closure occurs between days 22–28 of gestation — before most women know they are pregnant — making periconceptional folic acid supplementation the critical window. (3) The standard antenatal care framework from og3-anc-objectives includes at minimum 8 contacts (WHO 2016); nutrition and vaccination counselling is built into each contact. (4) From OG2: placental transfer of iron, calcium, and folate is an active transport process; maternal deficiency directly depletes fetal stores.
Clinical Indication and Relevance
The epidemiological argument for systematic nutritional counselling in pregnancy is compelling. Anaemia in pregnancy is defined as haemoglobin below 11 g/dL in the first and third trimesters and below 10.5 g/dL in the second trimester (WHO). In India, iron-deficiency anaemia accounts for approximately 50% of maternal deaths attributable to anaemia directly, and substantially worsens outcomes in haemorrhage, infection, and cardiac decompensation. The NFHS-5 figure of 52.2% maternal anaemia prevalence means that more than half of pregnant women a clinician encounters in India are anaemic.
Neural tube defects (NTDs) — anencephaly and spina bifida — affect approximately 2.0–2.9 per 1,000 live births in India. The absolute risk is substantially reducible by periconceptional folic acid supplementation, which is why NHM provides free IFA tablets and why supplementation should begin ideally three months before conception and continue through the first trimester at minimum.
On the vaccine front, neonatal tetanus (caused by Clostridium tetani spores entering through the umbilical cord after unhygienic delivery) can be entirely prevented by adequate maternal immunisation, which confers passive immunity to the neonate via transplacental IgG. India's Tetanus-Diphtheria (Td) toxoid programme for pregnant women is a cornerstone of the National Immunisation Programme. Additional vaccines increasingly recommended include inactivated influenza (particularly relevant in flu season and for women with comorbidities) and COVID-19 vaccines, both of which are safe in all trimesters.
The clinical indication for nutritional counselling is universal — every pregnant woman benefits. The clinical indication for vaccination is specific to the woman's immunisation history, gestational age, and endemic disease risk. Both require structured communication skills.
Provided image
Anatomy and Governing Principles of Nutritional Physiology in Pregnancy
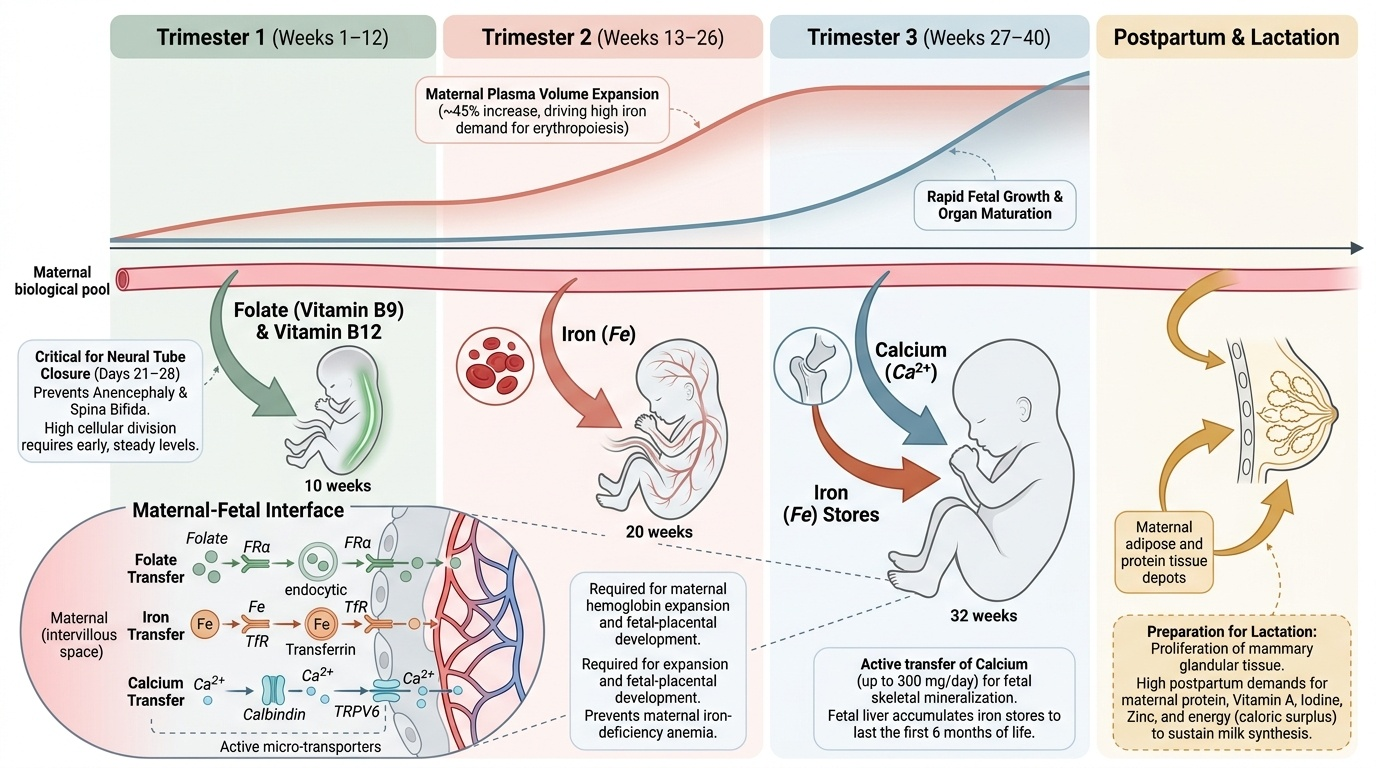
Understanding why nutritional demands escalate in pregnancy requires understanding the physiological changes that occur across three trimesters. The governing principle is straightforward: a woman is now supporting two organisms — her own expanded physiology and a growing fetus — with a single alimentary tract.
Iron requirements increase dramatically: a non-pregnant woman requires approximately 1–2 mg absorbed iron per day; in the second and third trimesters this rises to 6–7 mg/day, far exceeding what most Indian diets can provide bioavailably. The main drivers are the expansion of maternal red cell mass (requiring ~500 mg elemental iron), fetal and placental iron deposition (~300 mg), and expected blood loss at delivery (~200 mg). Total additional iron requirement across pregnancy is approximately 1,000 mg — impossible to source from diet alone in a resource-limited setting, which is why supplementation is mandatory rather than optional.
Folate (folic acid/vitamin B9) is required for DNA synthesis and cell division. The neural tube closes between days 22–28 post-fertilisation, making the periconceptional window critical. Later in pregnancy, folate supports rapid fetal cell replication, placental development, and prevention of megaloblastic anaemia. Folic acid from dietary sources (leafy green vegetables, legumes) is poorly absorbed; synthetic folic acid in supplements has approximately 70% higher bioavailability.
Calcium is required for fetal skeletal mineralisation, which accelerates sharply from 20 weeks onward. The fetus deposits approximately 200–250 mg of calcium per day in the third trimester. The maternal parathyroid compensates by increasing intestinal absorption, but in women with low dietary calcium intake (as is common in rural India), supplementation is necessary. Adequate calcium supplementation also reduces the risk of pre-eclampsia — a benefit that has led WHO to recommend calcium supplementation (1.5–2 g/day) specifically in populations with low dietary calcium intake.
Iodine deficiency causes cretinism and cognitive impairment in the neonate; the maternal requirement increases from 150 µg/day to 220 µg/day in pregnancy. Use of iodised salt is the primary strategy; in iodine-deficient areas, direct supplementation is recommended.
Vitamin D is required for calcium absorption; deficiency is highly prevalent in India despite abundant sunlight due to skin pigmentation, cultural clothing practices, and indoor work. Requirements increase to 600 IU/day in pregnancy.
SELF-CHECK
A pregnant woman at 24 weeks has haemoglobin of 10.3 g/dL (mild anaemia). She says she has been taking her IFA tablet every day. Which of the following is the MOST important next step?
A. Double her IFA dose to 120 mg elemental iron
B. Assess dietary habits — especially tea/coffee intake with meals — and advise on optimising iron absorption
C. Prescribe injectable iron immediately as oral iron has failed
D. Defer further investigation until the third trimester
Reveal Answer
Answer: B. Assess dietary habits — especially tea/coffee intake with meals — and advise on optimising iron absorption
Tea and coffee contain tannins that markedly inhibit non-haem iron absorption. Before escalating to injectable iron, compliance should be confirmed, and dietary factors optimised (take IFA on empty stomach or with vitamin C-rich foods; avoid tea/coffee within 1 hour of IFA). Injectable iron is reserved for severe anaemia (Hb <7 g/dL), malabsorption, or intolerance, not for mild anaemia in a patient claiming compliance.
Nutritional Assessment and Counselling Technique
A structured nutritional assessment at each ANC contact should be brief, non-judgmental, and culturally sensitive. The key elements are:
Step 1 — Anthropometric Assessment: Weigh the patient at every visit and plot on a weight-gain chart. Calculate or recall pre-pregnancy BMI. Target weight gain by pre-pregnancy BMI (IOM guidelines, adapted for Indian women): underweight (BMI <18.5) → 12.5–18 kg total; normal weight (18.5–24.9) → 11.5–16 kg; overweight (25–29.9) → 7–11.5 kg; obese (≥30) → 5–9 kg. In practice, a weight gain of approximately 1–1.5 kg/month in the second and third trimesters is acceptable as a clinical rule of thumb. Fundal height measurement complements weight gain assessment for fetal growth.
Step 2 — Dietary History: A brief 24-hour dietary recall is the most practical tool in a busy clinic. Ask about: staple grain (rice/wheat/millets), protein source (pulses/legumes/eggs/fish/meat), green leafy vegetables (spinach, methi, drumstick leaves — the most affordable iron and folate sources), dairy (milk/curd — calcium), and fruits. Identify barriers: food insecurity, cultural restrictions (e.g., taboos around egg eating in first trimester), nausea limiting intake, economic constraints.
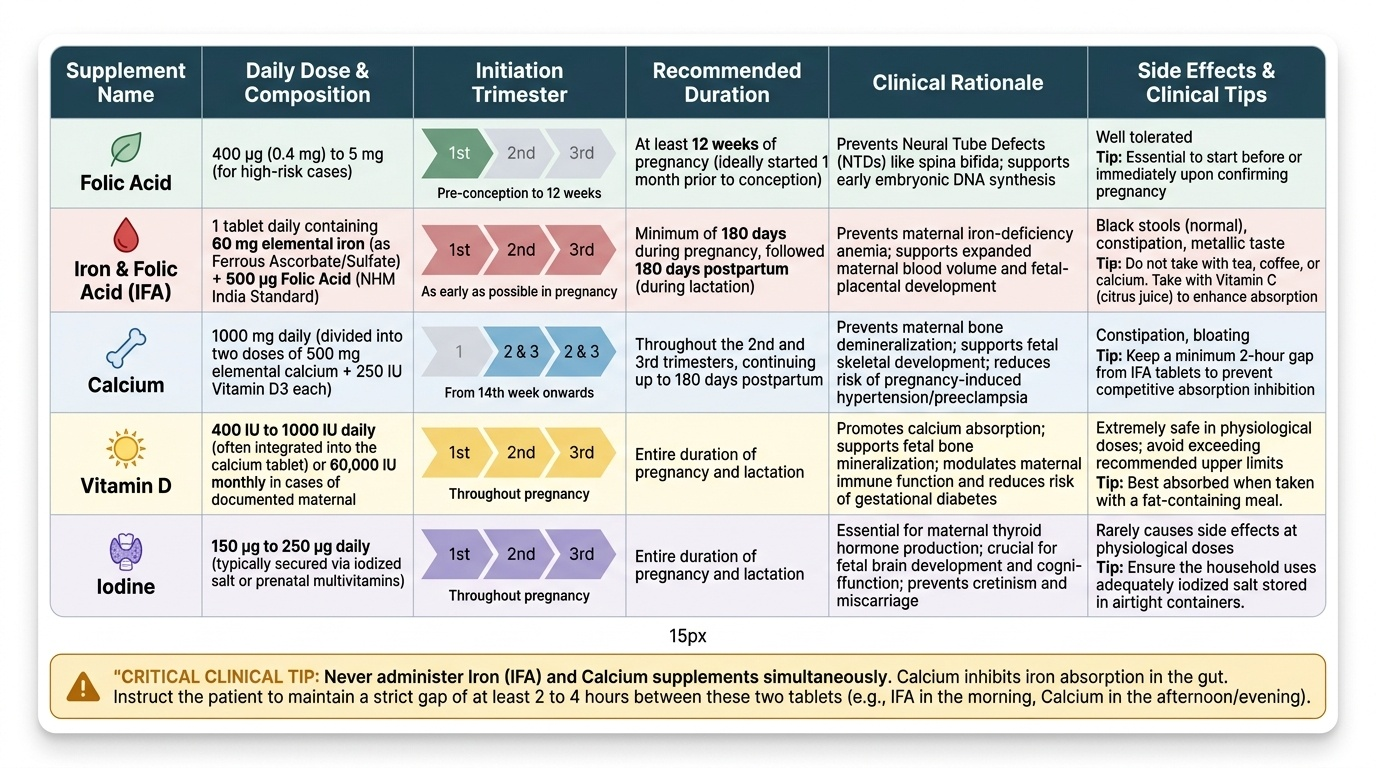
Step 3 — Supplement Prescription: The National Health Mission (NHM) standard supplement regimen for pregnancy in India is:
- IFA (Iron–Folic Acid) tablet — 1 tablet daily containing 60 mg elemental iron + 500 µg (0.5 mg) folic acid, starting as early as possible in pregnancy and continuing for a minimum of 180 days (6 months). This is different from the preconception tablet (0.4 mg folic acid only) — both are available at PHC free of cost.
- Calcium supplement — 1 g elemental calcium per day (typically two 500 mg tablets, one twice daily), starting from the second trimester (approximately 14–20 weeks) through delivery and lactation. This is particularly important in populations with low dietary dairy intake.
- Iodine — ensure iodised salt use. In documented deficiency areas, potassium iodide supplementation is prescribed.
- Vitamin D — 400–600 IU/day is the standard recommendation; in women with clinical deficiency (symptoms, low sun exposure), higher replacement doses may be required under supervision.
Counselling technique: Use OARS (Open questions, Affirming, Reflecting, Summarising) for communication. Specifically: (a) Ask about current diet in a neutral, non-judgmental manner. (b) Affirm what the patient is already doing well — even small positives reinforce behaviour. (c) Explain WHY each supplement is needed (e.g., 'The iron tablet helps prevent anaemia, which makes delivery safer and helps your baby grow'). (d) Counsel on taking IFA on an empty stomach or with a small amount of vitamin C-rich food, and avoiding tea/coffee within one hour. (e) Acknowledge and address side effects (nausea, constipation) — advise taking after food if nausea is a problem, and increasing fluid and fibre for constipation. (f) Summarise clearly: 'One iron tablet and two calcium tablets every day — do not stop them even if you feel well.'
Provided image