Page 11 of 17
OG11.1 | Multiple Pregnancy — SDL Guide (Part 3)
Self-Assessment
You have now worked through the full clinical arc of multiple pregnancy: from the epidemiology and rising incidence driven by ART, through the mechanistic basis of chorionicity and its determination by first-trimester USS (lambda vs T-sign), to the full spectrum of maternal and fetal complications — particularly twin-to-twin transfusion syndrome with its Quintero staging system and the evidence basis for fetoscopic laser ablation — and the chorionicity-specific surveillance schedules and delivery protocols that constitute modern management. This is a topic that rewards systematic recall: the chorionicity classification is a branching tree from which every complication, every surveillance frequency, and every delivery gestation follows. When revising, anchor your recall to that tree — DCDA at the bottom (safest, 38 weeks), MCDA in the middle (TTTS risk, 36–37 weeks), MCMA at the apex (cord entanglement, 32–34 weeks CS). The self-assessment questions below cover the most-tested aspects: the lambda and T-sign distinction, the Quintero staging criteria, the appropriate delivery gestation by chorionicity, and the specific complications associated with monochorionic versus dichorionic placentation. Work through each question independently before reading the explanation, and use errors as a guide to which sections to revisit.
Key concepts to revisit:
- Lambda sign = DCDA; T-sign = MCDA — determined at 11–14 weeks
- Chorionicity determines risk, not zygosity
- TTTS Quintero Stages I–V: what moves the stage up, and when is laser indicated
- Delivery timing: DCDA 38 wks, MCDA 36–37 wks, MCMA 32–34 wks (CS)
- PPH risk in twins: prepare blood products for every twin delivery
- MCMA: cord entanglement, inpatient monitoring from 28–30 weeks
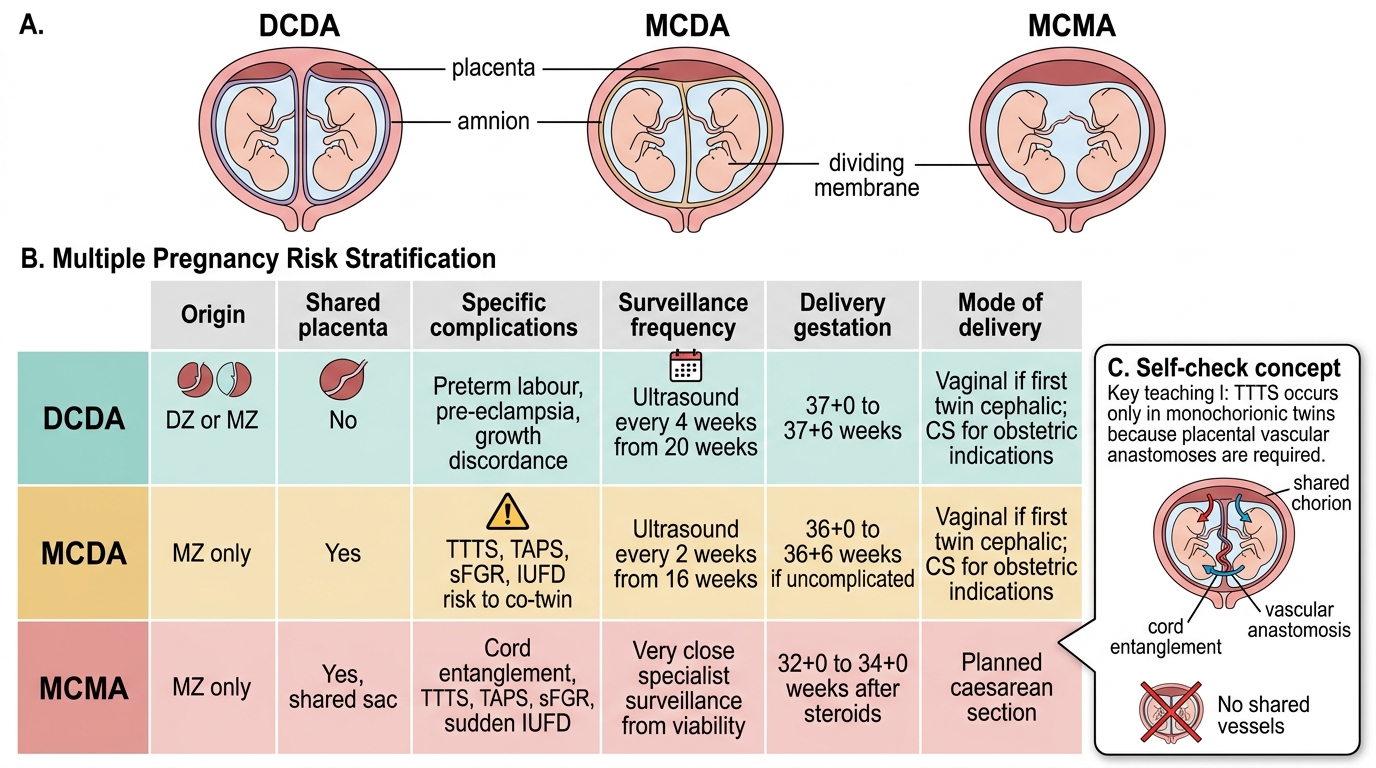
Multiple Pregnancy Risk Stratification
SELF-CHECK
Which of the following complications occurs EXCLUSIVELY in monochorionic twin pregnancies and CANNOT occur in dichorionic-diamniotic (DCDA) twins?
A. Pre-eclampsia
B. Preterm labour
C. Twin-to-twin transfusion syndrome (TTTS)
D. Gestational diabetes
Reveal Answer
Answer: C. Twin-to-twin transfusion syndrome (TTTS)
TTTS requires arteriovenous anastomoses between the two fetal circulations — connections that only exist in a shared (monochorionic) placenta. In DCDA pregnancies, each twin has its own placenta with no vascular connections to the co-twin's circulation. Pre-eclampsia, preterm labour, and GDM can all occur in both DCDA and monochorionic pregnancies — they are not chorionicity-specific.