Page 10 of 23
OG9.4 | Ectopic Pregnancy and Acute Abdomen — SDL Guide
Learning Objectives
- Define ectopic pregnancy and describe its common sites with approximate frequency
- Describe the clinical presentation of ectopic pregnancy including the differential diagnosis of acute abdomen in early pregnancy
- Explain the pathophysiology of tubal ectopic pregnancy and the risk factors that predispose to it
- Select and interpret investigations for suspected ectopic pregnancy using the serum β-hCG/TVS algorithm
- Enumerate the strict criteria for medical management with methotrexate and contrast salpingostomy versus salpingectomy
- Outline the emergency management of a haemodynamically unstable patient with ruptured ectopic pregnancy
INSTRUCTIONS
Ectopic pregnancy is a life-threatening surgical emergency that simultaneously tests your diagnostic reasoning, your knowledge of anatomy, and your ability to act quickly under uncertainty. It is the commonest cause of maternal death in the first trimester, responsible for approximately 3–4% of all pregnancy-related deaths in India. This module takes you through the full clinical arc: from the woman presenting with vague lower abdominal pain and a positive pregnancy test, through the β-hCG/ultrasound algorithm, to the management decision between expectant waiting, methotrexate, and laparoscopic surgery. Every section builds on the last — read them in order. The known-traps section on methotrexate criteria and salpingostomy vs salpingectomy indications are high-yield viva topics.
References
- DC Dutta's Textbook of Obstetrics, 9th ed, Chapter 11 (textbook)
- Williams Obstetrics, 26th ed, Chapter 19 (textbook)
- RCOG Green-top Guideline No. 21 — Diagnosis and Management of Ectopic Pregnancy, 2016 (guideline)
- ASRM Practice Committee Opinion — Medical Treatment of Ectopic Pregnancy, 2013 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman presents to the casualty at midnight with severe right-sided lower abdominal pain, two syncopal episodes, and a positive urine pregnancy test. Her last menstrual period was 7 weeks ago. Her pulse is 118/min, blood pressure 88/56 mmHg, and on palpation she has guarding and rebound tenderness in the right iliac fossa and hypogastrium. The abdomen is soft but tender. The pelvic examination shows an adnexal mass. There is no tissue at the cervical os. What is happening, what must you do in the next 5 minutes, and what operation will she need?
WHY THIS MATTERS
Ectopic pregnancy is the leading cause of maternal death in the first trimester of pregnancy. In India, it accounts for approximately 3–4% of all pregnancy-related deaths, and the majority of these deaths are due to delayed diagnosis — the woman presents with haemorrhagic shock from a ruptured tube, having been reassured earlier that her abdominal pain was 'gastritis' because the pregnancy test was positive. Your ability to maintain a high index of suspicion for ectopic pregnancy in any woman of reproductive age with lower abdominal pain — regardless of whether she reports pregnancy symptoms — is a life-saving clinical skill. The differential diagnosis of the acute abdomen in early pregnancy is tested repeatedly in both written papers and viva examinations precisely because it requires integration of anatomy, physiology, and clinical reasoning.
RECALL
Before you begin, recall the following from earlier modules. From reproductive anatomy (OG2): the fallopian tube has four segments — interstitial (within the uterine wall), isthmic (narrow medial portion), ampullary (widest section where fertilisation occurs), and fimbrial (open end); the uterus receives blood from the uterine artery (branch of internal iliac) and the ovarian artery, both anastomosing at the cornua — this rich anastomosis is why interstitial/cornual ectopics rupture so catastrophically. From OG9.1 (investigations for abortion): the β-hCG discriminatory zone concept — when β-hCG exceeds a threshold (~1500–2000 IU/L on TVS) and no intrauterine sac is visible, ectopic must be excluded. From PID/infections: salpingitis damages the tubal epithelium and its cilia, impairing ovum transport — the mechanism by which STIs cause ectopic predisposition.
Clinical Presentation of Ectopic Pregnancy
Ectopic pregnancy is the implantation and development of the fertilised ovum at a site other than the uterine cavity. The vast majority (95–98%) occur in the fallopian tube. Every medical student memorises the classic clinical presentation, but the dangerous clinical reality is that many ectopic pregnancies do not present with the textbook triad — up to 50% of women who die from ruptured ectopic have been seen by a clinician in the preceding 24–48 hours, who missed the diagnosis because the presentation was atypical. The woman may report only mild, intermittent pain and attribute her missed period to stress. She may have no obvious vaginal bleeding. She may have seen a doctor, been reassured, and returned in extremis with haemorrhagic shock. The clinician who restricts the differential to 'threatened abortion' or 'gastritis' in any woman of reproductive age with lower abdominal pain will, statistically, miss an ectopic. Maintaining a high index of suspicion — and using the β-hCG/TVS algorithm systematically — is the only reliable protection against this diagnostic error.
The classic triad of ectopic pregnancy is:
1. Amenorrhoea — typically 6–8 weeks of absent menses (shorter if isthmic, longer if ampullary)
2. Lower abdominal/pelvic pain — often unilateral; may be vague or sudden and severe (if rupture occurs); shoulder-tip pain (diaphragmatic irritation by haemoperitoneum) is a red-flag symptom
3. Vaginal bleeding — usually scanty, dark ('old blood'); distinguishable from the heavier red bleeding of incomplete abortion (but not always reliable)
On examination:
- Vital signs: may be haemodynamically stable (unruptured) or unstable (ruptured — HR >100, SBP <90, pallor, syncope)
- Abdominal: lower abdominal tenderness; guarding and rebound if peritoneum is irritated by haemoperitoneum; shoulder-tip tenderness if significant intraperitoneal bleeding
- Pelvic examination: cervical os CLOSED (distinguishes from inevitable/incomplete abortion); cervical excitation tenderness (pain on moving the cervix — adnexal pathology = pain when tube is palpated via cervical movement); adnexal mass may be palpable
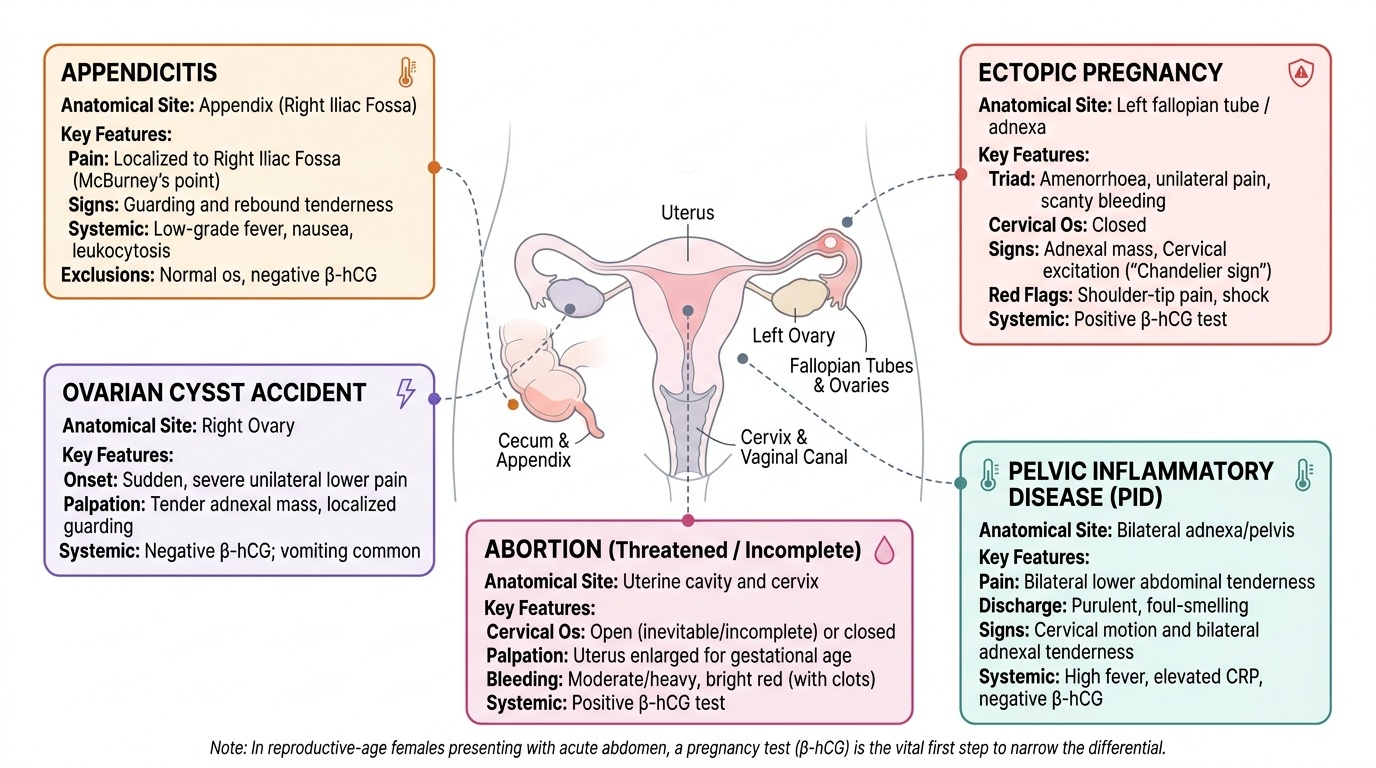
Differential diagnosis of acute abdomen in early pregnancy — this is the core clinical reasoning challenge:
- Ectopic pregnancy: closed os, adnexal mass/tenderness, cervical excitation, haemoperitoneum signs if ruptured; positive hCG
- Threatened/inevitable abortion: bleeding, uterus size = dates, open os (inevitable), USG may show live fetus or failing IUP
- Incomplete abortion: open os, tissue passed or retained, uterus smaller than dates
- Ruptured corpus luteum cyst: no intrauterine pregnancy expected; may present identically to ectopic; negative or very low hCG distinguishes
- Ovarian cyst accident (torsion or rupture): adnexal mass on USG, may be afebrile; Doppler shows absent or reduced flow in torsion
- Appendicitis: right iliac fossa tenderness at McBurney's point, Rovsing's sign, fever, raised WBC; positive pregnancy test does not exclude — appendicitis is the most dangerous non-obstetric diagnosis to miss in a pregnant woman
- Pelvic inflammatory disease (PID): bilateral adnexal tenderness, cervical discharge, fever; closed os; lower hCG level
- Degeneration in fibroid: if previous fibroids known; USG shows fibroid with heterogeneous core
Provided image
SELF-CHECK
A woman with 7 weeks amenorrhoea presents with right-sided pelvic pain and minimal dark vaginal bleeding. Pelvic examination shows cervical excitation tenderness and a right adnexal fullness. The cervical os is CLOSED. Which feature most reliably distinguishes this presentation from a threatened abortion?
A. The minimal nature of the vaginal bleeding
B. Cervical excitation tenderness and closed os with adnexal fullness
C. The 7-week period of amenorrhoea
D. Dark colour of the vaginal bleeding
Reveal Answer
Answer: B. Cervical excitation tenderness and closed os with adnexal fullness
Cervical excitation tenderness (CEP) — pain on moving the cervix, indicating adnexal pathology — combined with an adnexal mass/fullness and a closed os is the key examination finding that distinguishes ectopic from threatened abortion. In threatened abortion: the os is also closed, but uterine size matches dates, there is no adnexal mass, and there is no cervical excitation tenderness (the pathology is intrauterine). The colour and amount of bleeding are unreliable discriminators.
Pathophysiology and Sites of Ectopic Implantation
The fertilised ovum normally completes its journey from the ampulla of the fallopian tube to the uterine cavity in approximately 3 days, propelled by coordinated tubal peristalsis and the rhythmic sweeping of the mucosal cilia lining the tube. This finely timed transport is necessary for the embryo to reach the uterine endometrium — which has been prepared by the progesterone-driven secretory phase — at precisely the right developmental stage for implantation. Ectopic implantation occurs when this transport is impaired: the blastocyst is delayed, misdirected, or structurally prevented from entering the uterine cavity, and implants in the first hospitable tissue it encounters — most often the tubal mucosa. Once implanted outside the uterus, the invading trophoblast follows its programmed behaviour: it erodes blood vessels, anchors itself to the surrounding tissue, and expands — until the containing structure, whether tubal wall or uterine cornua or ovarian stroma, can no longer accommodate the growing mass and ruptures. The resulting haemorrhage can be life-threatening within minutes. The site of implantation determines the timeline to rupture and the severity of haemorrhage when it occurs.
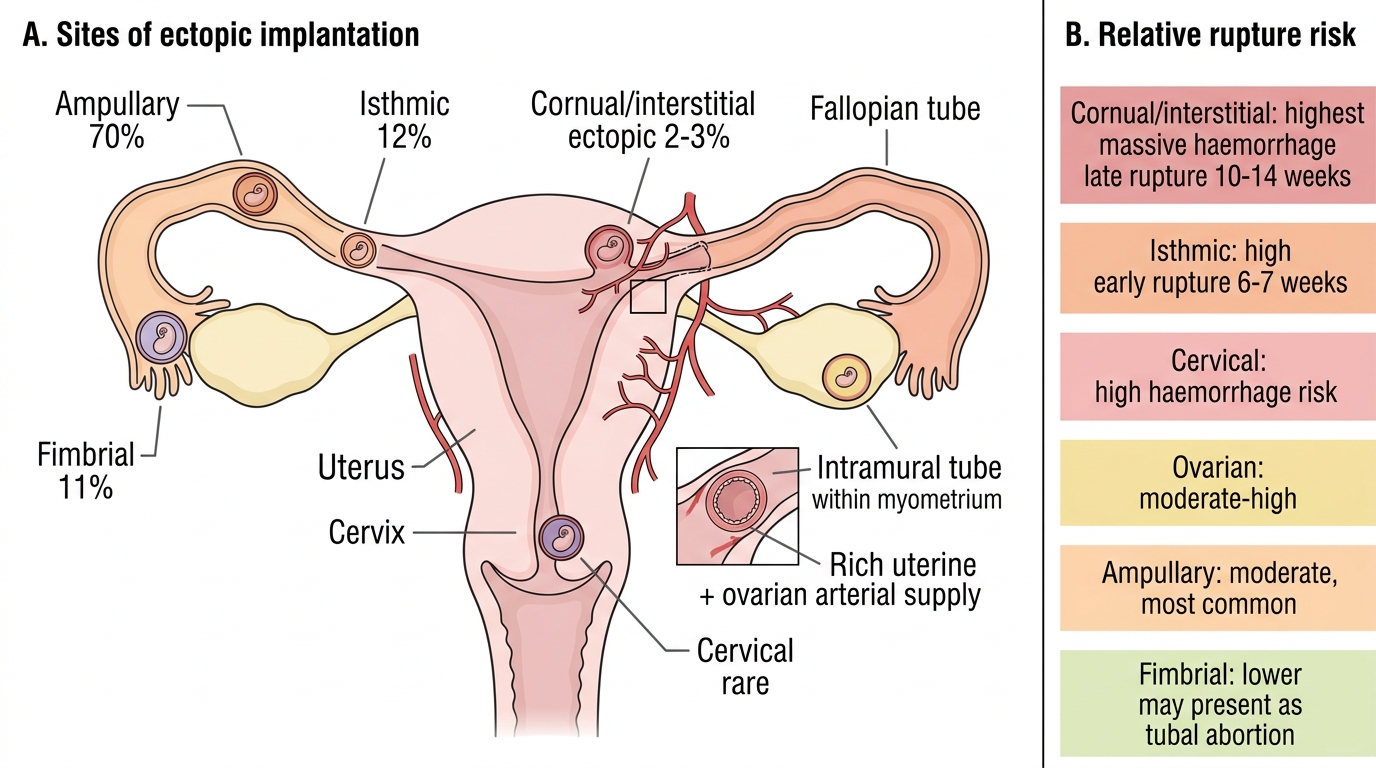
Sites of ectopic implantation and their clinical significance:
- Ampullary (~70%): the widest tubal segment; most common site; the tube accommodates the growing conceptus longest before rupture; tends to present as 'tubal abortion' (extrusion of the ectopic through the fimbrial end) rather than tubal rupture; usually presents at 6–8 weeks
- Isthmic (~12%): narrow segment; least space for growth; tends to rupture EARLY, often at 6–7 weeks, with acute haemorrhage
- Fimbrial (~11%): near the fimbrial end; may present as tubal abortion
- Cornual/interstitial (~2–3%): within the intramural segment of the tube where it enters the uterus; very small percentage but MOST DANGEROUS because it lies surrounded by the myometrium with a dual blood supply from both uterine and ovarian arteries; rupture tends to occur LATER (10–14 weeks) but produces massive haemorrhage; requires different surgical approach
- Ovarian, abdominal, cervical: rare (<5% collectively); cervical ectopics may be confused with placenta praevia; abdominal ectopics can progress to advanced abdominal pregnancy
- Heterotopic pregnancy: simultaneous intrauterine and ectopic pregnancy; rare naturally (~1 in 30,000) but significantly increased with IVF/assisted reproduction (~1 in 100 or higher); critically important — the presence of an intrauterine pregnancy does NOT exclude a simultaneous ectopic
Risk factors for ectopic pregnancy:
All risk factors share the common mechanism of impairing tubal transport or causing tubal implantation:
- Previous ectopic pregnancy (strongest risk factor — 10× risk; future ectopic risk ~10–15%)
- Previous pelvic inflammatory disease / salpingitis: Chlamydia trachomatis and Neisseria gonorrhoeae damage tubal cilia and cause peritubal adhesions — single most modifiable population-level risk factor
- Tubal surgery: salpingostomy (leaves scarring), tubal ligation (increases ectopic risk if tubes fail to remain occluded)
- Intrauterine device (IUCD): IUCD protects against intrauterine pregnancy more effectively than tubal; if pregnancy occurs despite IUCD, it is more likely to be ectopic (does NOT mean IUCD causes ectopic — overall rate is reduced)
- Assisted reproduction: ovarian hyperstimulation disrupts normal tubal physiology; multiple embryo transfer increases heterotopic risk
- Cigarette smoking: impairs tubal motility (anti-oestrogenic effect on cilia)
- Congenital tubal anomalies: diverticulae, accessory ostia
- Endometriosis: peritubal involvement affects tubal function
Sites and Rupture Risk of Ectopic Pregnancy
SELF-CHECK
Which site of ectopic pregnancy carries the highest risk of massive haemorrhage upon rupture, tends to rupture latest (at 10–14 weeks), and is most difficult to distinguish from an intrauterine pregnancy on early ultrasound?
A. Ampullary ectopic
B. Isthmic ectopic
C. Cornual/interstitial ectopic
D. Fimbrial ectopic
Reveal Answer
Answer: C. Cornual/interstitial ectopic
The cornual/interstitial ectopic implants within the intramural segment of the fallopian tube, surrounded by myometrium. It is supplied by both the uterine and ovarian arteries, giving it a richer blood supply than any other tubal site. Rupture typically occurs late (10–14 weeks) but produces massive haemorrhage. On TVS, the gestational sac appears eccentrically placed within the myometrium — easily mistaken for an intrauterine pregnancy or a cornual pregnancy in a unicornuate uterus. The isthmic ectopic ruptures earliest (6–7 weeks) but the blood supply is more limited than the cornual.
Diagnosis and Investigation
The diagnosis of ectopic pregnancy is made by integrating the clinical presentation with two objective investigations: a quantitative serum β-hCG measurement and a transvaginal ultrasound (TVS). Used together and interpreted in sequence using the discriminatory zone principle, these two investigations can confirm or exclude ectopic pregnancy in the vast majority of stable patients. This algorithm is the standard of care in all settings with access to quantitative β-hCG assay and TVS — and it is the framework you must be able to apply at the bedside and articulate in a viva. One critical exception must be stated at the outset: when a patient presents with haemodynamic instability (tachycardia, hypotension, syncope, signs of haemoperitoneum), the diagnosis is made on clinical grounds alone. A woman in shock with a positive pregnancy test and abdominal peritonism has an ectopic until proven otherwise — she goes to the operating theatre without delay, not for TVS imaging. The investigation algorithm applies only to haemodynamically STABLE patients in whom there is time for a methodical diagnostic workup.
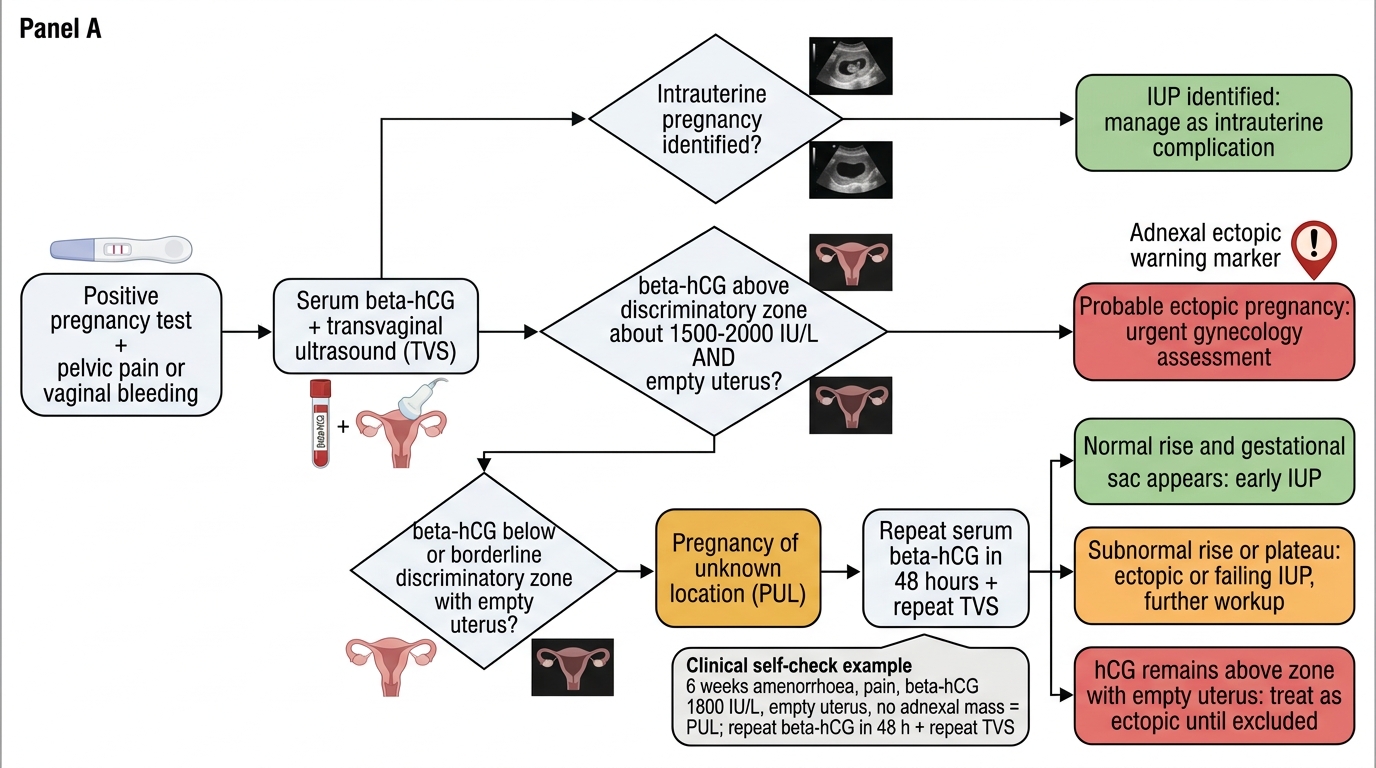
The β-hCG / TVS algorithm for haemodynamically stable patients:
Step 1 — Urine or serum β-hCG:
- Positive test confirms an active trophoblastic pregnancy (intrauterine or ectopic)
- A very high β-hCG (>100,000 IU/L) makes ectopic extremely unlikely — consider gestational trophoblastic disease
Step 2 — TVS:
- Identifies intrauterine gestational sac from ~4.5–5 weeks (TVS); yolk sac from ~5.5 weeks; fetal pole from ~6 weeks
- Finding: intrauterine sac with yolk sac/fetal pole → IUP confirmed; proceed to manage as intrauterine complication
- Finding: empty uterus + adnexal mass with echogenic ring ('tubal ring' sign) ± cardiac activity in adnexal mass → ectopic confirmed
- Finding: empty uterus, no definite adnexal mass → indeterminate; apply discriminatory zone
Step 3 — Discriminatory zone:
- The β-hCG threshold above which a TVS should always visualise an IUP: approximately 1,500–2,000 IU/L (TVS)
- β-hCG ABOVE discriminatory zone + empty uterus on TVS = presumed ectopic or failing IUP → manage accordingly
- β-hCG BELOW discriminatory zone + empty uterus = pregnancy of unknown location (PUL) — too early for TVS to confirm; repeat β-hCG in 48 hours
Step 4 — Serial β-hCG (48-hour repeat):
- Normal IUP: β-hCG rises ≥53% in 48 hours (practically 'doubles')
- Sub-optimal rise (<53% in 48 hours) → failing IUP or ectopic — requires further evaluation
- Declining β-hCG → most likely a failing pregnancy (spontaneous abortion); if declining slowly and there is no IUP on USG, ectopic still possible
- Rising β-hCG above discriminatory zone with persistently empty uterus → ectopic until proven otherwise; proceed to management
Additional investigations:
- Full blood count: haemoglobin and white cell count; eosinophilia may be present with haemoperitoneum
- Blood group and cross-match: in any haemodynamically unstable patient
- Serum progesterone: <5 ng/mL suggests non-viable pregnancy; does not distinguish site
- Posterior culdocentesis: rarely performed now (TVS has replaced it); aspiration of non-clotting blood from the pouch of Douglas confirms haemoperitoneum
- Diagnostic laparoscopy: the definitive diagnostic and therapeutic procedure when β-hCG/TVS are inconclusive and clinical suspicion remains
Diagnostic Algorithm for Suspected Ectopic Pregnancy
SELF-CHECK
A woman with 6 weeks amenorrhoea and lower abdominal pain has a serum β-hCG of 1,800 IU/L. TVS shows an empty uterine cavity with no adnexal mass. What is the correct next step?
A. Diagnose threatened abortion and send home with reassurance
B. Diagnose ectopic pregnancy and arrange immediate laparoscopy
C. Repeat serum β-hCG in 48 hours and repeat TVS; classify as pregnancy of unknown location
D. Administer methotrexate immediately without further investigation
Reveal Answer
Answer: C. Repeat serum β-hCG in 48 hours and repeat TVS; classify as pregnancy of unknown location
The β-hCG of 1800 IU/L is just above the lower end of the discriminatory zone (~1500–2000 IU/L on TVS). An empty uterus at this level is indeterminate — it could be a very early IUP just below visible threshold, a failing IUP, or an ectopic. This is a 'pregnancy of unknown location' (PUL). The correct management is serial β-hCG at 48 hours and repeat TVS: if hCG rises normally and a sac appears, it is likely an IUP; if rise is sub-optimal or hCG stays above discriminatory zone with empty uterus on repeat scan, manage as ectopic. Methotrexate without confirming the diagnosis risks treating an early viable IUP.