Page 16 of 30
OG8.6-7 | Nutrition and Vaccination in Pregnancy — SDL Guide (Part 2)
Vaccination in Pregnancy — Principles, Schedule and Contraindications
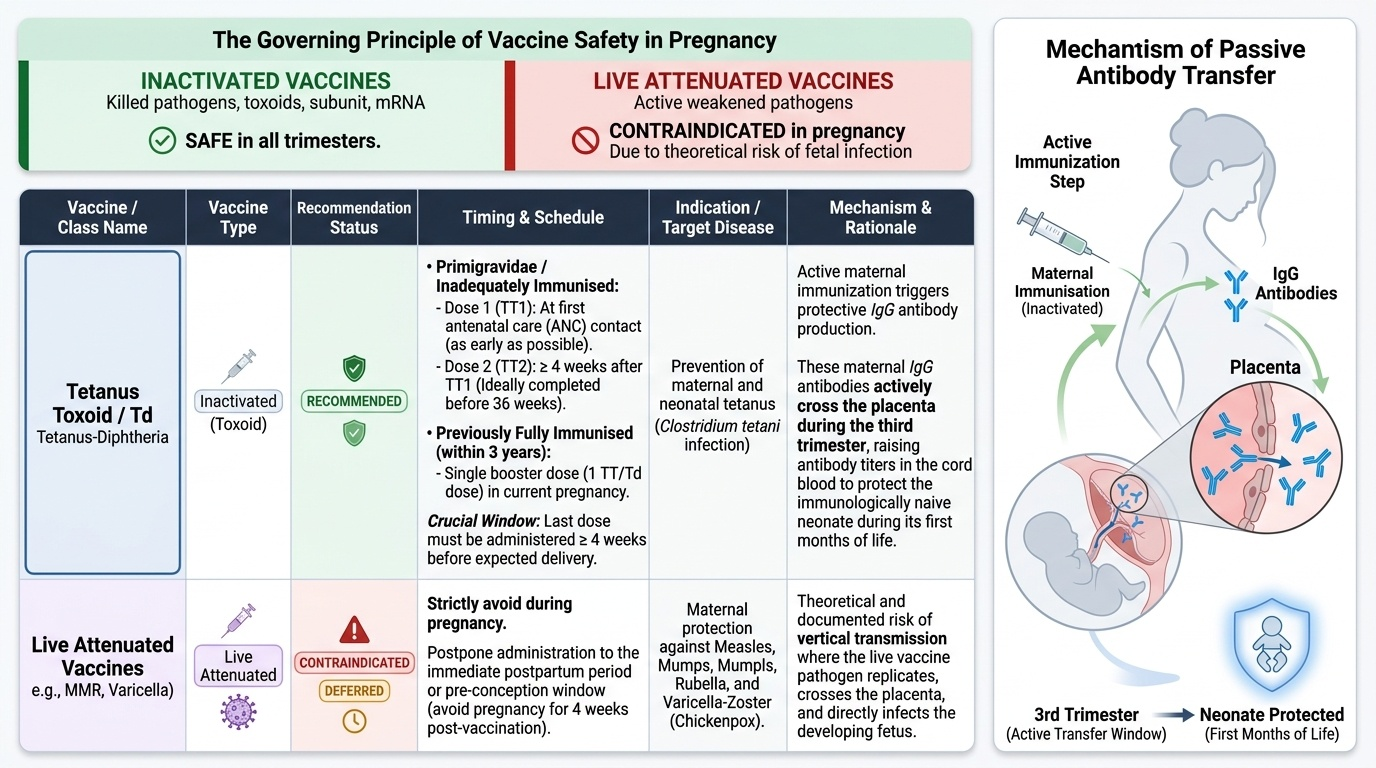
Vaccination in pregnancy is one of the most cost-effective interventions in maternal-neonatal care. It aims to achieve two outcomes simultaneously: protection of the mother from vaccine-preventable illness that carries excess risk in pregnancy, and passive transfer of maternal antibodies to the neonate via the placenta and breast milk, providing protection during the first months of life before the infant's own immunisation schedule begins. The rationale for maternal immunisation extends beyond the mother — the newborn is born immunologically naive to many pathogens and cannot receive most vaccines in the first weeks of life. Maternal IgG antibodies cross the placenta actively in the third trimester, reaching protective concentrations in the cord blood if the mother was immunised sufficiently early.
The safety profile of a vaccine in pregnancy depends almost entirely on whether it is inactivated or live attenuated. Understanding this distinction is the most clinically and examinationally important principle in this topic.
Governing principle for vaccine safety in pregnancy: Inactivated vaccines (killed organisms, toxoids, subunit, mRNA) are SAFE in all trimesters. Live attenuated vaccines are CONTRAINDICATED in pregnancy because of the theoretical (and in some cases documented) risk of infecting the fetus. This distinction is the most testable principle in this domain.
Vaccines INDICATED (recommended) in pregnancy:
1. Tetanus Toxoid / Td (Tetanus-Diphtheria) vaccine — the cornerstone of India's maternal immunisation programme. An inactivated toxoid. The schedule per NHM:
- Primigravidae (first pregnancy) or inadequately immunised: TT1 at the first ANC contact (as early as possible), TT2 at least 4 weeks after TT1 (minimum 4-week interval is mandatory). Both doses should be given, ideally completing TT2 before 36 weeks.
- Previously fully immunised women (completed primary series and received a booster within 3 years): A single booster dose (1 TT/Td dose) in the current pregnancy is sufficient.
- The interval to delivery after the last dose should be ≥4 weeks for the maternal antibody to reach protective titres that can be transferred to the neonate.
- Tetanus protection to the neonate: Maternal IgG anti-tetanus antibodies cross the placenta and protect the neonate against neonatal tetanus (tetanus neonatorum) in the critical first weeks of life.
- Influenza vaccine (inactivated, trivalent/quadrivalent) — recommended for all pregnant women in any trimester, especially during flu season. Pregnancy increases the risk of severe influenza complications (pneumonia, preterm labour, ICU admission). The inactivated vaccine is safe; live attenuated influenza vaccine (LAIV/FluMist) is contraindicated in pregnancy.
- COVID-19 vaccines (mRNA and vector-based) — recommended in pregnancy following risk-benefit analysis. Current national guidelines support vaccination in all trimesters; COVID-19 infection in pregnancy is associated with increased risk of preterm birth, ICU admission, and maternal mortality.
Vaccines CONTRAINDICATED in pregnancy (live attenuated):
- MMR (Measles-Mumps-Rubella) — live attenuated; theoretical risk of fetal infection; defer until postpartum (give immediately postpartum).
- Varicella vaccine — live attenuated; varicella in pregnancy causes congenital varicella syndrome, but the vaccine virus can also theoretically infect the fetus; contraindicated.
- Oral Polio Vaccine (OPV) — live attenuated; IPV (inactivated polio) is the safe alternative.
- Yellow fever vaccine — live attenuated; generally contraindicated but may be given if travel to high-risk endemic area is unavoidable.
- Typhoid oral vaccine (Ty21a capsule) — live; injectable Vi polysaccharide typhoid vaccine (inactivated) is safe.
Counselling on vaccination: Address vaccine hesitancy directly and calmly. Key messages: (a) The TT vaccine protects both mother and baby from life-threatening tetanus. (b) The vaccine does NOT contain live bacteria and cannot cause tetanus. (c) Mild local soreness and low-grade fever after the injection are common and do not require stopping the vaccine. (d) Vaccination is free and available at every PHC, sub-centre, and hospital.
Provided image
SELF-CHECK
Which of the following vaccines is SAFE to administer in the first trimester of pregnancy?
A. MMR (Measles-Mumps-Rubella)
B. Varicella vaccine
C. Tetanus Toxoid (TT/Td) vaccine
D. Oral polio vaccine (OPV)
Reveal Answer
Answer: C. Tetanus Toxoid (TT/Td) vaccine
The Tetanus Toxoid (TT) and Td vaccines are inactivated toxoids and are safe in all trimesters — they are in fact recommended in pregnancy and form the backbone of neonatal tetanus prevention. MMR and varicella are live attenuated vaccines and are contraindicated in pregnancy. OPV is also live attenuated and contraindicated — inactivated polio vaccine (IPV) is the safe alternative.
Interpreting Findings and Identifying Risk
After taking a dietary history and reviewing the vaccination card, the clinician must synthesise findings into a risk assessment and act accordingly. The following clinical patterns require specific management responses:
Anaemia detected (Hb <11 g/dL): First, grade severity — mild (10–10.9 g/dL), moderate (7–9.9 g/dL), severe (<7 g/dL), or very severe/dangerous (<4 g/dL) by WHO classification. For mild-to-moderate iron-deficiency anaemia, double-dose IFA (120 mg elemental iron + 500 µg folic acid, i.e., 2 tablets daily) with enhanced dietary counselling is the NHM first-line approach in pregnancy. Injectable iron sucrose or ferric carboxymaltose is indicated for severe anaemia (Hb <7 g/dL), second-trimester presentations with inadequate time for oral therapy, malabsorption, or documented intolerance. Blood transfusion is reserved for haemodynamically significant anaemia (Hb <5–6 g/dL near term or symptomatic). Always screen for non-nutritional causes of anaemia (thalassaemia trait, sickle cell disease) in high-prevalence areas using peripheral smear and HPLC where available.
Inadequate weight gain: Assess for food insecurity, hyperemesis gravidarum, uncontrolled diabetes, and — crucially — fetal growth restriction using serial symphysis-fundal height measurements. Refer for targeted nutritional support under the Pradhan Mantri Matru Vandana Yojana (PMMVY) and Integrated Child Development Services (ICDS) supplementary nutrition programmes.
Excessive weight gain (>1 kg/week especially in third trimester): Raises the suspicion of fluid retention, gestational hypertension, or oedema. Check blood pressure and urine protein. Do not attribute all weight gain to nutrition alone — oedema is a different diagnosis requiring different management.
Incomplete or absent vaccination: If TT1 and TT2 have not been given, initiate the schedule immediately regardless of gestational age. If TT2 cannot be completed 4 weeks before the due date due to late presentation, give at least TT1 — some protection is better than none. Record accurately in the ANC card and ensure the patient understands the importance of completing the schedule.
Vaccination refusal: Explore concerns, provide accurate information, and document the conversation in the ANC record. Never coerce. Revisit at the next ANC contact.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
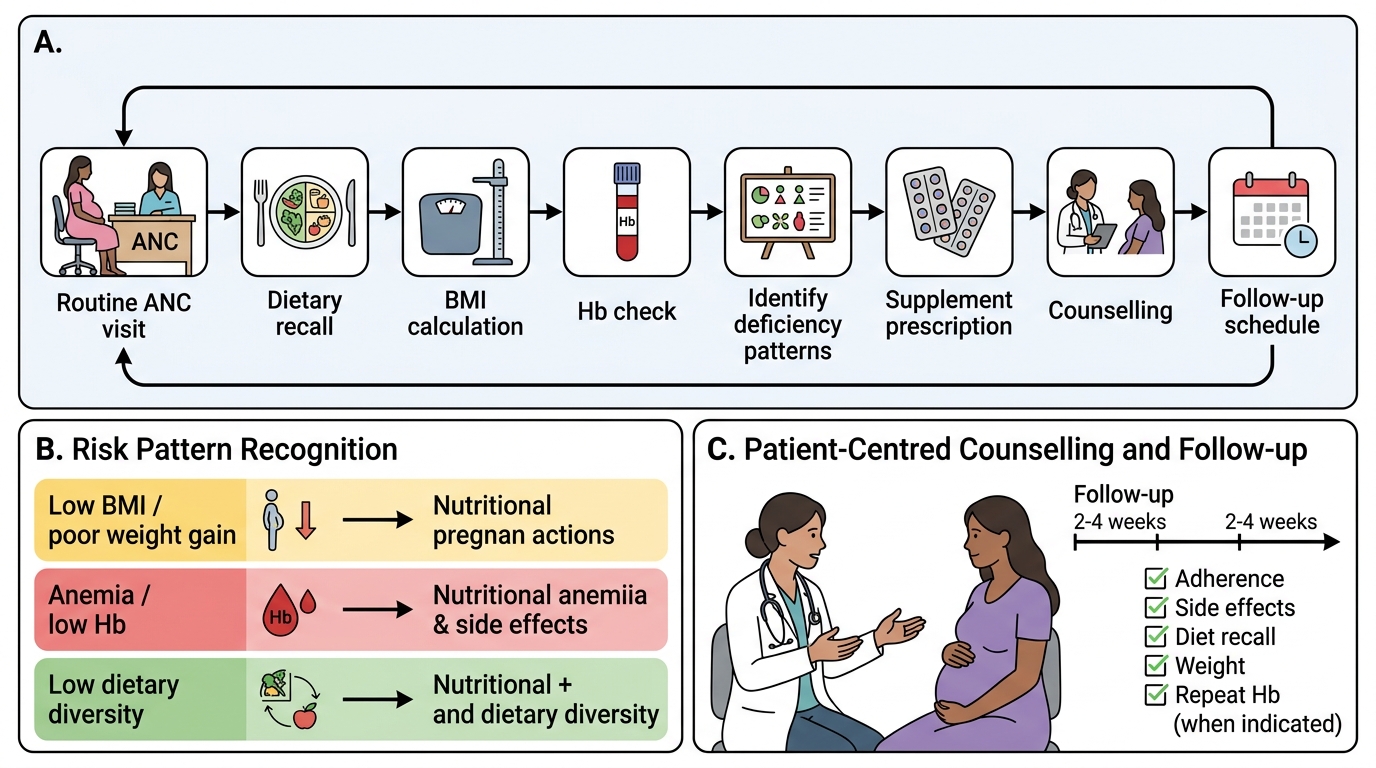
Nutritional Risk Assessment Flow in Antenatal Care
Applied Practice — Counselling in Simulated ANC
In the OSCE (Objective Structured Clinical Examination) and in your clinical postings you will be asked to conduct a 5–10 minute nutritional and vaccination counselling station with a simulated or real ANC patient. This section provides a structured approach to performing this skill at the SH (Skill under Supervision) level as required by OG8.6. The OSCE station typically presents a standardised patient who may be expressing concern about supplement side effects, requesting to stop the IFA tablet, or unaware that her vaccination card is incomplete. The examiner expects you to work through the assessment and counselling in a logical, empathetic, and clinically correct sequence — not just recall facts, but demonstrate the skill of communicating them effectively to a patient with limited health literacy. Practising this checklist mentally before entering the station, and rehearsing the exact phrasing for explaining IFA side effects and TT scheduling, will give you a significant advantage. Supervision in clinical postings gives you the opportunity to observe experienced clinicians integrate nutrition and vaccination counselling smoothly into a 5-minute ANC contact — observe what they prioritise when time is limited.
Structured counselling checklist for a simulated ANC nutritional + vaccination station:
- Introduce and establish rapport: Greet the patient by name, introduce yourself, and explain the purpose of the session ('Today we will talk about your diet and iron tablets, and also check your vaccination status').
- Weight review: Weigh the patient and compare to the previous visit. Praise appropriate weight gain. If below target, explore dietary intake. If above target (especially sudden fluid weight), check BP and urinalysis.
- 24-hour dietary recall: Use open questions ('Tell me what you ate yesterday — starting from morning'). Identify sources of iron (dark green vegetables, legumes, eggs, meat, fish), calcium (dairy, ragi/finger millet, sesame seeds), and folate. Identify inhibitors (tea, coffee, phytate-rich unfermented foods).
- Supplement counselling: Confirm the patient is taking IFA (1 tablet = 60 mg elemental iron + 500 µg folic acid) and calcium (2 × 500 mg tablets). Address side effects (nausea → take after food; constipation → increase water and roughage; black stools → reassure, not harmful). Reinforce duration: minimum 180 days, ideally from first contact through delivery and 3 months postpartum.
- Vaccination review: Check the ANC card for TT/Td record. If no doses: explain neonatal tetanus, give TT1 today (or arrange), and schedule TT2 at ≥4 weeks. If TT1 done: check interval — give TT2 if ≥4 weeks since TT1. If previously fully immunised within 3 years: one booster only. Document accurately.
- Structured closing: Summarise the key action points for the patient: 'One iron tablet every day after food, two calcium tablets, continue your iodised salt, eat more dal and leafy vegetables, come back for your second tetanus injection on [date]'. Ask if she has any questions. Provide the ANC card back with entries updated.
Common examiner-observed errors at OSCE nutrition/vaccination stations:
- Giving the wrong IFA dose (e.g., stating 30 mg or 100 mg elemental iron).
- Stating TT can be given in both arms on the same day (it cannot — TT1 and TT2 must be ≥4 weeks apart).
- Failing to address vaccine hesitancy or sidestepping the patient's concerns.
- Not checking previous vaccination history before prescribing the schedule.
- Forgetting calcium supplementation entirely.
- Telling a patient to STOP IFA because of black stools (black stools are expected and harmless — stopping IFA for this reason is incorrect).