Page 7 of 23
OG9.3 | Early Pregnancy Evacuation — SDL Guide
Learning Objectives
- Identify the clinical indications for early pregnancy evacuation in both spontaneous loss and MTP settings
- Describe the anatomy relevant to safe cannula insertion and recognise the significance of uterine position
- Outline the step-by-step technique of medical abortion (mifepristone + misoprostol) and manual vacuum aspiration (MVA)
- Describe how complete evacuation is confirmed and recognise intraoperative complications
- Explain the post-procedure monitoring, anti-D administration, and follow-up requirements
- State the MTP Act 2021 requirements for lawful termination
INSTRUCTIONS
Early pregnancy evacuation is one of the commonest procedures in obstetrics and gynaecology — performed for incomplete or missed abortion, inevitable abortion, and for medical termination of pregnancy (MTP). As a Phase III student, your competency (OG9.3) requires you to describe the steps and to observe or assist in the procedure, not to perform it independently. This module equips you to understand the procedure thoroughly enough to anticipate each step at the bedside, recognise when something goes wrong, and communicate clearly with the patient and the operating team. The legal framework (MTP Act) is equally important — you must know the limits and the safeguards.
References
- WHO Safe Abortion: Technical and Policy Guidance for Health Systems, 3rd ed, 2022 (guideline)
- DC Dutta's Textbook of Obstetrics, 9th ed, Chapter 10 & 38 (textbook)
- FOGSI Good Clinical Practice Recommendations on Safe MTP, 2020 (guideline)
- Medical Termination of Pregnancy (Amendment) Act 2021, MTP Rules 2021 (legislation)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 24-year-old woman is brought to the emergency unit with heavy bleeding and passage of some tissue at 8 weeks of pregnancy. On examination, the cervical os is open and there is retained tissue on ultrasound. The doctor on call tells you: 'She needs an MVA — come and watch.' Before you walk into that procedure room, you need to know: What is the doctor going to do, step by step? What instruments are on the tray? What complication might arise, and how would the team respond? And — if she asks you — what exactly happened to her pregnancy?
WHY THIS MATTERS
Uterine evacuation procedures are performed daily in every district hospital, medical college, and private maternity unit in India. In the public sector, access to safe, evidence-based evacuation is a critical component of maternal healthcare — the WHO estimates that complications from unsafe abortion procedures account for approximately 7–13% of all maternal deaths globally. In India, the MTP Act 2021 has broadened access to safe termination, and medical colleges are required to train students to observe and assist in these procedures. Understanding the technique — including what can go wrong — also makes you a better advocate for patients when they ask whether a procedure was performed correctly. This is not optional knowledge; it is a clinical competency mandated by the NMC for Phase III MBBS.
RECALL
Before you begin, recall the following from earlier modules. From anatomy and OG2: the cervix consists of the external os (visible on speculum), the cervical canal, and the internal os (at the junction with the uterine cavity); the uterus may be anteverted/anteflexed or retroverted/retroflexed — the axis of the uterine cavity changes accordingly, affecting the safe direction of instrument insertion. From pharmacology: misoprostol is a prostaglandin E1 (PGE1) analogue that causes cervical softening and uterine contractions; mifepristone is an antiprogestogen that sensitises the uterus to prostaglandins. From OG9.1: incomplete abortion = retained products with open os; missed abortion = dead fetus, closed os — both require evacuation.
Clinical Indication and Relevance
Uterine evacuation of the uterus in early pregnancy is a core obstetric intervention performed across all levels of the healthcare system, from district hospitals to tertiary medical colleges, and is among the most commonly performed gynaecological procedures in India. It is indicated in two broad and conceptually distinct categories: first, the management of pregnancy failure or complications — where the pregnancy is wanted but has been lost — and second, medical termination of pregnancy (MTP) — where the woman has chosen or been advised to end a potentially viable pregnancy. These two categories share the same procedural techniques but differ fundamentally in their legal requirements, their ethical dimensions, and the emotional context of the consultation. Understanding which indication applies in a given case is clinically important because it determines the legal framework, the urgency of the procedure, the pre-procedure counselling, and the documentation required before the patient consents.
For spontaneous pregnancy complications, evacuation is indicated in the following situations:
- Incomplete abortion: retained products of conception with open cervical os and ongoing bleeding; urgent evacuation is required to prevent haemorrhage and infection
- Inevitable abortion: open os, heavy bleeding — evacuation is both therapeutic and preventive
- Missed abortion: retained non-viable fetus with closed os; evacuation is required (urgency is less acute, allowing time for medical management) to prevent consumptive coagulopathy (rare but dangerous after prolonged retention >4 weeks) and patient psychological suffering
- Septic abortion: evacuation must be performed AFTER antibiotic stabilisation (within 1–2 hours of starting antibiotics) — not days later
For MTP (induced termination), evacuation is performed in accordance with the MTP Act 1971 amended 2021. The key legal requirements are:
- Up to 20 weeks: written opinion of ONE Registered Medical Practitioner (RMP)
- 20–24 weeks: written opinion of TWO RMPs; restricted to specified categories (survivor of sexual assault/rape/incest, minor, change of marital status during pregnancy, women with physical/mental disability, foetal anomaly, humanitarian setting)
- Beyond 24 weeks: substantial foetal abnormality, on approval of a State Medical Board
- All terminations must be performed in a government hospital or an MTP-approved facility
- Sex determination before MTP is PROHIBITED under PCPNDT Act 1994 — never allow a sex-determination request to be framed as an MTP indication
IMPORTANT: The student must never conflate the clinical indication (pregnancy complication requiring evacuation) with the legal indication (MTP Act requirement for induced termination). A woman with a missed abortion does NOT need MTP paperwork — the procedure is therapeutic management of a complication. The MTP framework applies only when the fetus is or was potentially viable and the woman is requesting termination.
SELF-CHECK
Under the MTP Act 2021, a 28-year-old single woman requests termination at 22 weeks after her marriage broke down. How many RMPs must give their written opinion, and is this woman in one of the specified categories?
A. One RMP — all terminations up to 24 weeks require only one opinion
B. Two RMPs — change in marital status during ongoing pregnancy is a specified category
C. Two RMPs — but change in marital status is NOT a specified category
D. A State Medical Board approval is required at 22 weeks
Reveal Answer
Answer: B. Two RMPs — change in marital status during ongoing pregnancy is a specified category
At 22 weeks, TWO RMP opinions are required (the 20-week single-RMP limit has been passed). Change in marital status during ongoing pregnancy is explicitly listed as a specified category under Rule 3B of the MTP Rules 2021, making this woman eligible for termination at 22 weeks with two-RMP approval. State Medical Board approval is only required beyond 24 weeks.
Anatomy and Governing Principles
Safe uterine evacuation depends on a precise three-dimensional mental model of the pelvis — the position of the uterus relative to the cervix, the length and axis of the uterine cavity, and the calibre of the cervical canal — because every instrument (sound, dilator, cannula) must follow the natural uterine axis to avoid creating a false passage or perforating the uterine wall. The commonest cause of uterine perforation during evacuation is failure to account for uterine position. The operator must determine uterine size and position on bimanual pelvic examination before inserting any instrument. This examination takes less than 60 seconds and is non-negotiable. Skipping it — whether from time pressure or overconfidence — is the single most avoidable error in evacuation procedures, and it accounts for a disproportionate share of iatrogenic injuries. The anatomy of the cervix and the principles that govern safe dilatation are equally critical: the cervical canal must be dilated gradually and atraumatically, matching the Hegar dilator size to the gestational age and using cervical priming where appropriate.
Key anatomical points relevant to evacuation:
1. The cervical canal and os:
- The external os is the visible opening on speculum examination — oval in nulliparae, transverse slit in parous women
- The cervical canal connects external to internal os; length ~3 cm; contains mucus plug in early pregnancy
- The internal os marks the boundary between cervix and uterine cavity; in incomplete/inevitable abortion this is the os that opens
- In a closed, unripened cervix, dilatation to the appropriate cannula diameter requires cervical priming with misoprostol (400 µg sublingual 2–3 hours before) or mechanical osmotic dilators
2. Uterine position:
- Anteflexion (most common — ~80%): the uterine body tilts forward over the bladder; the uterine cavity opens anteriorly; the cannula should be directed anteriorly (upward) after passing the internal os
- Retroflexion (~20%): the uterine body tilts posteriorly; the cavity opens backward; the cannula should be directed posteriorly
- Failure to account for retroflexion and inserting anteriorly is the classic mechanism of fundal perforation
3. Uterine size and gestational age:
- At 8 weeks the uterus is a large orange; at 12 weeks, a grapefruit
- Cannula size corresponds to gestational weeks: 8 mm cannula for 8 weeks, 10 mm for 10 weeks, 12 mm for 12 weeks
- Beyond 13 weeks: D&E (dilatation and evacuation) with larger-bore instruments; requires more dilatation and may need osmotic dilators the night before
4. Governing safety principles:
- Bimanual examination FIRST to establish uterine size and position
- Cervical priming/dilatation commensurate with gestational age
- Gentle instrument insertion following uterine axis
- Never force a dilator against resistance — reassess uterine position
- Uterine sound to measure cavity length before cannula (confirms length before inserting wider instrument)
- Antibiotic prophylaxis: doxycycline 100 mg oral 1 hour before (or azithromycin 500 mg single dose)
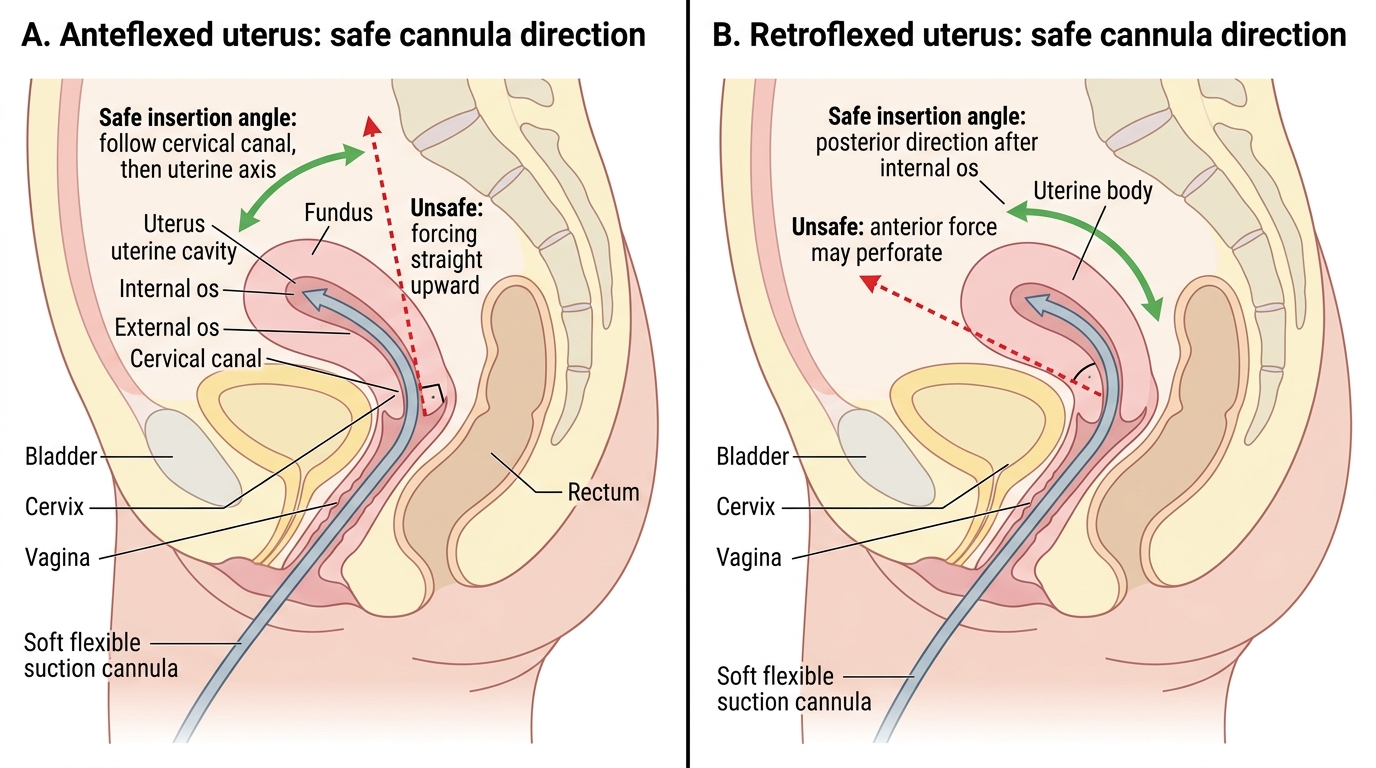
Safe Cannula Direction in Anteflexed and Retroflexed Uterus
Procedure and Technique
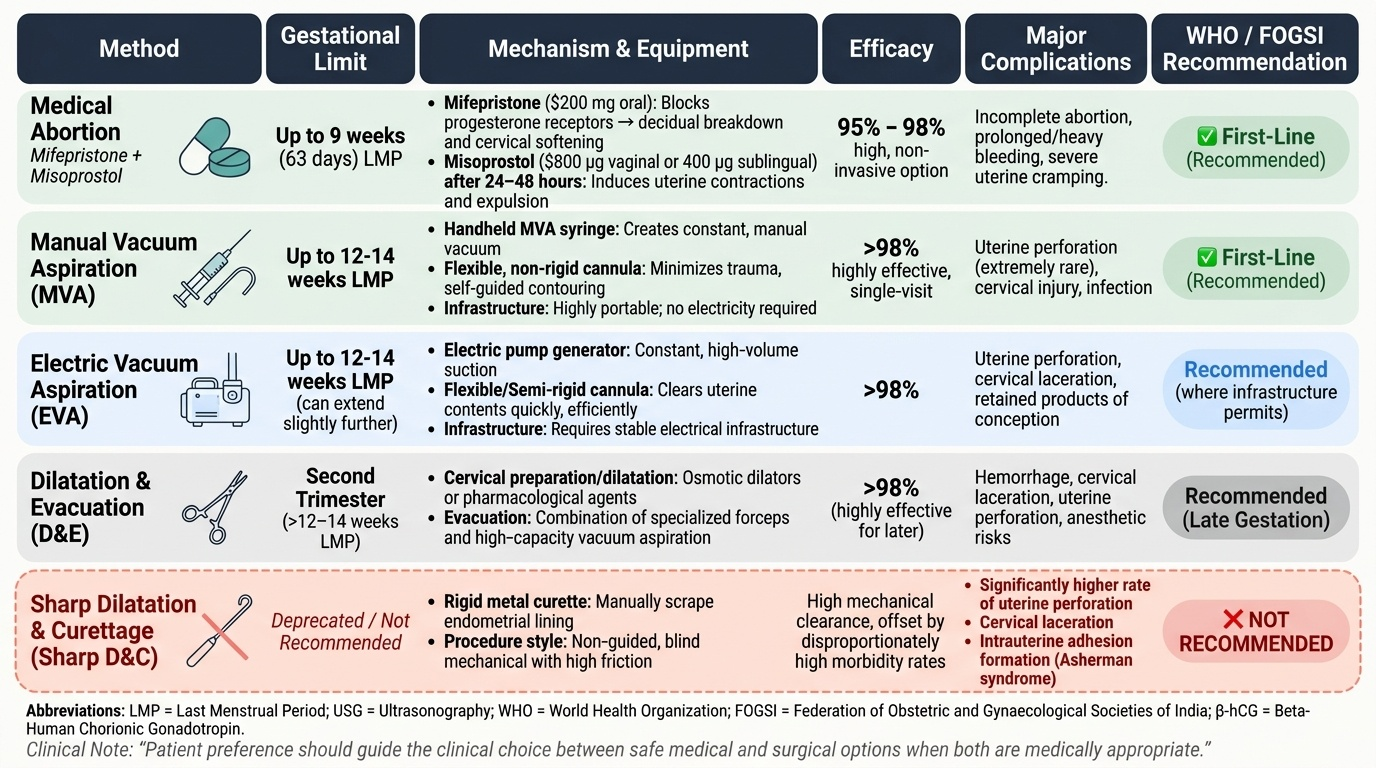
The available early pregnancy evacuation techniques fall into two primary categories: medical (pharmacological) methods that use drugs to induce uterine contractions and expulsion, and surgical methods that remove the products of conception instrumentally. Within the surgical category, the choice between manual vacuum aspiration (MVA), electric vacuum aspiration (EVA), and dilatation and evacuation (D&E) is determined primarily by gestational age and available infrastructure. The choice between medical and surgical management, where both are appropriate, is increasingly guided by patient preference — for women who prefer to avoid an invasive procedure or who are managing an early missed abortion at home, medical management is safe and effective; for women who prefer a single-visit surgical solution, MVA is preferred. The WHO and FOGSI actively recommend medical management or vacuum aspiration as first-line for early pregnancy evacuation, and have specifically recommended AGAINST sharp curettage with a metal curette as a routine technique, because the metal curette is rigid, non-guided, and carries significantly higher rates of uterine perforation, cervical laceration, and intrauterine adhesion (Asherman syndrome) formation compared to the flexible, suction-based MVA cannula.
A. Medical Abortion:
Combination regimen (first-line up to 63 days/9 weeks LMP — most effective):
1. Mifepristone 200 mg oral: blocks progesterone receptors → decidual breakdown, cervical softening
2. Wait 24–48 hours
3. Misoprostol 800 µg vaginal (insert into posterior fornix) OR 400 µg sublingual: causes uterine contractions and expulsion
4. Patient returns in 1–2 weeks for confirmation of complete expulsion (USG or β-hCG)
5. If incomplete at follow-up: proceed to MVA
Misoprostol alone (when mifepristone unavailable):
- Misoprostol 800 µg vaginal, repeat at 3 hours if needed
- Less effective than combination (complete abortion ~80% vs ~95–98% with combination)
Beyond 13 weeks (medical induction):
- Mifepristone 200 mg → 24–48 h → misoprostol 400 µg vaginal every 3–6 hours until expulsion
- Requires monitored hospital admission; higher dose/frequency of misoprostol at later gestations
B. Manual Vacuum Aspiration (MVA) — first-line surgical method up to 13 weeks:
Equipment: Karman cannula (sizes 4–12 mm; colour-coded), MVA syringe (60 mL with two valves and plunger), cervical tenaculum (single-tooth forceps to grasp cervix), uterine sound, Hegar dilators (series 1–12), speculum, Sims vaginal retractor, ring forceps, antiseptic (povidone-iodine), local anaesthetic (paracervical block with lignocaine 1%).
Step-by-step MVA technique:
1. Pre-procedure: verbal consent, bimanual examination to assess uterine size/position; cervical priming if indicated (misoprostol 400 µg sublingual 2–3 hours before for gestations ≥9 weeks or nulliparae)
2. Preparation: empty bladder, lithotomy position, antiseptic preparation of vulva, vagina, cervix
3. Speculum insertion: Sim's speculum (lower blade) and anterior vaginal wall retraction OR bivalve speculum; visualise cervix
4. Paracervical block: inject 5 mL of 1% lignocaine at 4 o'clock and 8 o'clock positions at cervicovaginal junction; wait 3 minutes
5. Tenaculum: grasp anterior lip of cervix (or posterior if retroverted) — this stabilises the cervix and straightens the uterocervical angle
6. Sound: gentle insertion of uterine sound in the axis of the uterine cavity to determine cavity length
7. Cervical dilatation: Hegar dilators in sequence (start with smallest) until diameter matches gestational age in weeks (8 weeks = 8 mm Hegar)
8. Cannula insertion: selected Karman cannula inserted gently beyond the internal os to fundus; measure depth against sound reading
9. Create suction: lock the MVA syringe, retract plunger to create vacuum, connect to cannula
10. Evacuation: rotate cannula 180° while withdrawing slightly; aspirate with gentle in-out motion; stop when uterus grips the cannula (grittiness = stripped endometrium), foam (no tissue) enters syringe, and the uterus feels firm
11. Tissue check: empty contents of syringe into kidney dish of water; inspect for chorionic villi (fluffy, floating pink-white material), gestational sac, fetal parts at later gestations
C. Electric Vacuum Aspiration (EVA):
- Same principle as MVA but uses an electric pump instead of the hand syringe
- Preferred in many hospital settings for ease and speed
- Equivalent safety and efficacy to MVA
D. Dilatation and Evacuation (D&E, 13–20 weeks):
- Requires wider cervical dilatation (≥14–16 mm) — osmotic dilators (laminaria/Dilapan) placed the night before
- Larger-bore suction cannula + forceps (sponge forceps, Bierer forceps) to remove larger fetal parts
- Should be performed in an operating theatre under adequate anaesthesia
- Carries higher risk than first-trimester procedures
Provided image
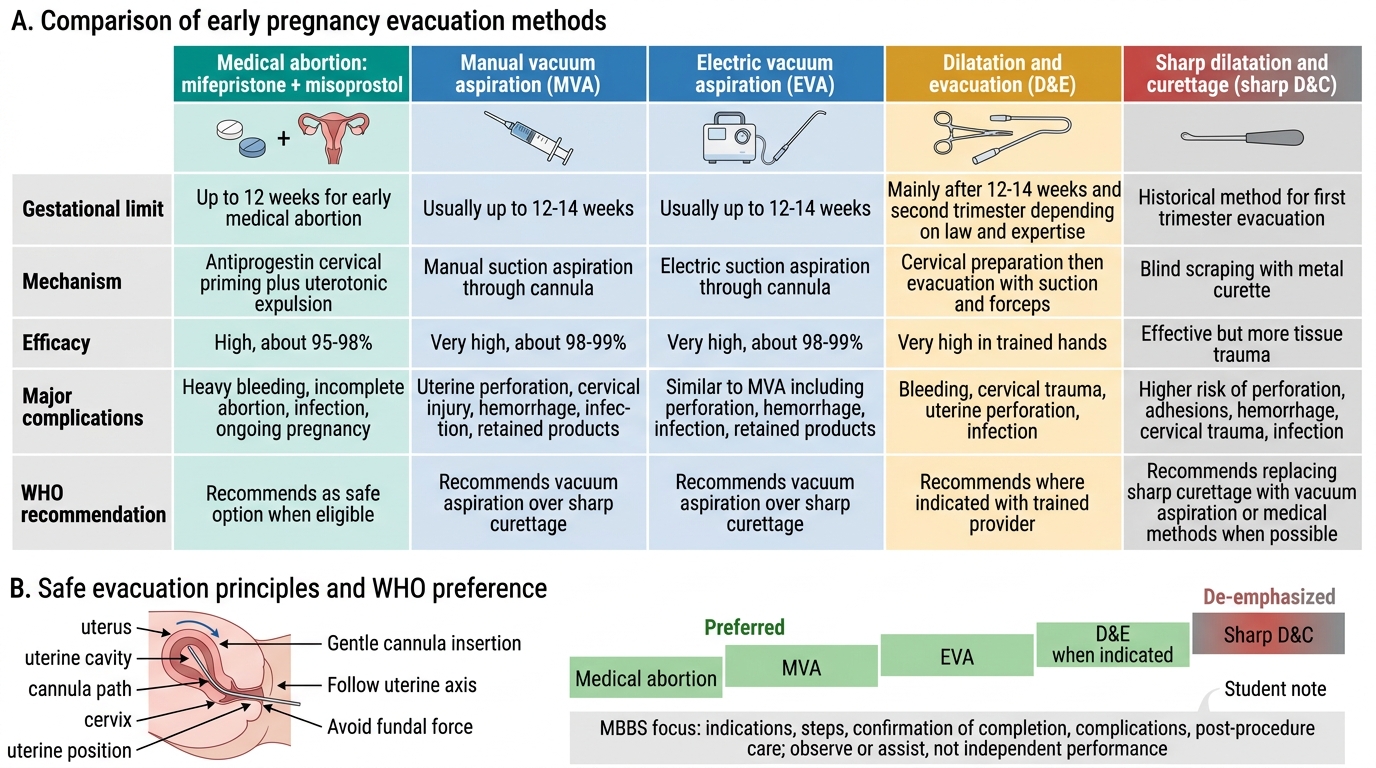
Early Pregnancy Evacuation Methods: Comparison and Safety
SELF-CHECK
During an MVA procedure at 9 weeks, after creating vacuum in the syringe, the operator notices the syringe fills with clear fluid and no tissue, and the uterus suddenly feels softer. What has most likely occurred?
A. Complete evacuation — procedure is finished
B. Uterine perforation — the cannula has exited the uterine cavity
C. Cervical stenosis — the cannula cannot pass
D. Anovaginal fistula — incorrect surgical approach
Reveal Answer
Answer: B. Uterine perforation — the cannula has exited the uterine cavity
Sudden loss of resistance, clear fluid (peritoneal fluid or serous content) in the syringe, and a 'soft' uterus that no longer grips the cannula are the hallmarks of uterine perforation. The cannula has passed through the uterine wall into the peritoneal cavity. The procedure must be stopped immediately, the patient observed for haemodynamic instability and internal bleeding, and surgical exploration considered. Complete evacuation produces a 'gritty' feel as the cannula scrapes the stripped endometrium, with foamy (no tissue) content — not clear fluid.