Page 10 of 17
OG11.1 | Multiple Pregnancy — SDL Guide (Part 2)
Complications of Multiple Pregnancy
Multiple pregnancy is a high-risk condition because both the maternal physiology and the fetal environment are pushed well beyond the adaptations that evolved for singleton pregnancy. The mother must sustain two placentas, two fetal circulations, and a uterine volume that in twin pregnancy at term may reach the equivalent of a 40-week singleton. The result is a concentration of obstetric complications — both maternal and fetal — that makes multiple pregnancy one of the highest-risk categories in antenatal care. These complications are not randomly distributed: some are general to all multiple pregnancies (anaemia, preterm labour, PPH), while others are specific to monochorionic twins whose shared placentation creates unique pathophysiology (TTTS, selective IUGR, cord entanglement). Understanding this distinction between general and chorionicity-specific complications is the framework for appropriate risk stratification and targeted surveillance. The uterus is overdistended, the placental mass is larger, the nutritional demands are double, and in monochorionic twins, the shared placental circulation introduces complications unique to this anatomy. Understanding these complications by category — maternal versus fetal, and chorionicity-specific versus general — is the key to anticipating and preventing them.
Maternal complications:
- Anaemia: Iron and folate demands are doubled; anaemia complicates up to 40–50% of twin pregnancies. Supplement with higher-dose iron (60 mg elemental iron twice daily) and folic acid 5 mg/day.
- Hyperemesis gravidarum: More severe nausea and vomiting due to higher hCG levels.
- Gestational diabetes (GDM): Risk is significantly higher than singleton; screen early and at 24–28 weeks.
- Hypertensive disorders (PIH/pre-eclampsia): Twice as common in twins; earlier onset and more severe. Monitor BP fortnightly from 20 weeks.
- Antepartum haemorrhage (APH): Placenta praevia and abruption are more common (larger placental mass, overdistended uterus).
- Postpartum haemorrhage (PPH): Major complication — uterine overdistension → atony after delivery is the dominant mechanism. Prepare blood products and active management of third stage.
- Preterm labour and delivery: Complicates 50% of twin pregnancies; preterm birth before 34 weeks in ~25%. Cervical surveillance by USS (cervical length ≤25 mm at 20–24 weeks = high risk).
- Polyhydramnios: Especially with the recipient twin in TTTS.
- Operative delivery: CS rate is significantly higher in twin pregnancies.
Fetal complications:
- Prematurity: Most important fetal complication; responsible for the majority of perinatal deaths in twins. Mean gestational age at delivery for twins is ~37 weeks; for triplets ~34 weeks.
- Fetal growth restriction (FGR/IUGR): Selective IUGR (sIUGR) in MCDA twins due to unequal placental sharing; affects ~10–15% of MCDA pregnancies. Defined as estimated fetal weight <10th centile in one twin with birthweight discordance ≥25%.
- Congenital anomalies: More common in MZ twins (especially MCDA/MCMA); include neural tube defects, cardiac anomalies.
- Twin-to-twin transfusion syndrome (TTTS): See below — specific to MC twins.
- Cord entanglement: Specific to MCMA twins — both fetuses in the same sac, cords entwine, causing acute fetal compromise.
- Acardiac twin (TRAP sequence): One twin (pump twin) perfuses an acardiac, often acephalic co-twin via reverse arterial perfusion; the pump twin is at risk of cardiac failure. Rare.
Twin-to-twin transfusion syndrome (TTTS):
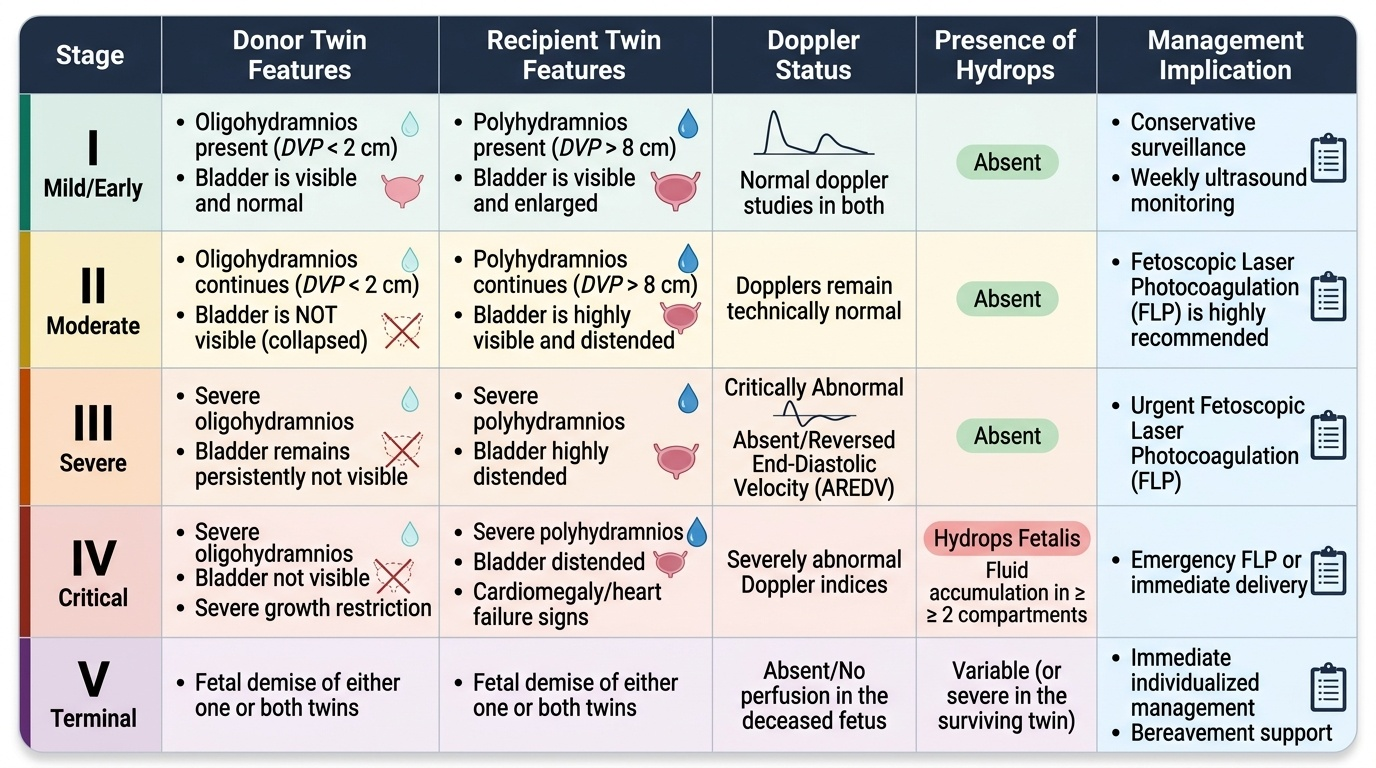
TTTS occurs exclusively in monochorionic twins (shared placenta with arteriovenous anastomoses). Blood flows preferentially from the donor twin (who becomes anaemic, growth-restricted, oligo/anuric — producing oligohydramnios) to the recipient twin (who becomes polycythaemic, volume-overloaded, polyuric — producing polyhydramnios). The imbalance is progressive and, untreated, carries 80–100% fetal mortality. The Quintero staging system (1999) classifies severity:
- Stage I: Discordant amniotic fluid volumes (donor oligohydramnios, recipient polyhydramnios) — donor bladder still visible.
- Stage II: Donor bladder not visible on USS (collapsed/absent — oliguria).
- Stage III: Critically abnormal Doppler in either twin (absent/reversed end-diastolic flow in donor UA, or pulsatile UV/reversed DV ductus venosus in recipient).
- Stage IV: Hydrops fetalis in recipient (fluid in two or more cavities — ascites, pleural effusion, pericardial effusion, skin oedema).
- Stage V: Death of one or both twins.
Treatment: Fetoscopic laser ablation of placental vascular anastomoses is the treatment of choice for Stages II–IV (and selected Stage I). Senat et al. (NEJM 2004) demonstrated significantly better survival and neurodevelopmental outcome with laser ablation versus amnioreduction alone. Amnioreduction alone is used for palliative/bridging in settings where laser is unavailable.
Provided image
SELF-CHECK
In a 24-week MCDA twin pregnancy, serial USS shows the donor twin has collapsed bladder on USS, amniotic fluid index of 2 cm (severe oligohydramnios), and absent end-diastolic flow on umbilical artery Doppler. The recipient twin has a deepest vertical pocket of 10 cm (polyhydramnios) and a distended bladder. What Quintero stage is this?
A. Stage I — discordant fluid volumes only
B. Stage II — absent donor bladder, discordant fluid
C. Stage III — critically abnormal Doppler in donor twin
D. Stage IV — hydrops in recipient twin
Reveal Answer
Answer: C. Stage III — critically abnormal Doppler in donor twin
This is Quintero Stage III TTTS: there is absent donor bladder (Stage II criterion met) AND critically abnormal Doppler — absent end-diastolic flow in the donor twin's umbilical artery (Stage III criterion). The Quintero stage is the highest stage met, so this is Stage III. Hydrops is not present (Stage IV). Stage III mandates urgent referral for fetoscopic laser ablation, as the fetal prognosis without treatment is very poor.
Antenatal Surveillance and Management Principles
The antenatal management of multiple pregnancy is stratified by chorionicity, because the risk profile differs so fundamentally between dichorionic and monochorionic twins that a single undifferentiated surveillance plan would both over-investigate low-risk DCDA pregnancies and fatally under-investigate high-risk MCDA ones. The entire NICE NG137 guideline (2019) is built around this chorionicity-stratified approach: DCDA twins receive 4-weekly growth scans and deliver at 38 weeks, while MCDA twins require fortnightly surveillance from 16 weeks and deliver at 36–37 weeks because their shared placenta ages faster and TTTS can develop within days. MCMA twins, sharing both placenta and amniotic cavity, require inpatient admission from 28 weeks because cord entanglement can cause sudden fetal death at any moment. These three management frameworks must be committed to memory as a unit — they are inseparable from the chorionicity classification. The goal is to detect the chorionicity-specific complications at the earliest reversible stage — growth restriction, TTTS, and abnormal Doppler — while also managing the maternal complications that are common to all multiple pregnancies.
General principles for all multiple pregnancies:
- Higher nutritional supplementation: Elemental iron 60 mg twice daily, folic acid 5 mg/day throughout pregnancy.
- Frequent antenatal visits: Every 2–4 weeks from 20 weeks onward (more frequent than singletons).
- Cervical length surveillance: Transvaginal USS cervical length at 20–24 weeks; cervical length ≤25 mm is a high-risk indicator for preterm birth.
- Corticosteroids: Betamethasone course if preterm birth is anticipated <34 weeks.
- GDM screen at booking and 24–28 weeks.
- BP and urine monitoring for pre-eclampsia.
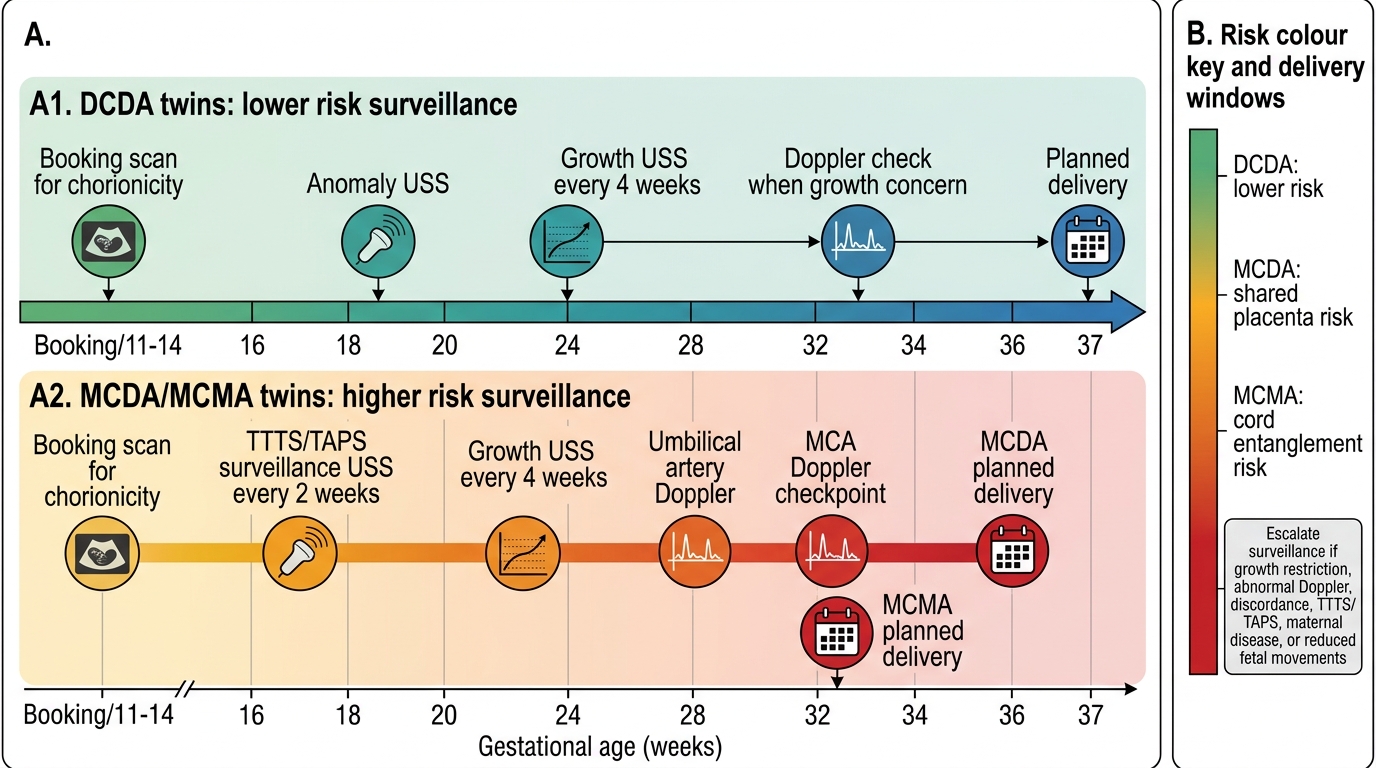
Surveillance schedule by chorionicity (NICE NG137, 2019):
Dichorionic-diamniotic (DCDA) twins:
- USS for growth and amniotic fluid every 4 weeks from 20 weeks.
- Umbilical artery Doppler from 24 weeks.
- Planned elective delivery at 38 weeks (uncomplicated) — beyond this, placental insufficiency risk rises sharply in twins.
Monochorionic-diamniotic (MCDA) twins:
- USS every 2 weeks from 16 weeks — intensive surveillance because TTTS can develop rapidly.
- Umbilical artery Doppler and middle cerebral artery (MCA) Doppler every 2 weeks.
- Planned delivery at 36–37 weeks (uncomplicated) — does not wait until 38 weeks because monochorionic placenta ages faster.
- Refer to fetal medicine centre with laser ablation capability from 16 weeks.
Monochorionic-monoamniotic (MCMA) twins:
- Inpatient admission from ~28–30 weeks for continuous CTG monitoring (cord entanglement can cause sudden fetal death at any time).
- Planned delivery at 32–34 weeks by elective CS (vaginal delivery is hazardous with intertwined cords).
TTTS management:
- Stages II–IV: Fetoscopic laser photocoagulation (FLP) of equatorial placental anastomoses — treatment of choice, performed at fetal medicine centres. Target: laser the communications between donor and recipient at the equatorial zone of the placenta.
- Stage I: Controversial — close surveillance vs early laser; managed case-by-case.
- Amnioreduction: Temporary measure; reduces recipient polyhydramnios and intrauterine pressure; used in centres without laser capability or as bridging therapy.
Chorionicity-Specific Surveillance in Twin Pregnancy
Intrapartum and Delivery Management
The timing and mode of delivery in multiple pregnancy are among the most consequential decisions in obstetrics, requiring a careful balance between the increasing risks of continuing the pregnancy — placental insufficiency, intrauterine death, cord complications, and escalating maternal PPH risk — against the risks of iatrogenic prematurity from delivering too early. The evidence base, synthesised in NICE NG137 and RCOG guidelines, recommends planned delivery at gestation-specific windows for each chorionicity category, with vaginal delivery reserved for pregnancies where twin 1 is cephalic and the clinical environment is fully prepared for twin birth complications. These complications, particularly the management of twin 2 after delivery of twin 1, require an experienced obstetrician who can perform internal podalic version and breech extraction — skills that are not universal in every obstetric unit and that must be anticipated at the time of delivery planning. The planned delivery gestation differs by chorionicity because DCDA twins tolerate pregnancy longer than MC twins. In all cases the aim is to deliver at the optimal gestation with a prepared team, appropriate monitoring, and blood products available — because multiple pregnancy carries substantially higher risk of PPH.
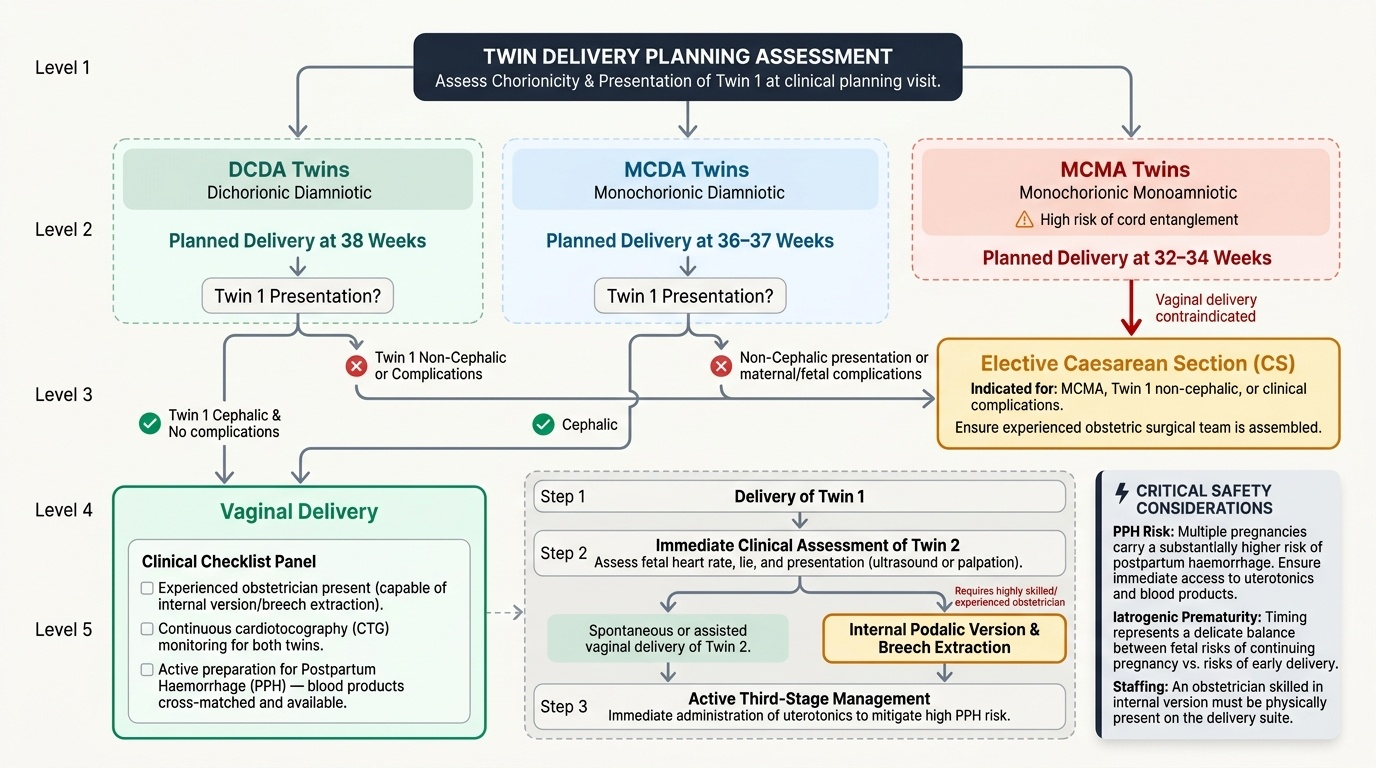
Planned delivery timing (uncomplicated pregnancies):
- DCDA: Elective delivery at 38 weeks (vaginal or CS depending on presentation).
- MCDA: Elective delivery at 36–37 weeks (vaginal if twin 1 is cephalic; CS if non-cephalic or complicated).
- MCMA: Elective CS at 32–34 weeks (vaginal delivery is contraindicated — cord entanglement makes it too dangerous).
- Higher-order multiples (triplets+): CS at 35 weeks or earlier depending on complications.
Mode of delivery — twin birth decisions:
- Twin 1 cephalic presentation: Vaginal birth can be planned for DCDA and uncomplicated MCDA; continuous CTG monitoring of both twins is mandatory; experienced obstetrician and anaesthetist in attendance; theatre available immediately.
- Twin 1 non-cephalic (breech or transverse): Elective CS recommended — the presenting part cannot engage or descend effectively and cord prolapse risk is high.
- Twin 2 management after twin 1 delivery: This is the critical phase. Twin 2 can undergo: (a) spontaneous cephalic vaginal delivery if engaged; (b) internal podalic version (IPV) + breech extraction if transverse lie; (c) external cephalic version (ECV) if time permits; (d) emergency CS if fetal distress occurs. The risk of fetal hypoxia rises after delivery of twin 1 — prompt management is essential.
Absolute indications for CS in twins:
- MCMA pregnancy (cord entanglement risk).
- Conjoined twins.
- Both twins non-cephalic.
- Locked twins (extremely rare — twin 1 breech, twin 2 cephalic, chins interlock).
- Complicated MCDA (TTTS after laser ablation, sIUGR, one fetal death).
Intrapartum monitoring:
- Continuous CTG of both fetal heart rates simultaneously (twin CTG).
- IV access and group-and-screen (crossmatch in high-risk cases) on admission.
- Epidural anaesthesia recommended to allow manipulation of twin 2 if needed.
- Prepare oxytocin infusion, ergometrine (if not hypertensive), and blood products for post-delivery PPH management.
Provided image
SELF-CHECK
A 36-week MCDA uncomplicated twin pregnancy is planned for delivery. Twin 1 is cephalic. What is the recommended mode and timing of delivery?
A. Emergency CS immediately — all monochorionic twins require CS regardless of presentation
B. Await spontaneous labour at 40 weeks — no early intervention needed for uncomplicated MCDA
C. Planned delivery (vaginal or CS based on presentation) at 36–37 weeks — she is at the appropriate gestation
D. Inpatient admission now with continuous CTG and CS at 32–34 weeks — MCDA requires this protocol
Reveal Answer
Answer: C. Planned delivery (vaginal or CS based on presentation) at 36–37 weeks — she is at the appropriate gestation
Uncomplicated MCDA twins are planned for delivery at 36–37 weeks (NICE NG137). She is at 36 weeks — this is the appropriate gestation for planned delivery. Twin 1 is cephalic, so vaginal delivery can be planned (with an experienced team and theatre standby), though CS may still be chosen based on local protocols or patient preference. Waiting until 40 weeks is unsafe — MCDA placentas have higher risk of insufficiency and fetal demise beyond 37 weeks. Continuous inpatient CTG and CS at 32–34 weeks is the protocol for MCMA (monoamniotic), not MCDA.
CLINICAL PEARL
Three high-yield points about multiple pregnancy that are frequently examined:
- Chorionicity, not zygosity, determines risk. A pair of DZ twins (always DCDA) is lower risk than a pair of MZ twins who split late and are MCMA. The question 'are they identical?' is far less important clinically than 'how many placentas?' First-trimester USS (lambda vs T-sign) is the only reliable way to answer the latter.
- TTTS occurs ONLY in monochorionic twins. It cannot occur in DCDA pregnancies because there are no shared vascular anastomoses. Whenever you see a question about TTTS, check the chorionicity first — if the twins are DCDA, TTTS is the wrong diagnosis regardless of the amniotic fluid discordance description.
- PPH is greatly amplified in multiple pregnancy. The combination of uterine overdistension (atony), a larger placental bed, and higher likelihood of preterm delivery (placenta praevia, abruption) makes PPH the leading obstetric emergency after twin delivery. Active management of the third stage — oxytocin 10 IU IM — is mandatory, and blood products should be available for all twin deliveries.