Page 11 of 23
OG9.4 | Ectopic Pregnancy and Acute Abdomen — SDL Guide (Part 2)
Management — Medical, Surgical, and Expectant
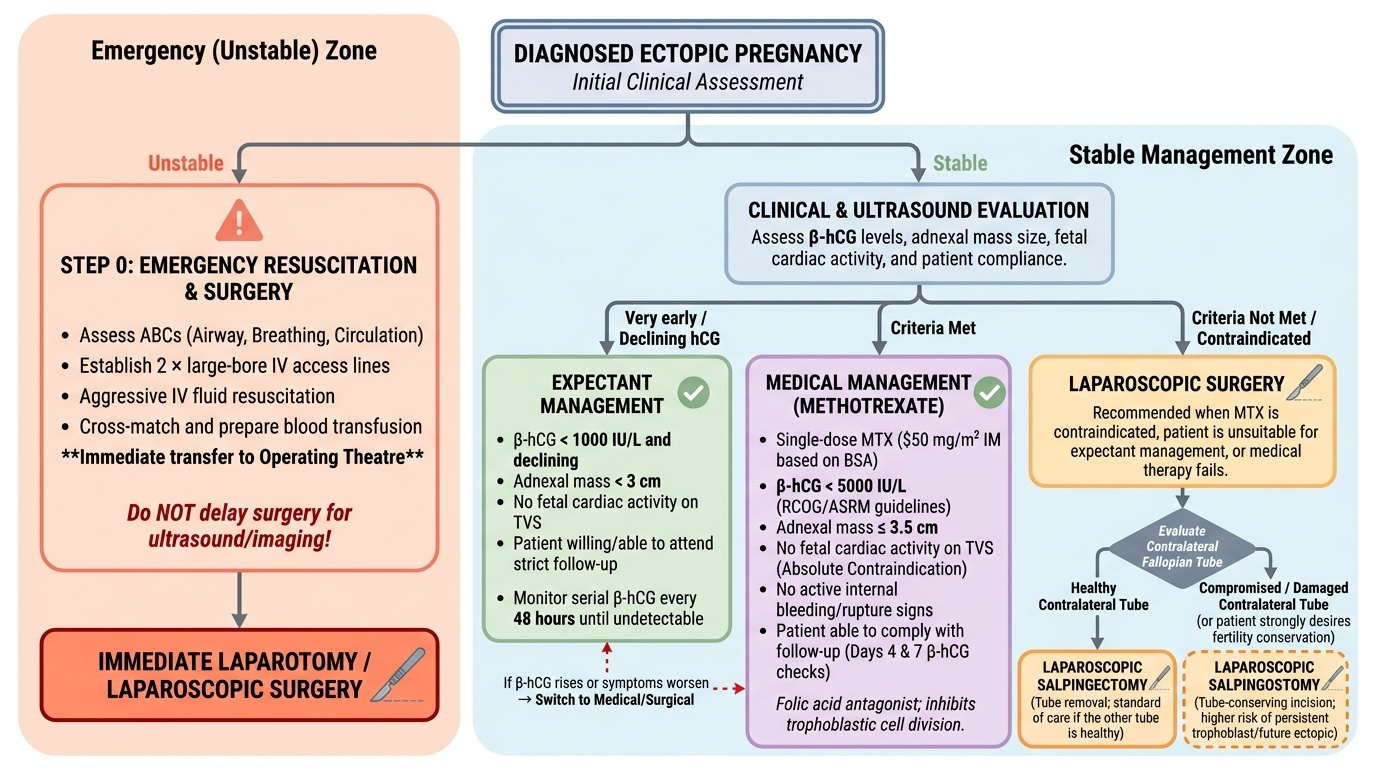
Management of ectopic pregnancy depends on two primary factors: the haemodynamic status of the patient and whether strict criteria for medical management are met. The three treatment options are: (1) expectant management (monitoring without active intervention) for very early, small, declining-hCG ectopics; (2) methotrexate (medical) for haemodynamically stable women meeting strict selection criteria; and (3) surgery (laparoscopic salpingostomy or salpingectomy) for all unstable patients and for those not meeting methotrexate criteria. The choice between salpingostomy (tube-conserving) and salpingectomy (tube removal) depends on the clinical situation and the status of the contralateral tube — this distinction is a classic viva topic and the indications must be memorised precisely.
Step 0 — Emergency resuscitation (if haemodynamically unstable):
A ruptured ectopic with haemodynamic instability is a surgical emergency — airway, breathing, circulation, IV access (two large-bore lines), aggressive IV fluids, cross-match and transfuse as needed, immediate transfer to operating theatre. Do NOT delay surgery for imaging in an unstable patient.
Expectant management:
- Appropriate only when: haemodynamically stable, β-hCG <1000 IU/L AND declining, no cardiac activity on USG, adnexal mass <3 cm, patient willing to attend for serial follow-up
- Serial β-hCG every 48 hours until undetectable
- If hCG rises or symptoms worsen → switch to methotrexate or surgery
- ~70% of carefully selected cases resolve without intervention
Medical management — Methotrexate (MTX):
MTX is a folic acid antagonist that inhibits rapidly dividing cells (trophoblast); kills the ectopic tissue, allowing natural resorption.
Strict inclusion criteria for single-dose MTX (50 mg/m² IM — calculated from body surface area):
- Haemodynamically STABLE (no signs of rupture or active haemorrhage)
- β-hCG level <5000 IU/L (most guidelines; ASRM and RCOG; success rate falls sharply above this level)
- No cardiac activity on TVS (cardiac activity is an absolute contraindication — fetal heart suggests advanced trophoblast; MTX success rate drops to <25%)
- Adnexal mass ≤3.5 cm (larger masses have higher rupture risk during treatment)
- Ability to comply with follow-up (β-hCG monitoring days 4 and 7 after injection)
Absolute contraindications to MTX:
- Haemodynamic instability / ruptured ectopic
- β-hCG showing cardiac activity
- Breastfeeding
- Significant liver disease, renal failure, blood dyscrasia, immunodeficiency
- Allergy to methotrexate
- Patient unable to comply with follow-up
Post-MTX protocol:
- Day 4 β-hCG: may transiently rise (acceptable — MTX causes trophoblast lysis that releases hCG)
- Day 7 β-hCG: MUST decline ≥15% from Day 4 value
- If <15% decline by Day 7: administer second dose of MTX OR proceed to surgery
- Advise: avoid folic acid supplementation (antagonises MTX), avoid NSAIDs, avoid intercourse, use contraception for 3 months (MTX is teratogenic)
- Monitor until β-hCG undetectable
Surgical management:
Laparoscopy is the preferred surgical approach (over laparotomy) unless the patient is haemodynamically unstable and laparoscopic equipment or expertise is unavailable.
Two options:
- Salpingostomy (linear incision over the ectopic, removal of products, tube left in place):
- Preferred when: the contralateral (other) tube is absent or damaged (to preserve future fertility through this tube)
- Risk: persistent trophoblast in ~5–8% of cases (requires MTX); incomplete removal; future ectopic risk in the same tube
- ESEP trial showed similar cumulative live birth rates for salpingostomy vs salpingectomy at 3 years when contralateral tube is normal
- Salpingectomy (removal of the entire affected tube):
- Preferred when: the contralateral tube is NORMAL and healthy (salpingectomy does not reduce fertility if the other tube is intact)
- Mandatory when: ruptured ectopic with uncontrolled haemorrhage; recurrent ectopic in the same tube; cornual/interstitial ectopic (requires cornual resection ± hysterectomy in severe cases); severely damaged tube
- Eliminates risk of persistent trophoblast and future ectopic in that tube
Post-operative care:
- Blood transfusion as indicated
- Anti-D immunoglobulin for all Rh-negative women: 300 µg IM (ectopic is ≥12 weeks equivalent risk even if earlier) — use the 300 µg dose to be safe
- Serial β-hCG post-salpingostomy until undetectable
- Contraceptive counselling: avoid pregnancy for ≥3 months
Provided image
CLINICAL PEARL
The two most dangerous clinical errors in ectopic pregnancy are: (1) Assuming the diagnosis is 'threatened abortion' because the os is closed and there is a positive pregnancy test — always exclude ectopic FIRST in any woman with first-trimester pain and bleeding, particularly if there is adnexal tenderness, cervical excitation, or if β-hCG is above the discriminatory zone without an intrauterine sac on TVS. The closed os does NOT confirm intrauterine pregnancy. (2) Giving methotrexate to a woman with cardiac activity in the adnexal mass — MTX has a very low success rate in the presence of fetal cardiac activity, and delay while waiting for MTX to work exposes the patient to the risk of rupture during the treatment window. Cardiac activity on USG in an adnexal mass is an absolute indication for surgery, not MTX.
Self-Assessment
Use these questions to consolidate your learning before your viva examination. Ectopic pregnancy is a classic viva topic because it requires integration across multiple domains: anatomy (tubal sites and their significance), pathophysiology (risk factors and mechanisms), investigations (β-hCG algorithm and discriminatory zone), and management (methotrexate criteria, salpingostomy versus salpingectomy). Examiners frequently present clinical scenarios and ask you to reason through to a management decision — you must be able to state not only what you would do but why, citing the specific clinical parameters that guide the choice between expectant, medical, and surgical management. Pay particular attention to the salpingostomy-versus-salpingectomy question: the answer depends entirely on the status of the contralateral tube, and getting this wrong in a viva signals a fundamental misunderstanding of reproductive surgery principles.
- Define ectopic pregnancy. List the six sites in order of frequency.
- Name five risk factors for ectopic pregnancy and explain the mechanism by which each predisposes to ectopic implantation.
- What is the 'discriminatory zone' and how does it guide the management of a woman with lower abdominal pain, a positive pregnancy test, and an empty uterus on TVS?
- A woman with a suspected unruptured ectopic has β-hCG of 3,200 IU/L, a 2.5 cm adnexal mass with no cardiac activity, and is haemodynamically stable. Is she a candidate for methotrexate? Justify your answer.
- What are the absolute contraindications to methotrexate treatment for ectopic pregnancy?
- In a laparoscopic procedure for ectopic pregnancy, when would you perform salpingostomy versus salpingectomy? What does the ESEP trial tell us about reproductive outcomes?
SELF-CHECK
A 30-year-old woman has a right-sided ectopic pregnancy with β-hCG of 4,200 IU/L, a 2.8 cm right adnexal mass, no cardiac activity, and is haemodynamically stable. She had her left salpingectomy 2 years ago for a previous ectopic. Which management is most appropriate?
A. Methotrexate 50 mg/m² IM — she meets all criteria
B. Laparoscopic right salpingectomy — remove the affected tube
C. Laparoscopic right salpingostomy — preserve the tube as it is her only remaining tube
D. Expectant management — β-hCG is below 5000 IU/L
Reveal Answer
Answer: C. Laparoscopic right salpingostomy — preserve the tube as it is her only remaining tube
This woman has only ONE remaining fallopian tube (left tube removed previously). Although she technically meets methotrexate criteria (stable, hCG <5000, no cardiac activity, mass <3.5 cm), the surgical decision if MTX fails or if surgery is needed is critically important: salpingectomy of her only remaining tube would leave her without tubal fertility. Therefore, if surgery is required, RIGHT SALPINGOSTOMY (tube-conserving) is preferred to preserve the only functional tube — even though the ESEP trial showed equivalent fertility rates for salpingostomy vs salpingectomy when the contralateral tube is NORMAL. In this case the contralateral tube is ABSENT, making salpingostomy the correct surgical choice. MTX remains an appropriate option here too, but if the examiner asks which SURGICAL approach — salpingostomy is correct.