Page 13 of 23
OG9.5 | Gestational Trophoblastic Neoplasia — SDL Guide
Learning Objectives
- Describe the clinical features of complete and partial hydatidiform mole and recognise the acute early-pregnancy presentation of gestational trophoblastic neoplasia
- Explain the pathophysiology of trophoblastic proliferation, the role of β-hCG excess, and the downstream complications (theca-lutein cysts, hyperemesis, early-onset pre-eclampsia, hyperthyroidism)
- Interpret the investigations for molar pregnancy, including the snowstorm ultrasound appearance and quantitative β-hCG, and construct a differential diagnosis
- Outline the principles of initial management including suction evacuation, peri-operative care, histopathological examination, and anti-D prophylaxis
- Apply the post-molar β-hCG surveillance protocol, recognise plateau and rising β-hCG as the trigger for GTN referral, and cross-reference oncologic staging and chemotherapy to OG34.3
INSTRUCTIONS
Gestational trophoblastic neoplasia (GTN) is a spectrum of abnormal trophoblastic proliferation that uniquely arises from placental tissue. Although malignant transformation is uncommon, the acute early-pregnancy presentation — a woman in the first or second trimester with disproportionate uterine enlargement, passage of vesicular tissue, and a dramatically elevated serum β-hCG — demands rapid recognition and decisive management. The clinician's role at this stage is diagnosis, suction evacuation, and careful post-molar surveillance; the critical skill is knowing when the β-hCG trajectory mandates escalation to a trophoblastic disease centre for oncologic care. This module focuses on that first clinical encounter and the bridge to oncologic management. Oncologic staging (FIGO 2002), the WHO prognostic scoring system, and chemotherapy regimens are covered in OG34.3.
References
- DC Dutta's Textbook of Obstetrics, 10th ed., Ch. 14 — Gestational Trophoblastic Neoplasia (textbook)
- Williams Obstetrics, 26th ed., Ch. 20 — Gestational Trophoblastic Disease (textbook)
- RCOG Green-top Guideline 38 (2020) — The Management of Gestational Trophoblastic Disease (guideline)
- FIGO 2002 Staging and Classification of GTN (for oncologic follow-up, see OG34.3) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 26-year-old woman presents at 14 weeks gestation with moderate vaginal bleeding and passage of grape-like vesicles. Her uterus feels 20 weeks in size. She reports severe vomiting since 8 weeks and two blood pressure readings above 140/90 in the past week — strikingly early for pre-eclampsia. Her serum β-hCG is reported at 380,000 mIU/mL. The ultrasound report reads: 'echogenic heterogeneous uterine mass with multiple anechoic cystic spaces; no fetal pole identified.' What are you dealing with, and what must you do in the next two hours?
WHY THIS MATTERS
Gestational trophoblastic disease (GTD) is one of the few human malignancies that is almost always curable, but only when recognised and followed up correctly. South-East Asia has the world's highest incidence — approximately 1–2 per 1,000 pregnancies in India — so you will encounter this in practice. The initial encounter is not the haematology-oncology clinic: it is you, in a district hospital or emergency assessment unit, confronted with a woman bleeding in the first or second trimester, a grossly elevated β-hCG, and an ultrasound that does not show a normal pregnancy. Recognising the molar pattern, performing or arranging a safe suction evacuation, sending tissue for histology, and initiating a rigorous β-hCG surveillance protocol — these are the tasks that determine whether malignant transformation is caught early, when cure rates approach 100%, or missed until metastatic disease is established.
RECALL
Before proceeding, consolidate two prior knowledge anchors. First, human chorionic gonadotrophin (hCG) is produced by syncytiotrophoblast; in normal pregnancy it peaks at around 8–10 weeks (typically 100,000–200,000 mIU/mL) then falls. It is the basis of all pregnancy tests. Second, from your embryology and maternal-physiology blocks: the trophoblast differentiates into cytotrophoblast and syncytiotrophoblast and invades the decidua to establish placentation. Uncontrolled trophoblastic proliferation — the hallmark of molar disease — amplifies this invasive potential and drives β-hCG to levels far above a normal pregnancy. Third, recall the early complications of pregnancy covered in this cluster (OG9.1–9.4): vaginal bleeding in early pregnancy has a broad differential including threatened abortion, ectopic pregnancy, and — now — molar pregnancy. Each has characteristic ultrasound and β-hCG patterns that distinguish it.
Clinical Presentation of Molar Pregnancy
The gestational trophoblastic disease (GTD) spectrum runs from the completely benign (an incidentally found partial mole on histology) to the acutely life-threatening (a haemorrhaging complete mole). Most clinically significant presentations involve complete hydatidiform mole (CHM), and this is the form the clinician must be able to recognise promptly.
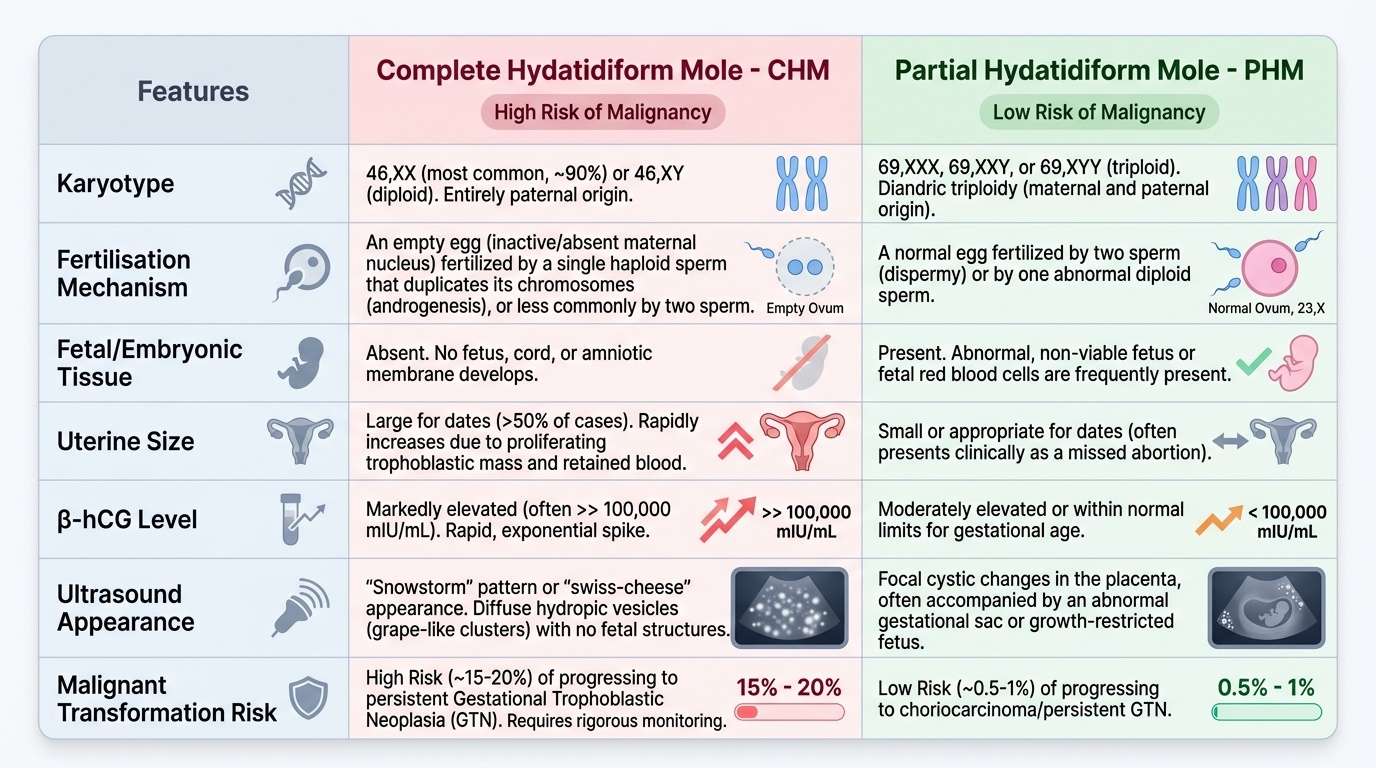
The classic presentation of a complete mole is a woman in the first trimester — most commonly between 8 and 16 weeks — with vaginal bleeding, often moderate to heavy. The bleeding is dark and continuous, occasionally accompanied by passage of grape-like vesicles (hydatid vesicles), which are pathognomonic when seen. The uterus is almost always large-for-dates — typically two or more weeks ahead of the gestational size — because of the proliferating trophoblastic mass. Alongside this, the patient frequently presents with hyperemesis gravidarum out of proportion to her gestation, driven by β-hCG excess stimulating the vomiting centre. Two other features are particularly important in the Indian context because they mislead the clinician: early-onset pregnancy-induced hypertension (before 20 weeks, which is virtually never pre-eclampsia in a normal pregnancy) and bilateral ovarian cysts felt on examination (theca-lutein cysts).
A partial hydatidiform mole (PHM) presents more subtly. The fetus is often present (albeit abnormal), the uterus may be small or appropriate for dates, and β-hCG is only moderately elevated. PHM is frequently diagnosed only on histology following a curettage for missed or incomplete abortion. The clinical picture rarely includes the dramatic features of CHM. Recognising the distinction matters because CHM carries a ~15–20% risk of persisting GTN requiring treatment, whereas PHM carries ~0.5–1% risk.
IMPORTANT: absent from the classic teaching but now well-recognised is the 'silent' molar pregnancy — an early mole evacuated before the classical triad develops, diagnosed entirely on ultrasound and β-hCG. Early booking ultrasound in the first trimester has made this the more common contemporary presentation.
Provided image
Pathophysiology: Trophoblastic Proliferation and β-hCG Excess
Understanding how a mole arises from an abnormal fertilisation event explains both its clinical features and its potential for malignant transformation.
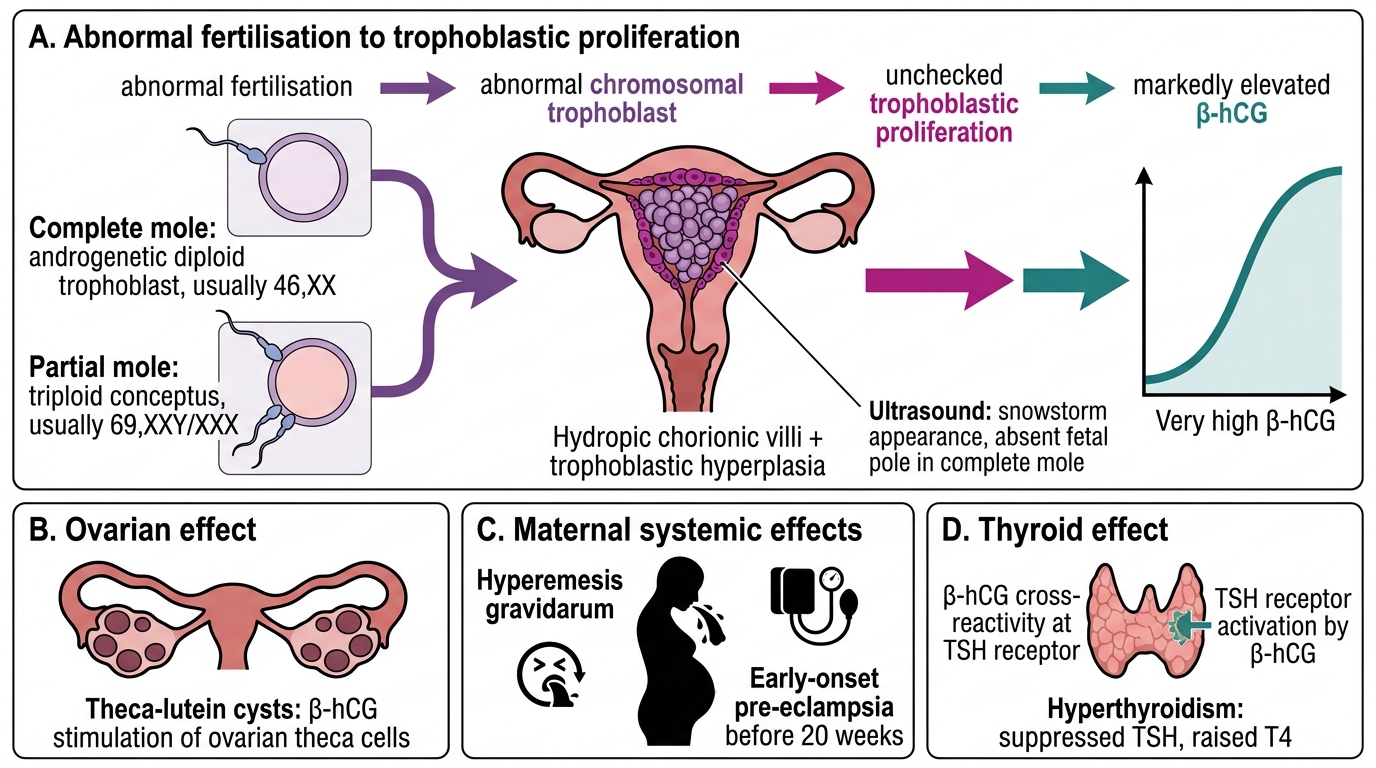
Complete hydatidiform mole arises when an ovum lacking its maternal chromosomes (an empty ovum) is fertilised — most commonly by a single sperm that then duplicates its chromosomes (androgenetic dispermy), yielding a 46,XX karyotype entirely of paternal origin. Less commonly, two sperms fertilise the empty ovum (dispermy), giving 46,XX or 46,XY. Because there is no maternal nuclear DNA, fetal development is impossible. The result is a uterus filled with grossly hydropic (oedematous), avascular chorionic villi intermixed with markedly proliferating trophoblast — the source of the grape-like vesicles and the driver of massive β-hCG secretion.
Partial hydatidiform mole arises from triploidisation — a normal ovum fertilised by two sperms (dispermia) or by a single diploid sperm, giving 69,XXX or 69,XXY. Maternal chromosomes are present; limited fetal development occurs, though the embryo is severely abnormal.
The downstream consequences of very high β-hCG account for most of the distinctive clinical features. β-hCG shares structural similarity with TSH (both are heterodimeric glycoprotein hormones): at very high concentrations, β-hCG cross-reacts with TSH receptors, causing biochemical hyperthyroidism (elevated free T4, suppressed TSH) and occasional thyroid storm. It stimulates ovarian theca cells heavily, producing bilateral theca-lutein cysts (also called hyperreactio luteinalis) — which regress after evacuation. It amplifies the normal first-trimester nausea, causing intractable hyperemesis. And it appears to contribute to endothelial dysfunction, producing pregnancy-induced hypertension before 20 weeks — a presentation that should always raise the index of suspicion for molar pregnancy.
The same trophoblastic proliferative drive that causes these clinical features underlies the risk of malignant transformation. If trophoblastic cells with their inherent invasive potential persist after evacuation — whether as an invasive mole (locally penetrating myometrium) or as choriocarcinoma (fully malignant, no villi, haematogenous spread) — they continue to secrete β-hCG. This is why falling β-hCG after evacuation is the surrogate of resolution, and a plateau or rise mandates treatment.
Pathophysiology of Molar Pregnancy
SELF-CHECK
A 24-year-old woman at 12 weeks gestation has vaginal bleeding, a uterus of 18 weeks size, β-hCG of 450,000 mIU/mL, and bilateral 6 cm ovarian cysts on ultrasound. Which single investigation is most likely to confirm the diagnosis?
A. Serum AFP and LDH for germ-cell tumour
B. Pelvic ultrasound looking for snowstorm appearance and absent fetal pole
C. Urine pregnancy test strip
D. Serum TSH to exclude thyrotoxicosis as the primary diagnosis
Reveal Answer
Answer: B. Pelvic ultrasound looking for snowstorm appearance and absent fetal pole
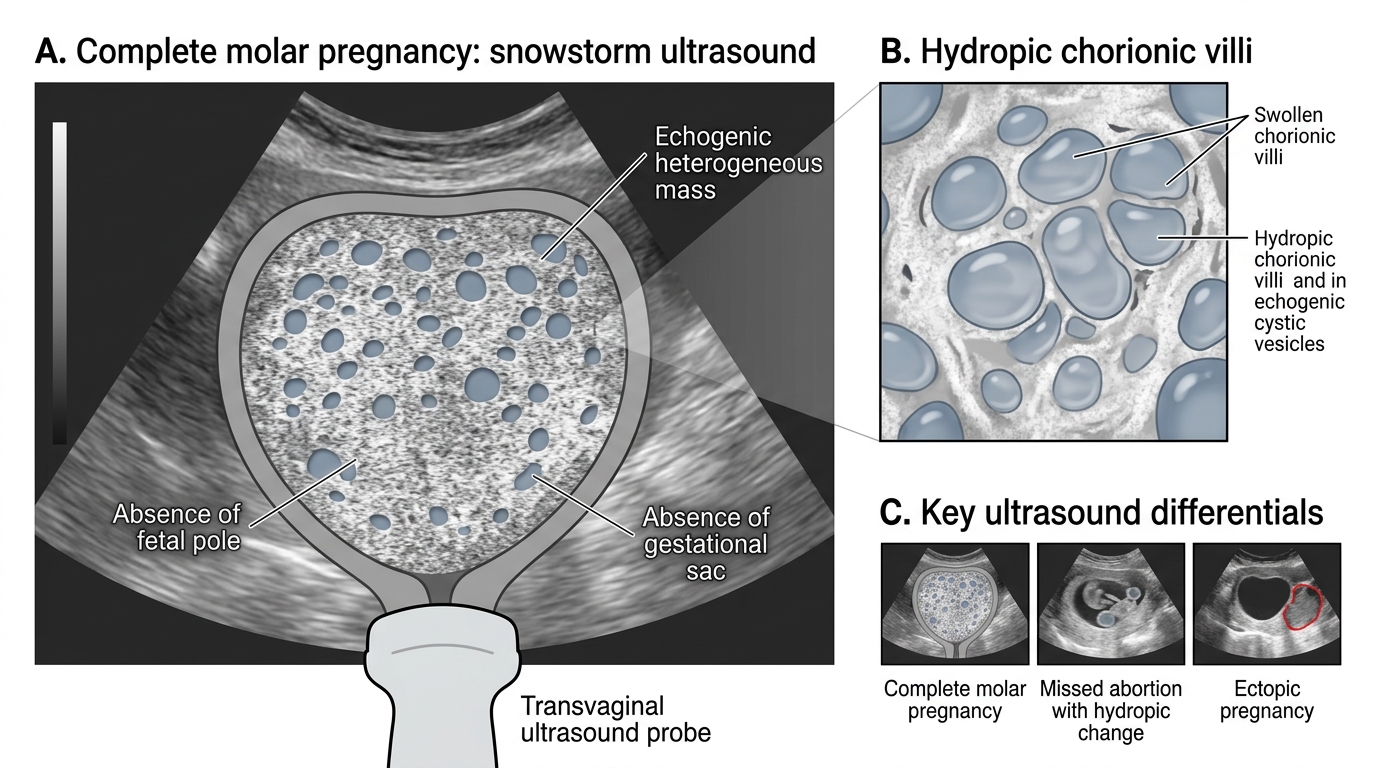
Pelvic ultrasound is the single most diagnostic investigation. In complete molar pregnancy the uterine cavity shows the characteristic 'snowstorm' pattern — a heterogeneous echogenic mass with multiple small anechoic cystic spaces replacing the chorionic villi — with no identifiable fetal pole or gestational sac. The β-hCG is already very high (consistent with molar pregnancy) and the bilateral ovarian cysts are theca-lutein cysts. TSH suppression may be found secondary to β-hCG cross-reactivity but is not the confirming test. AFP and LDH are germ-cell markers, not indicated here. The urine pregnancy test is qualitative and would be positive but not diagnostic.
Investigations: Ultrasound, β-hCG, and Differential Diagnosis
Three investigations establish the diagnosis and guide pre-operative risk assessment: ultrasound, quantitative serum β-hCG, and chest X-ray.
Pelvic ultrasound is the cornerstone. In a complete mole, the uterine cavity is occupied by an echogenic heterogeneous mass studded with multiple small, irregular anechoic cystic spaces corresponding to the hydropic chorionic villi — the classic 'snowstorm' or 'Swiss-cheese' pattern. There is no fetal pole, no gestational sac, and no amniotic fluid. Bilateral multicystic ovarian enlargement (theca-lutein cysts) may be visible. In a partial mole, the ultrasound may show a small fetus with severe anomalies, a ratio of transverse to AP diameter of the gestational sac >1.5, and focal cystic areas within an abnormal placenta. This pattern is less specific and more easily confused with a missed abortion with hydropic degeneration.
Quantitative serum β-hCG must be measured before evacuation. In complete molar pregnancy, values typically exceed 100,000 mIU/mL and may exceed one million mIU/mL — far above the normal first-trimester peak. This figure is the baseline from which post-evacuation decline is measured. A single quantitative value cannot diagnose GTN; serial values are needed post-evacuation.
Chest X-ray is mandatory before evacuation to detect pulmonary metastases ('cannon-ball' lesions), which can occur even with what appears to be uncomplicated molar disease. Pulmonary involvement alters the risk stratification at the time of GTN assessment.
Baseline haematology, renal function, liver function tests, and thyroid function (free T4 and TSH) are obtained to screen for anaemia from haemorrhage, thyroid storm risk, and comorbidity.
Differential diagnosis of a first-trimester uterus filled with heterogeneous echoes and elevated β-hCG must include: missed abortion with hydropic placental change (β-hCG appropriate for dates, ultrasound shows recognisable fetal parts though non-viable), multiple pregnancy (two or more gestational sacs with fetal poles, no cystic villi), and — very rarely — a primary ovarian or uterine choriocarcinoma (no prior molar pregnancy on history, different age distribution). The diagnosis of molar pregnancy is confirmed histopathologically on the evacuated tissue.
Complete Molar Pregnancy: Snowstorm Ultrasound Appearance
| Feature | Molar Pregnancy (Complete) | Missed Abortion with Hydropic Change | Ectopic Pregnancy |
|---|---|---|---|
| β-hCG | Markedly elevated (often >100,000) | Appropriately elevated or falling | Variable; may be low |
| Uterus size | Large for dates | Small or appropriate | Small or normal |
| Ultrasound | Snowstorm; no fetal pole | Non-viable fetal parts; less cystic | Adnexal mass; empty uterus |
| Ovaries | Theca-lutein cysts | Normal | Possible blood in pouch of Douglas |
| Vesicle passage | Yes (grape-like) | No | No |
SELF-CHECK
A woman with confirmed molar pregnancy has a chest X-ray showing two rounded opacities in the left lower lobe before suction evacuation. What is the significance of this finding?
A. It is a contraindication to suction evacuation and requires immediate chemotherapy
B. It indicates pulmonary metastases and changes risk stratification if GTN develops post-evacuation
C. It suggests co-existing pulmonary tuberculosis and requires anti-tubercular therapy first
D. It has no management significance and the report should be reviewed after evacuation
Reveal Answer
Answer: B. It indicates pulmonary metastases and changes risk stratification if GTN develops post-evacuation
Pulmonary metastases ('cannon-ball' lesions on CXR) may be present even before formal GTN is diagnosed. Their presence is not a contraindication to suction evacuation — the mole still needs to be removed. However, this finding is incorporated into the post-evacuation FIGO/WHO risk scoring (covered in OG34.3): pre-evacuation pulmonary lesions increase the score and may shift the patient from low-risk to high-risk GTN if β-hCG subsequently plateaus or rises. Recognising this on the pre-evacuation CXR ensures appropriate counselling and follow-up intensity.