Page 24 of 30
OG8.10 | Post-Caesarean Pregnancy — SDL Guide (Part 3)
Consolidating Your Understanding — Self-Assessment Framework
Having worked through the clinical presentation, pathophysiology, diagnostic assessment, and management pathways for post-caesarean pregnancy, you are now equipped to integrate this knowledge into clinical reasoning. The self-assessment section asks you to test that integration — not merely recall isolated facts, but apply them to clinical scenarios of the kind you will encounter in wards, clinics, and examinations.
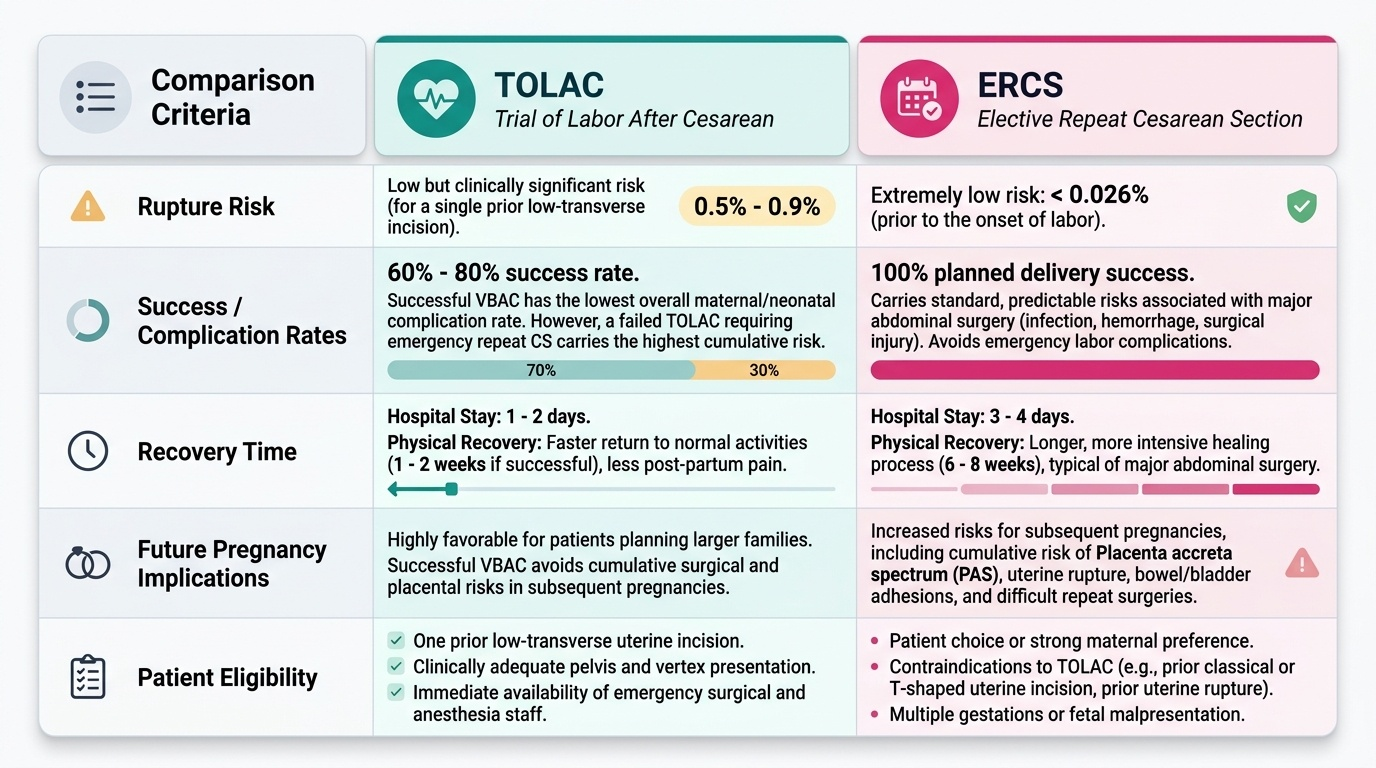
A useful self-check framework for any post-CS pregnancy case is the acronym SCARE: Scar type (lower-segment transverse vs classical/other), Contraindications to TOLAC (enumerate and apply), Adequacy of pelvis and presentation, Rupture risk figures and warning signs, ERCS indications and timing. Running this framework mentally over each case ensures no critical element is omitted before making or documenting a delivery plan.
The micro-quiz questions that follow are drawn from the key decision points in this module. As you answer, note not just the correct option but the reasoning chain that eliminates the distractors — that reasoning chain is what you will need in a viva or at the bedside.
Provided image
CLINICAL PEARL
The scar type overrides everything else. Before discussing TOLAC success rates, fetal weight, pelvic adequacy, or CTG capabilities, establish the type of uterine incision. A classical scar — regardless of all other favourable factors — is an absolute contraindication to TOLAC. This is one of the few binary decisions in obstetric management where evidence is unequivocal and clinical judgement does not modify the answer. In practice, many women (and some clinicians) do not know the scar type; if operative notes are unavailable, default to ERCS. The consequences of an unrecognised classical scar rupturing in labour are irreversible.