Page 23 of 30
OG8.10 | Post-Caesarean Pregnancy — SDL Guide (Part 2)
Management — TOLAC/VBAC: Eligibility, Counselling, and Success Predictors
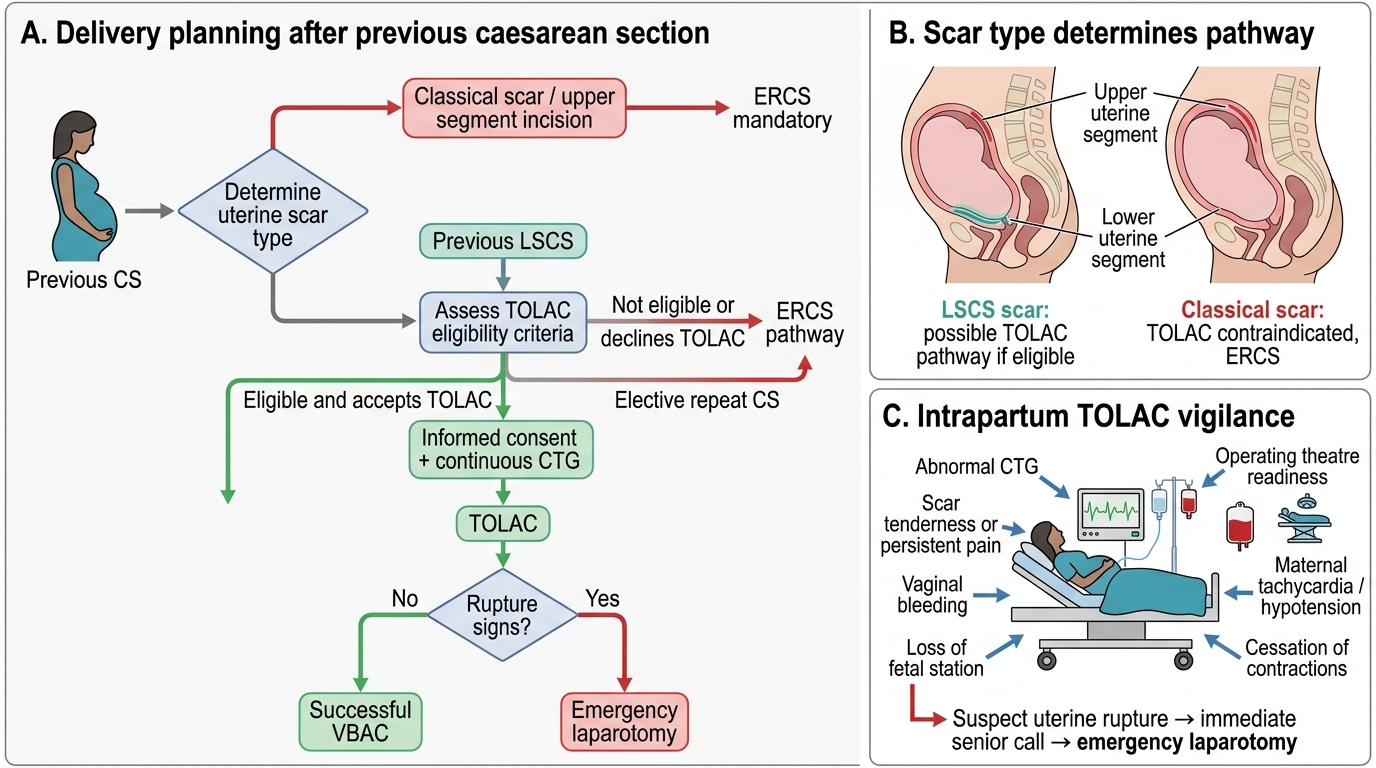
Once contraindications have been excluded, management of post-caesarean pregnancy shifts decisively toward shared decision-making — one of the most nuanced counselling tasks in obstetrics. The clinician must present the woman with a personalised comparison of two pathways: TOLAC (Trial of Labour After Caesarean), which offers the possibility of vaginal birth with its associated benefits of shorter recovery, avoidance of surgical morbidity, and improved outcomes in future pregnancies, but carries a small but real risk of uterine rupture (~0.5% with an LSCS scar); and ERCS (Elective Repeat Caesarean Section), which eliminates the immediate rupture risk but is a major abdominal surgery with cumulative morbidity that increases with each repeat procedure. This is not a situation where one answer fits all — the decision depends on the woman's individual risk profile, her values and preferences regarding labour and surgery, her reproductive plans, and the institutional capabilities available to her. The process begins with formal eligibility assessment and culminates in an informed, documented, woman-centred decision.
TOLAC eligibility criteria (all must be met for TOLAC to be offered):
1. One previous lower-segment transverse caesarean section
2. No previous classical, inverted-T, J, or low-vertical uterine incision
3. No previous uterine rupture
4. No absolute obstetric contraindication to vaginal delivery in this pregnancy (e.g., placenta praevia, brow presentation)
5. Clinically or radiologically adequate pelvis (no absolute CPD)
6. Singleton pregnancy with cephalic presentation
7. Institution capable of immediate emergency CS (24-hour anaesthetic and theatre availability)
VBAC success predictors — presented as modifiable and non-modifiable:
The overall VBAC success rate in well-selected TOLAC candidates is approximately 60–80%. The following factors individually and additively improve success rates:
- Prior vaginal delivery (including previous VBAC): this is the single strongest predictor; women with a prior VBAC have VBAC success rates of >85–90%
- Non-recurrent indication for previous CS (e.g., fetal distress, malpresentation now corrected): the underlying indication is unlikely to recur
- Spontaneous onset of labour: TOLAC with spontaneous labour has a significantly better success rate than induced TOLAC; induction with oxytocin approximately doubles rupture risk compared to spontaneous TOLAC (oxytocin 0.9–1.0% vs spontaneous ~0.4%), and prostaglandins are generally contraindicated for TOLAC due to unacceptable hyperstimulation and rupture risk
- Favourable cervical status (Bishop score ≥6 on admission in spontaneous labour)
- Non-obese BMI (BMI <30): maternal obesity independently reduces VBAC success
- Estimated fetal weight <4 kg: macrosomia reduces cephalic fit and increases likelihood of obstructed labour
- Age <35 years: older maternal age modestly reduces VBAC success rates
Factors that make VBAC LESS likely but do not necessarily contraindicate TOLAC: induction of labour (higher failure and rupture rates — requires very careful case selection and close monitoring), BMI ≥30, estimated fetal weight ≥4 kg, no prior vaginal deliveries, labour not yet in progress.
Counselling framework: Informed consent for TOLAC must include: (1) estimated VBAC success rate personalised to the woman's predictors; (2) rupture risk with TOLAC (~0.5% LSCS scar); (3) what uterine rupture means clinically (emergency laparotomy, possible hysterectomy, fetal risk); (4) comparison with ERCS risks (increased surgical morbidity, longer recovery, scar complications in future pregnancies especially placenta accreta spectrum with increasing numbers of CS); (5) the requirement for continuous CTG monitoring and IV access; (6) the right to change her decision.
Post-Caesarean Delivery Planning and TOLAC Safety Algorithm
Management — Intrapartum TOLAC and Recognising Uterine Rupture
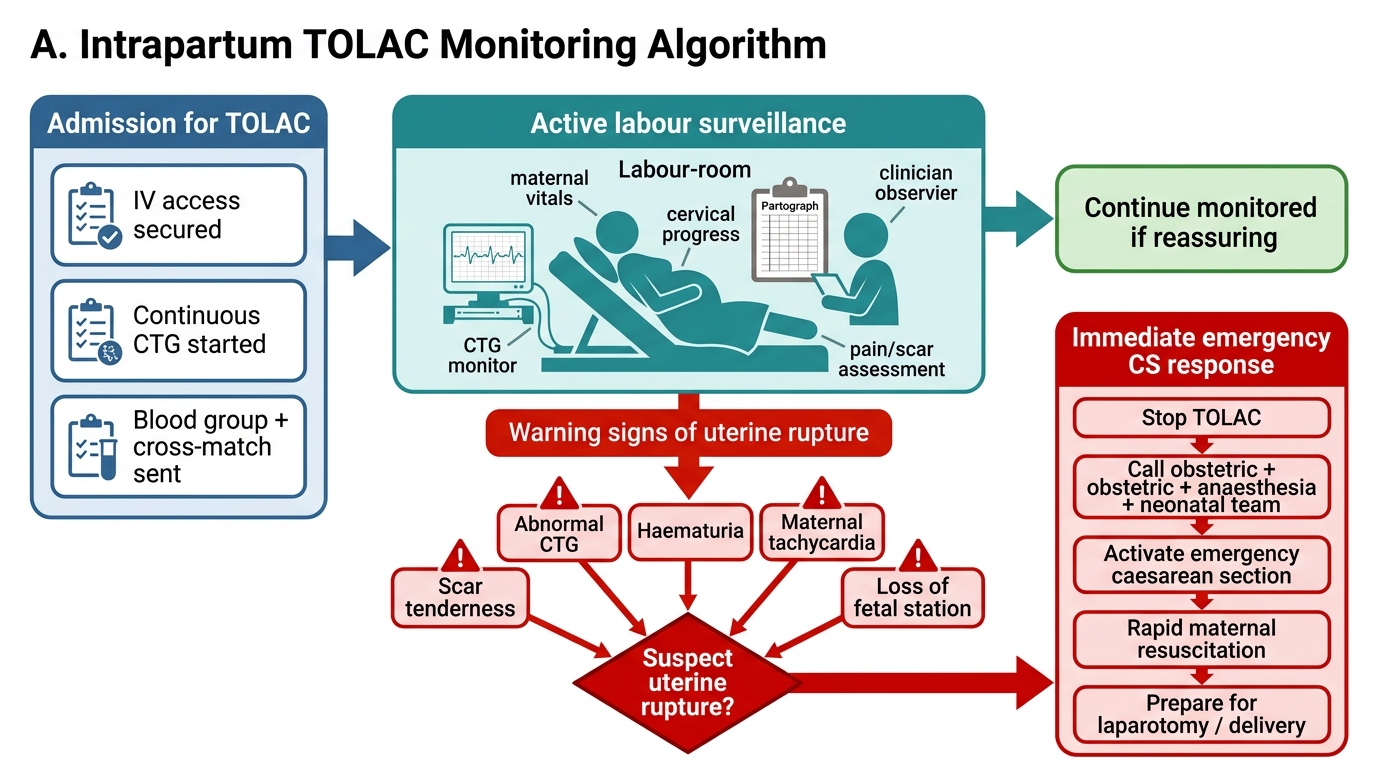
Intrapartum management of a woman undergoing TOLAC is categorically distinct from managing a standard labour. The presence of a uterine scar introduces a low but life-altering risk — uterine rupture — that demands a level of vigilance, preparation, and rapid response capacity beyond what routine labour monitoring provides. Unlike most intrapartum complications, uterine rupture can escalate from warning signs to catastrophic maternal-fetal compromise within minutes: the window for fetal salvage after complete rupture is typically no more than 10–37 minutes, and that window begins not when rupture is confirmed but when it is first suspected. This is why every member of the team caring for a TOLAC patient — the resident, the midwife, the anaesthetist on call — must be primed to act before the picture is unambiguous. The protocol that follows is not simply a checklist; it is a system designed so that when the clinical warning signs appear, the response is immediate and rehearsed rather than delayed by deliberation.
Intrapartum protocol for TOLAC:
1. IV access and cross-match at admission (blood should be available within the blood bank, not necessarily pre-transfused)
2. Continuous electronic fetal monitoring (CTG) throughout active labour — this is mandatory, not optional. Intermittent auscultation is NOT acceptable for TOLAC
3. Active participation of senior obstetric staff — TOLAC should not be managed by a junior resident alone
4. Immediate theatre availability — team must be able to perform emergency CS within 30 minutes (many centres aim for 15 minutes)
5. Careful use of oxytocin if augmentation is required — use the minimum effective dose; high-dose oxytocin regimens are associated with uterotonic hyperstimulation and increased rupture risk. Prostaglandins (misoprostol, PGE₂) are contraindicated for cervical ripening/induction in TOLAC
6. No epidural mandate — epidural analgesia is not contraindicated in TOLAC but the concern that it masks rupture pain is largely unfounded; epidurals can be offered with appropriate counselling
7. Scar palpation — some clinicians palpate the lower uterine segment at full dilatation or post-delivery, but this has poor sensitivity and specificity for scar integrity and is not a substitute for clinical vigilance
Recognising impending uterine rupture — the warning signs:
Uterine rupture typically gives warning before complete disruption. Early recognition requires active surveillance for:
- Scar site pain or tenderness, especially between contractions (the normal contraction pain of labour is felt during contractions, not between them; inter-contraction lower segment tenderness is a warning sign)
- CTG abnormalities: prolonged late decelerations, persistent fetal bradycardia, or sudden profound fetal heart rate change — these are the most reliable early signs; CTG abnormality is present in >70% of ruptures
- Maternal tachycardia and hypotension — signs of haemorrhage from a significant rupture
- Haematuria — bladder involvement in rupture produces blood-stained urine; it is pathognomonic when present
- Loss of fetal station — the presenting part rises on vaginal examination as the fetus is expelled or retracts into the peritoneal cavity
- Cessation of uterine contractions (the uterus may stop contracting once it ruptures, causing apparent relief of pain — do not be falsely reassured)
- Maternal collapse, peritonism, and acute abdomen — signs of established complete rupture
Management of uterine rupture:
Once rupture is suspected clinically, the response is: (1) emergency CS — call theatre immediately, do not await confirmation with investigations; (2) two large-bore IV cannulae, fluid resuscitation; (3) cross-match and activate massive haemorrhage protocol if haemodynamically compromised; (4) at laparotomy — deliver the fetus, control haemorrhage, assess the rupture site; (5) uterine repair vs hysterectomy depending on the extent of rupture, surgeon skill, and the woman's desire for future fertility. Extension into bladder or uterine vessels mandates urgent repair or hysterectomy.
Intrapartum TOLAC Monitoring Algorithm
Management — Elective Repeat Caesarean Section (ERCS)
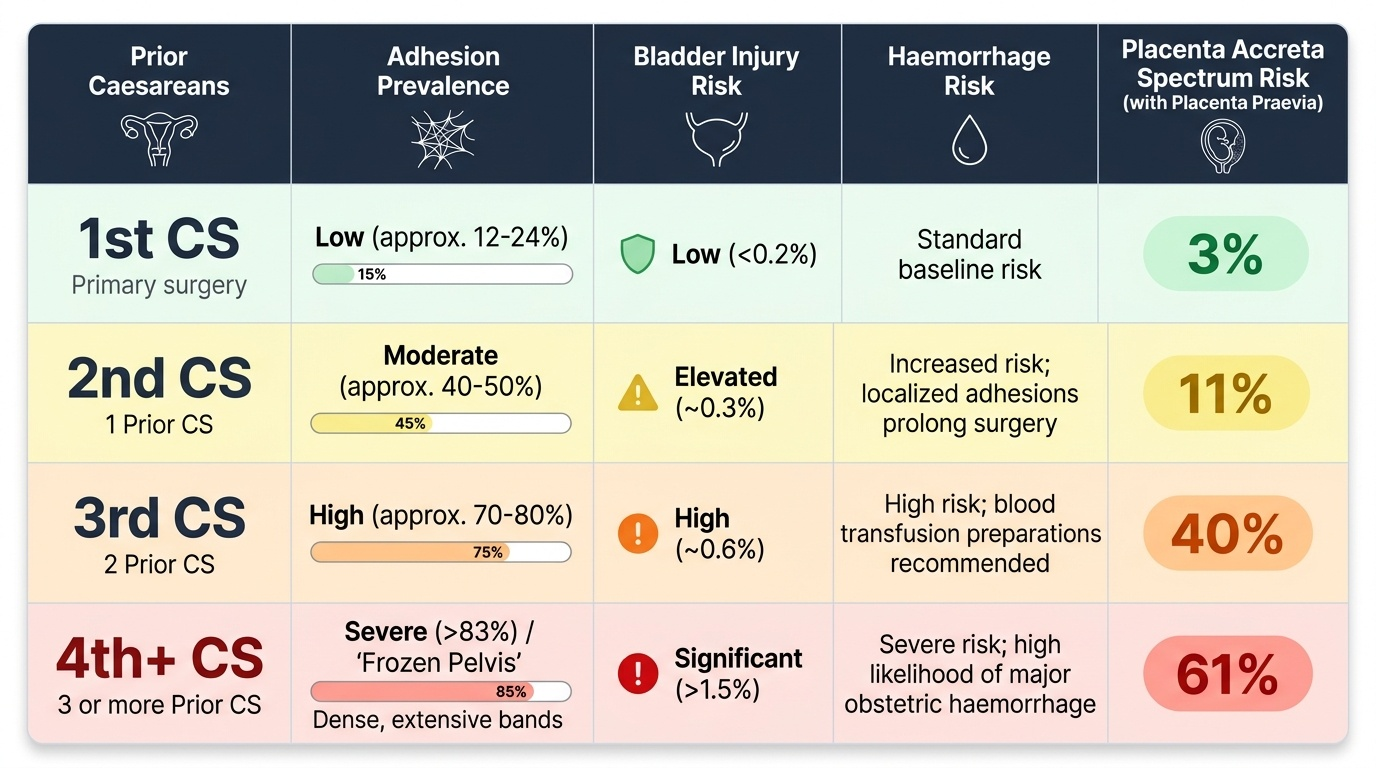
Elective Repeat Caesarean Section (ERCS) is the planned delivery by repeat caesarean at a gestational age and time determined in advance — not in response to a new complication in labour, but as the primary pre-specified delivery mode chosen antenatally. It is the appropriate pathway for all women with contraindications to TOLAC, and it is also a valid choice for eligible women who, after thorough counselling, prefer the predictability and controlled setting of planned surgery over the uncertainty of labour. The clinician's role is not to steer the woman toward or away from ERCS but to ensure her decision is genuinely informed — that she understands both the immediate risks of repeat surgery and the longer-term cumulative consequences that accrue with each additional caesarean. These cumulative risks are not trivial and constitute one of the strongest arguments for reducing primary caesarean rates: a woman who has had four or more caesareans faces haemorrhage risks, adhesion densities, and placenta accreta spectrum probabilities that fundamentally change the risk calculus of each delivery. Understanding ERCS therefore requires understanding not just the single operation but the reproductive trajectory it implies.
Indications for ERCS (primary — i.e., TOLAC not offered):
- Previous classical, T, J, or low-vertical uterine incision
- Previous uterine rupture
- Two or more previous lower-segment CS without any prior vaginal delivery
- Absolute contraindication to vaginal delivery in the current pregnancy (e.g., placenta praevia, brow/shoulder presentation unamenable to correction)
- Institutional inability to provide 24-hour emergency CS cover
Indications for ERCS (by patient choice after balanced counselling): Women eligible for TOLAC who, after being fully informed, decline it and prefer planned CS. This is a valid and respected choice — the role of the clinician is to ensure the decision is truly informed, not to coerce.
Optimal timing of ERCS: ERCS should ideally be performed at ≥39 weeks of gestation. This is because neonatal respiratory morbidity (transient tachypnoea of the newborn, respiratory distress syndrome) is significantly higher in elective CS performed before 39 weeks compared to 39+ weeks. Performing ERCS at 38 weeks doubles the risk of neonatal respiratory complications compared to 39 weeks; at 37 weeks the risk is approximately 3–4-fold higher. The argument for earlier timing (37–38 weeks) applies only when there is a clinical indication such as previous classical CS (concern about scar rupture before labour onset) or obstetric complication requiring earlier delivery.
Complications of repeat CS — cumulative with each operation:
- Adhesions: peritoneal and bladder adhesions are present in ~50% of second CS, ~75% of third CS, increasing operative time, blood loss, and risk of inadvertent injury
- Bladder injury: the risk increases with each successive caesarean due to adhesions displacing the bladder upward
- Haemorrhage: greater blood loss at each repeat CS; average blood loss at third CS is approximately twice that at first CS
- Placenta accreta spectrum (PAS): the single most important long-term morbidity of multiple CS. PAS — including placenta accreta, increta, and percreta — occurs when placental trophoblast invades the myometrium through the CS scar. Risk with placenta praevia: ~3% with 1 prior CS, ~11% with 2 prior CS, ~40% with 3 prior CS, ~61% with 4 or more prior CS. PAS can cause catastrophic haemorrhage requiring hysterectomy and carries high maternal mortality
- Longer hospitalisation and recovery: recovery from repeat CS is typically longer than from a first CS due to adhesion-related surgical complexity
- Increased anaesthetic risk: cumulative exposure; prior abdominal surgeries may complicate regional anaesthesia positioning
These cumulative risks are a central argument for offering TOLAC to eligible women and for limiting first caesareans to genuine indications — the primary CS prevention policy.
Provided image
SELF-CHECK
Which factor is the SINGLE STRONGEST predictor of VBAC success in a woman undergoing TOLAC?
A. Spontaneous onset of labour
B. Previous vaginal delivery (including previous VBAC)
C. Lower uterine segment thickness ≥3.5 mm on ultrasound
D. Favourable Bishop score (≥8) on admission
Reveal Answer
Answer: B. Previous vaginal delivery (including previous VBAC)
A previous vaginal delivery — including a previous VBAC — is the single strongest individual predictor of VBAC success, with success rates of >85–90%. While spontaneous labour onset and a favourable cervix also improve success rates, prior vaginal delivery demonstrates that the pelvis-cephalic relationship is capable of normal delivery and the uterus can sustain productive labour.
SELF-CHECK
A woman with one previous LSCS, spontaneous onset of labour at 39 weeks, and a cephalic singleton is managed as TOLAC with continuous CTG. At 7 cm dilatation, the CTG shows a prolonged deceleration to 80 bpm lasting 4 minutes with slow recovery, and the woman complains of inter-contraction lower-segment pain. The MOST appropriate immediate action is:
A. Start oxytocin augmentation and recheck CTG in 30 minutes
B. Perform amniotomy to accelerate labour
C. Call for senior obstetric review and prepare for immediate caesarean section
D. Administer terbutaline and observe for CTG improvement
Reveal Answer
Answer: C. Call for senior obstetric review and prepare for immediate caesarean section
This presentation — prolonged CTG deceleration combined with inter-contraction lower-segment tenderness — is a high-probability sign of impending or established uterine rupture. The appropriate response is immediate senior obstetric review and preparation for emergency CS. Terbutaline may be given to temporarily improve fetal condition if there is a brief delay to theatre, but it does not treat the rupture. Starting oxytocin or amniotomy would be dangerous. Every minute of delay in this scenario worsens fetal and maternal outcomes.
SELF-CHECK
An elective repeat caesarean section (ERCS) is planned. What is the recommended optimal gestational age for ERCS in an uncomplicated post-LSCS pregnancy?
A. 37 weeks, to avoid the risk of labour onset before the scheduled surgery
B. 38 weeks, balancing fetal maturity against risk of labour onset
C. ≥39 weeks, to minimise neonatal respiratory morbidity
D. 40 weeks, to allow maximum fetal maturity
Reveal Answer
Answer: C. ≥39 weeks, to minimise neonatal respiratory morbidity
ERCS should ideally be performed at ≥39 weeks of gestation. Neonatal respiratory morbidity (transient tachypnoea, RDS) is significantly higher when elective CS is performed before 39 weeks. At 38 weeks the risk is approximately doubled compared to 39 weeks; at 37 weeks it is 3–4 times higher. The risk of spontaneous labour onset before a scheduled ERCS at 39 weeks is low (~5–8%) and is managed by counselling the woman to present immediately if labour begins.