Page 14 of 23
OG9.5 | Gestational Trophoblastic Neoplasia — SDL Guide (Part 2)
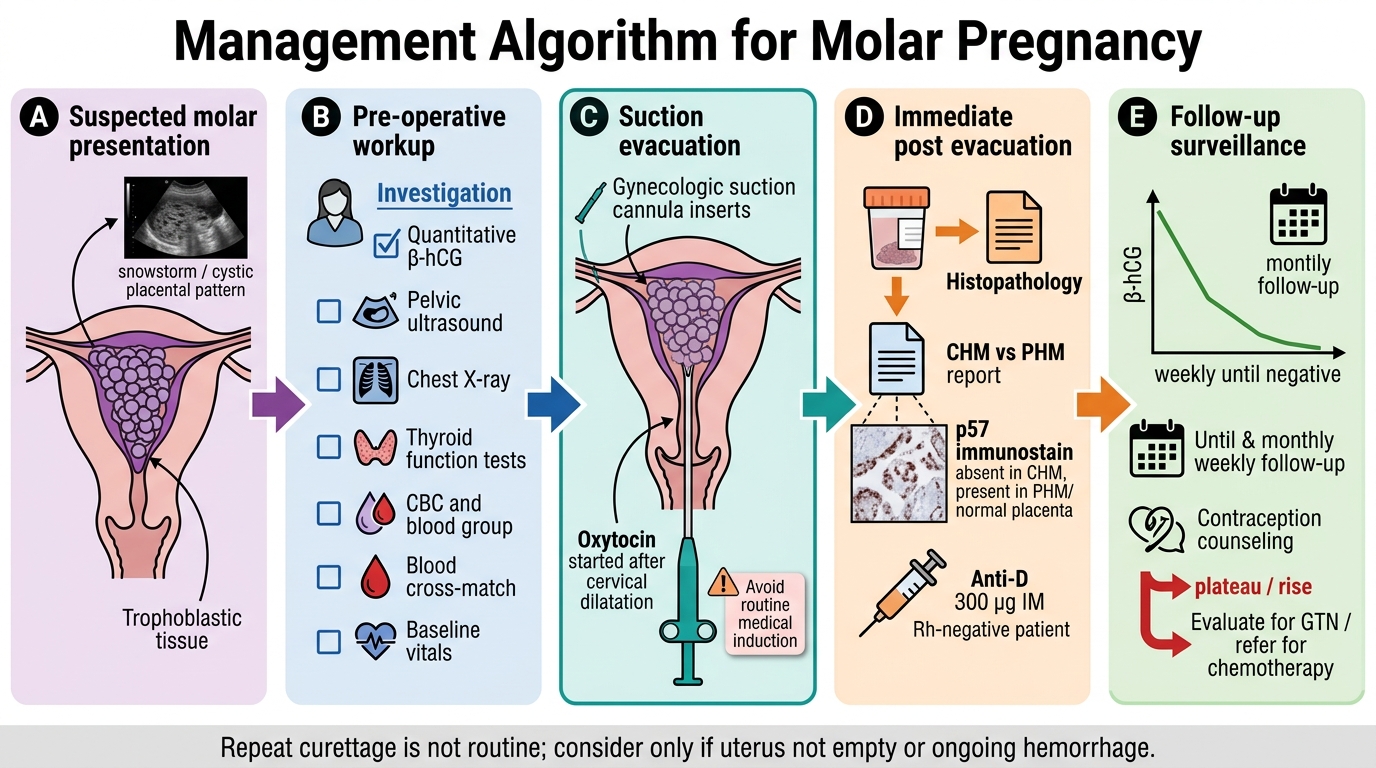
Initial Management: Suction Evacuation and Peri-operative Care
Once the diagnosis of molar pregnancy is made — clinically suspected on ultrasound and β-hCG, and almost always confirmed — the primary intervention is suction curettage (vacuum aspiration). The fundamental principle is that the uterus must be emptied efficiently, the specimen sent for histopathological confirmation, and the patient prepared for rigorous post-evacuation follow-up.
Pre-operative preparation includes: cross-match and blood availability (haemorrhage risk is significant), correction of anaemia, assessment and management of thyroid status (thyroid storm is a life-threatening peri-operative risk if free T4 is elevated — beta-blockade with propranolol and liaison with an endocrinologist is prudent before proceeding), and a review of the chest X-ray finding. Coagulation studies are obtained because molar tissue releases thromboplastin and may cause consumptive coagulopathy.
Suction curettage is the method of choice, performed under general or spinal anaesthesia. Sharp (conventional) curettage is avoided — the soft, vascular molar tissue is friable and the uterine wall thinned by trophoblastic invasion, making perforation a real risk. The cervix is dilated carefully, and a large-bore suction cannula (12–14 Fr) is used. The entire uterine contents are aspirated. Oxytocin infusion is begun after cervical dilatation (not before, to avoid forcing trophoblastic cells into the circulation before the cavity is opened) and continued for several hours post-operatively to reduce haemorrhage and the risk of trophoblastic embolism.
Stepwise Management of Molar Pregnancy
All evacuated tissue is sent for histopathology — this is non-negotiable. The pathologist's classification of CHM versus PHM, the presence of atypia, and (in referral settings) immunohistochemical markers (p57 — expressed in PHM/normal placenta, absent in CHM) determine the diagnosis and the surveillance intensity required.
Anti-D immunoglobulin (300 µg IM) is given to all Rh-negative women after suction evacuation, as fetal red cells may be present in partial moles.
Repeat curettage is NOT routine (it does not reduce GTN incidence and increases the risk of intrauterine adhesions), but is sometimes performed if the uterus is not clearly empty on post-evacuation ultrasound or if haemorrhage is ongoing. The patient and family must be counselled about the diagnosis, the probability of a normal subsequent pregnancy after surveillance, and — critically — the post-evacuation β-hCG protocol that determines whether she will need further treatment.
SELF-CHECK
Why is oxytocin started AFTER cervical dilatation rather than before suction evacuation in the management of molar pregnancy?
A. Oxytocin causes severe uterine contractions that make it impossible to dilate the cervix
B. Starting oxytocin before evacuation risks forcing trophoblastic cells into the systemic circulation, increasing the risk of trophoblastic pulmonary embolism
C. Oxytocin is contraindicated in molar pregnancy and is used only to manage post-operative haemorrhage
D. The cervix must be fully dilated before oxytocin will have any uterotonic effect
Reveal Answer
Answer: B. Starting oxytocin before evacuation risks forcing trophoblastic cells into the systemic circulation, increasing the risk of trophoblastic pulmonary embolism
The greatest theoretical risk of pre-evacuation oxytocin is causing uterine contractions that squeeze trophoblastic cells into the venous sinuses and pelvic veins before the cavity is open — increasing the risk of trophoblastic pulmonary embolism, which can be fatal. Starting the infusion after the cervix is dilated (and the suction cannula placed, allowing the cavity to decompress as it empties) minimises this risk while still providing uterotonic protection against haemorrhage during and after evacuation.
Post-Molar Surveillance: β-hCG Follow-up and the GTN Referral Trigger
After successful suction evacuation, the most important element of management is structured β-hCG surveillance. This surveillance is the bridge between the acute obstetric presentation and the potential need for oncologic treatment — and it is the clinician's primary responsibility to initiate and maintain it. No other investigation substitutes for the serial quantitative serum β-hCG assay during this period, and no aspect of care more directly determines whether a malignant transformation is caught at its earliest, most curable stage or missed until systemic spread has occurred.
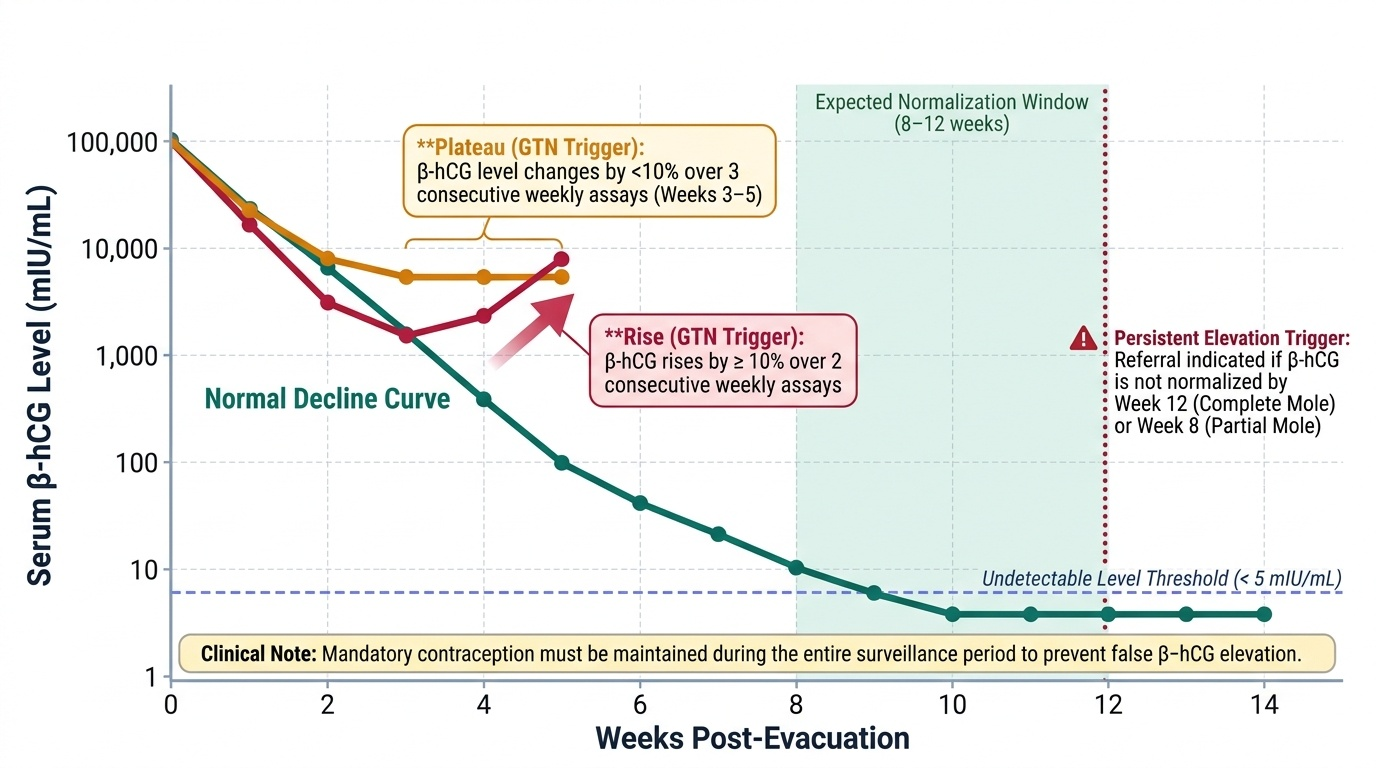
The physiological expectation after a successful and complete suction evacuation is a steady decline in circulating β-hCG levels. Because molar trophoblast is the sole source of the hormone, its progressive disappearance from the serum mirrors the elimination of residual trophoblastic activity. In a complete mole, β-hCG typically reaches undetectable levels (below 5 mIU/mL) by approximately 8 to 12 weeks after evacuation. After a partial mole — which carries substantially lower malignant potential — normalisation usually occurs more rapidly. Any deviation from this expected decline pattern is the signal for escalation. The surveillance protocol (RCOG Green-top Guideline 38, 2020, adopted in principle by Indian trophoblastic disease centres) is:
- Weekly serum β-hCG until two consecutive undetectable levels are obtained.
- Once undetectable: monthly β-hCG for a further 6 months (for complete mole) or until undetectable for two weeks (partial mole, lower risk).
Two patterns of β-hCG behaviour after evacuation are diagnostic of gestational trophoblastic neoplasia (GTN) and mandate referral to a trophoblastic disease centre:
1. Plateau: a β-hCG level that neither falls by >10% nor rises by >10% over three consecutive weekly assays.
2. Rise: β-hCG rises by >10% over two consecutive weekly assays at any point post-evacuation.
3. Additionally: β-hCG that has not normalised by 8 weeks (for partial mole) or 12 weeks (for complete mole) post-evacuation may trigger referral even without a strict plateau or rise, depending on the centre's protocol.
Contraception during surveillance is mandatory — a new pregnancy will elevate β-hCG independently and make surveillance uninterpretable. The oral contraceptive pill is safe and effective (there is no evidence it increases GTN risk). Intrauterine devices are avoided until β-hCG is undetectable (risk of perforation with residual disease). Women can be reassured that a subsequent pregnancy after completing surveillance carries no increased risk of molar recurrence compared with the general population, and that fertility is preserved.
When to refer: any plateau or rise meeting the criteria above, any evidence of metastatic disease (haemoptysis, neurological symptoms, hepatic mass), or a histology report showing invasive or atypical trophoblast should prompt immediate referral to a designated trophoblastic disease centre or oncology unit. At that point, FIGO staging and WHO prognostic scoring system are applied — as detailed in OG34.3 (og16-gtd) — and chemotherapy decisions (methotrexate for low-risk, EMA/CO for high-risk) are made by the oncology team. The clinician presenting the case should not initiate chemotherapy without formal risk scoring.
Provided image
CLINICAL PEARL
The 'too-sick-for-dates' triad is your diagnostic alarm for molar pregnancy: hyperemesis that seems excessive for gestational age, blood pressure elevation before 20 weeks (pseudo-pre-eclampsia), or a uterus that measures two or more weeks larger than expected — ANY one of these in the first or early second trimester should trigger an immediate quantitative β-hCG and pelvic ultrasound. In resource-limited settings, a β-hCG level clearly above the expected gestational range combined with an ultrasound that shows no normal fetal pole is sufficient to justify suction evacuation and histopathology even without a formal reference laboratory cut-off for your setting. Never let the reassuring persistence of vaginal bleeding with some pregnancy material lull you into diagnosing a threatened abortion before excluding molar disease.
Self-Assessment: GTN Clinical Vignettes
The following two vignettes test your ability to apply the core clinical and surveillance skills from this module. Work through each scenario before reading the explanation.
Vignette A: A 30-year-old G2P1 at 13 weeks is referred with severe vomiting, 3 kg weight loss, and β-hCG of 520,000 mIU/mL. Ultrasound shows a uterus of 18 weeks size packed with cystic vesicular tissue, no fetal pole. Bilateral 7 cm ovarian cysts are noted. Your immediate priorities: (1) confirm diagnosis — snowstorm ultrasound pattern + very high β-hCG points to complete molar pregnancy; (2) check CXR for pulmonary metastases; (3) check TFTs (risk of thyroid storm); (4) arrange suction curettage under GA with oxytocin after dilatation; (5) send all tissue for histology; (6) begin weekly β-hCG surveillance from the day of evacuation; (7) prescribe OCP and counsel regarding follow-up protocol.
Vignette B: The same woman returns at week 5 of post-evacuation surveillance. Her β-hCG values are: Day 0 (evacuation): 520,000; Week 1: 180,000; Week 2: 95,000; Week 3: 88,000; Week 4: 91,000; Week 5: 93,000. What does this pattern indicate, and what is your next step?
The week 3–5 pattern shows a plateau (values fluctuate ±10% over three consecutive weekly assays). This meets the RCOG criterion for GTN. The patient must be referred immediately to a trophoblastic disease centre for FIGO staging, WHO prognostic risk scoring, and chemotherapy planning. Do NOT initiate chemotherapy without formal risk scoring. This is the exact scenario where your knowledge of the referral trigger saves a life — the oncologic management, including whether she receives single-agent methotrexate or multi-agent EMA/CO, is determined in OG34.3.
SELF-CHECK
After suction evacuation of a complete hydatidiform mole, a woman's weekly β-hCG values are: Week 1: 90,000; Week 2: 42,000; Week 3: 38,000; Week 4: 41,000; Week 5: 43,000 mIU/mL. What is the correct interpretation and action?
A. Normal post-evacuation decline; continue surveillance as scheduled
B. β-hCG plateau meeting GTN criteria; refer to trophoblastic disease centre for staging and treatment
C. β-hCG is falling rapidly; discharge after one more undetectable value
D. Repeat the β-hCG in two weeks before making a decision
Reveal Answer
Answer: B. β-hCG plateau meeting GTN criteria; refer to trophoblastic disease centre for staging and treatment
Weeks 3-5 show a β-hCG plateau: the value has not declined by >10% between consecutive weekly assays (38,000 → 41,000 → 43,000 represents fluctuation less than 10% decline and actually a small rise). By RCOG criteria, a plateau or rise over three consecutive weekly assays after evacuation is diagnostic of GTN and mandates immediate referral to a trophoblastic disease centre for FIGO staging, WHO prognostic scoring, and chemotherapy. Waiting two more weeks is inappropriate once the plateau criterion is met; the pattern already satisfies the referral trigger.